Sarcina ventriculi Bacteremia Complicating Aspiration Pneumonia: A Case Report
Shogo Saito, Yusuke Sasaki, Hiromi Nagashima, Tohru Fujiwara, Kiwamu Nakamura

TL;DR
This case report describes a rare instance of Sarcina ventriculi bacteremia in an elderly man with aspiration pneumonia.
Contribution
The paper presents the first reported case of S. ventriculi bacteremia linked to a lower respiratory tract infection.
Findings
S. ventriculi was detected in blood cultures and sputum of an 89-year-old man with aspiration pneumonia.
The patient recovered after treatment with ceftriaxone.
Literature review found only three prior cases of S. ventriculi bacteremia, all linked to the gastrointestinal tract.
Abstract
Sarcina ventriculi, a large anaerobic Gram-positive coccus that clusters in tetrads, is most commonly detected histologically in gastric biopsy specimens from patients with gastrointestinal disorders. Herein, we describe a rare case of bacteremia caused by S. ventriculi in an 89-year-old man. The patient had a history of cerebral infarction, atrophic gastritis, and chronic obstructive pulmonary disease and was receiving home oxygen therapy. He was admitted to our hospital with a right femoral neck fracture. Three days after femoral surgery, he developed aspiration pneumonia, and S. ventriculi was detected in the anaerobic blood culture bottle. A Gram-stained sputum smear showed large Gram-positive cocci (presumed to be S. ventriculi) clustered in tetrads. The patient was diagnosed with S. ventriculi bacteremia as a complication of aspiration pneumonia and recovered after ceftriaxone…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
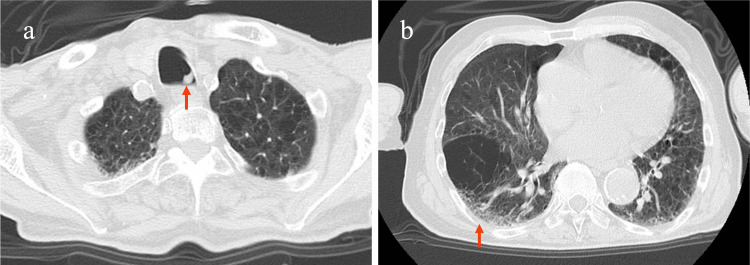 Figure 1
Figure 1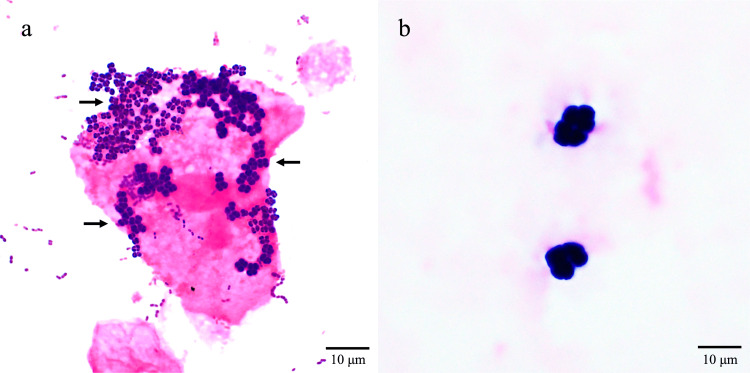 Figure 2
Figure 2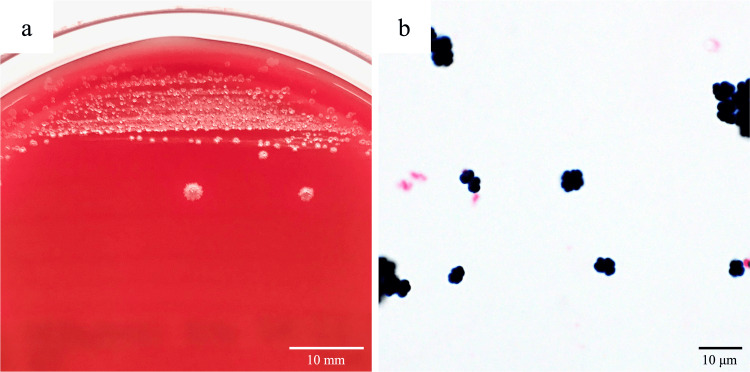 Figure 3
Figure 3| Test (units) | Result | Reference range |
| White blood cells (× 109/L) | 7.3 | 3.3-8.6 |
| Red blood cells (× 1012/L) | 2.67 | 4.35-5.55 |
| Hemoglobin (g/L) | 86 | 137-168 |
| Platelets (× 109/L) | 112 | 158-348 |
| Total protein (g/L) | 46 | 66-81 |
| Albumin (g/L) | 20 | 41-52 |
| Urea nitrogen (mmol/L) | 5.7 | 2.7-7.1 |
| Creatinine (µmol/L) | 53 | 58-94 |
| C-reactive protein (mg/L) | 219.1 | <1.4 |
| Reference (year) | Country | Age, sex | Underlying diseases | Suspected infection source | Positive blood culture in submitted blood culture set* |
Other samples containing | Antimicrobial therapy | Outcome |
|
Bortolotti et al. [ | France | 65, M | Cardiac failure, ileocecal resection for acute colonic pseudo-obstruction | Gastrointestinal tract | One anaerobe bottle in one set | ND | IV VCM for five days and IV PIPC/TAZ for 10 days | Survived |
|
Tuuminen et al. [ | Finland | 48, F | Congenital chloride diarrhea | Gastrointestinal tract | One anaerobe bottle in one set | ND | Oral AMPC for five days | Survived |
|
Elvert et al. (2018) [ | USA | 33, F | Medullary sponge kidney | Gastrointestinal or urogenital tract | One anaerobe bottle in one set | ND | Oral LVFX for 14 days | Survived |
| This case | Japan | 89, M | Past cerebral infarction, atrophic gastritis, COPD | Lower respiratory tract (aspiration pneumonia) | One anaerobe bottle in one set |
| IV CTRX for five days | Survived |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAnimal health and immunology · Viral gastroenteritis research and epidemiology · Congenital Anomalies and Fetal Surgery
Introduction
Sarcina ventriculi is an anaerobic Gram-positive coccus belonging to the Clostridiaceae family [1]. *Sarcina *spp. are found as commensals in soil and human feces, especially in vegetarians [2]. S. ventriculi is most commonly detected in patients with gastroesophageal content stasis due to gastric outlet obstruction, gastroparesis, or delayed gastric emptying [3]. It is found primarily in the stomach, followed by the esophagus and duodenum. The severity of cases of infection varies, ranging from asymptomatic to life-threatening [4]. In severe cases, complications such as hemodynamic instability secondary to emphysematous gastritis and gastric perforation can occur [5]. It is primarily identified through histopathology of the gastrointestinal tract and is rarely detected using microbiological tests such as blood culture or sputum microscopy. The typical morphological features of S. ventriculi on Gram staining are useful for identification, but the identity must be confirmed using molecular techniques. Few cases of S. ventriculi bacteremia have been reported. Herein we report a unique case of S. ventriculi bacteremia that occurred as a complication of aspiration pneumonia and provide a brief literature review of S. ventriculi as a human pathogen.
Case presentation
The patient was an 89-year-old man with a height of 160.0 cm and a weight of 51.8 kg, who had experienced a cerebral infarction 15 years previously. He had been taking cilostazol and mosapride citrate tablets for atrophic gastritis and receiving home oxygen therapy (2 L/min nasally) for chronic obstructive pulmonary disease (COPD). He visited the emergency room because of the acute onset of weakness in his right leg, which had started several hours previously. He was admitted to our hospital with a right femoral neck fracture. On admission, the patient’s vital signs were as follows: Glasgow Coma Scale: E4V5M6; blood pressure: 139/82 mmHg; heart rate: 74 beats/min; body temperature: 36.9°C; respiratory rate: 16 breaths/min; and peripheral oxygen saturation: 93% breathing 2 L/min oxygen via nasal prongs. Bipolar hip arthroplasty was performed on day 3 of hospitalization. On day 6, he became febrile and expectorated copious amounts of sputum. At that time, his body temperature was 39.6°C, his respiratory rate was 28 breaths/min, and his peripheral oxygen saturation had decreased to 80%, breathing 2 L/min oxygen via nasal prongs. His hematology and serum biochemistry test results are shown in Table 1.
Chest CT revealed aspirated sputum in the main bronchus (Figure 1a), mild lung infiltration, and old lung damage caused by COPD (Figure 1b).
Chest CT of the patientChest CT shows (a) aspirated sputum in the main bronchus (red arrow) and (b) mild lung infiltration (red arrow) with underlying lung damage caused by COPD.COPD, chronic obstructive pulmonary disease
Sputum, urine, and blood samples were submitted for microbiological testing. The Miller and Jones visual classification of the sputum sample was P3, and sputum smears were determined to be class 3 according to the Geckler classification, both indicating purulent sputum. Large Gram-positive cocci clustered in tetrads were present in the sputum (Figure 2a), clearly distinguishable from staphylococci. No significant bacteria were detected on the urine culture. Two sets of blood culture samples were obtained using BD BACTEC Plus Aerobic/F and Anaerobic/F blood culture bottles (Becton, Dickinson and Company, Franklin Lakes, NJ, USA), with approximately 10 mL of blood added to each bottle. The blood culture bottles were promptly transported to the microbiological laboratory and incubated in the BD BACTEC FX blood culture system for five days at 35°C. The anaerobic blood culture bottle showed a positive signal at 47 hours. Gram staining of the blood culture revealed large Gram-positive cocci in clusters of tetrads with difficulty in obtaining a clear focus on microscopy owing to their large size (Figure 2b), morphologically similar to the Gram-positive bacteria that had been seen in the sputum (Figure 2a).
Gram-stained sputum and blood smears showing the appearance of Sarcina ventriculi on microscopy(a) Sputum smear showing large Gram-positive cocci in clusters of tetrads (black arrows; magnification ×1,000). (b) Gram-stained blood smear sample obtained from a positive anaerobic blood culture bottle after 47 hours of culture showing large Gram-positive clusters of tetrads (magnification ×1,000). Due to the large size of the Gram-positive clusters of tetrads, clear focus could not be achieved. The samples were collected immediately prior to initiating antibiotic treatment.
As no potential infectious source other than the respiratory tract was identified, the patient was diagnosed with bacteremia and aspiration pneumonia, and ceftriaxone (CTRX) 2 g daily was initiated. His fever resolved two days after starting CTRX, and his respiratory function recovered to the pre-admission level. He was treated with CTRX for five days and was discharged without further complications.
During bacterial isolation from blood cultures, irregular-shaped, grayish colonies with ragged edges were cultured on Brucella HK agar (RS) (Kyokuto Pharmaceutical Industrial Co., Ltd., Tokyo, Japan) after 48 hours of incubation at 35°C (Figure 3).
Appearance of Sarcina ventriculi colonies on Brucella HK agar and bacterial morphology on Gram staining(a) Characteristic irregular-shaped, grayish colonies with ragged edges of S. ventriculi growing on Brucella HK agar. The colonies were cultured from a blood culture sample plated on Brucella HK agar and incubated at 35°C for 48 hours under anaerobic conditions. (b) Microscopic image of Gram-stained S. ventriculi grown on Brucella HK agar (magnification ×1,000).
Similar colonies were cultured on phenylethyl alcohol-supplemented Brucella HK agar, but not on paromomycin-vancomycin (VCM)-supplemented Brucella HK agar or Bacteroides Bile Esculin agar (Kyokuto Pharmaceutical Industrial Co., Ltd., Tokyo, Japan). Identification using matrix-assisted laser desorption ionization-time of flight mass spectrometry (MALDI-TOF MS) with the MALDI Biotyper Microflex LT/SH (Bruker Daltonics GmbH & Co. KG, Bremen, Germany) and MBT Compass Library 2023 Revision P confirmed *Sarcina sp. (score value 1.80). Species-level identification was performed using 16S rDNA sequencing by amplifying a 1,447-bp DNA fragment using universal primers 27F and 1492R. The DNA sequence analysis showed 99.65% identity with S. ventriculi (DSM 286) 16S rRNA gene (GenBank accession number X76649), and 100% identity with S. ventriculi *16S ribosomal RNA gene, complete sequence (GenBank accession number AF110272), confirming its identity as S. ventriculi [6]. A test for β-lactamase production using BD BBL Cefinase paper discs (Becton, Dickinson and Company) was negative. Antimicrobial susceptibility testing was performed using Brucella broth and Dry Plate Eiken DP1R (Eiken Chemical Co., Ltd., Tokyo, Japan), incubated under anaerobic conditions at 36°C ± 1°C for five days, which revealed minimum inhibitory concentrations (MICs) of ≤0.5 µg/mL for minocycline, levofloxacin, moxifloxacin, and clindamycin (CLDM), and ≤2 µg/mL for metronidazole (MNZ), confirming CLDM and MNZ susceptibility according to the CA-SFM 2019 guidelines [7]. However, the MICs of β-lactams were variable and were classified as indeterminate after five independent tests.
Discussion
S. ventriculi was first described in 1842 after being found in the stomach contents of a patient with vomiting [8]. The individual bacteria are large (1.8-3 μm in diameter) compared with staphylococci (~1 μm in diameter) [3]. The name comes from the Latin “sarcina” meaning “package” or “bundle,” and the bacteria typically clustered in tetrads or octets [9]. The number of bacterial cells per cluster can reach several hundred [10]. Likewise in this case, the Gram-stained smear from the blood culture bottle revealed distinctly large Gram-positive cocci, clearly distinguishable from the stained smear from staphylococci. Furthermore, the characteristic appearance of irregular-shaped, grayish colonies with ragged edges also helps to identify *Sarcina *spp. As a colonizer of the stomach and upper intestinal tract, *S. ventriculi *is well adapted to acidic environments. In low pH (acidic) environments, it exhibits characteristic square or cuboidal cell arrangements, whereas in high pH (alkaline) environments, it exhibits distorted cell shapes and irregular arrangements, and spore formation is induced [11]. The correct nomenclature of this species has been a source of debate. In addition to the two historical species names, *S. ventriculi and Zymosarcina ventriculi, a reclassification based on 16S rRNA phylogeny proposed that the species be transferred to Clostridium ventriculi [10,12]. However, the proposal was ultimately rejected, and the correct name for this bacterial species remains S. ventriculi *[13]. Other species of the genus *Sarcina *include Sarcina maxima, which has also been detected in human feces [14]. Only one Sarcina sp. strain is registered in the MALDI-TOF MS library (MBT Compass Library 2023 Revision P). Therefore, 16S rDNA sequencing is required to identify S. ventriculi at the species level, as in this study.
No standard method has been established for antimicrobial susceptibility testing of S. ventriculi. In a previous report, its antimicrobial susceptibility was determined by the broth dilution method using Brucella broth under anaerobic conditions at 35°C ± 2°C for 48 ± 4 hours according to the CA-SFM 2019 guidelines [7]. Antibiotic susceptible breakpoints in the guidelines were set as follows: penicillin G: 0.25 mg/L; amoxicillin (AMPC): 4 mg/L; AMPC/clavulanic acid: 4/2 mg/L; piperacillin (PIPC): 16 mg/L; PIPC/tazobactam (TAZ): 8/4 mg/L; ticarcillin: 16 mg/L; ticarcillin/clavulanic acid: 8/2 mg/L; ertapenem: 0.5 mg/L; imipenem: 2 mg/L; meropenem: 2 mg/L; VCM: 2 mg/L; CLDM: 4 mg/L; linezolid: 2 mg/L; tigecycline: 4 mg/L; rifampicin: 4 mg/L; MNZ: 4 mg/L; and chloramphenicol: 8 mg/L [7]. In this study, antimicrobial susceptibility testing was also performed according to the CA-SFM 2019 guidelines. Owing to the slow growth of the bacteria, the incubation period was extended to five days. We were unable to determine the MICs of β-lactam antibiotics, which were variable and were classified as indeterminate. Therefore, a modified culture method is required for the determination of the MICs of β-lactam antibiotics. However, MICs for MINO, quinolones, CLDM, and MNZ were consistently low. The isolate was interpreted as susceptible to CLDM and MNZ according to the CA-SFM 2019 guidelines [7]. Considering the patient’s clinical course and previous cases, CTRX could be an effective option for treating *S. ventriculi *bacteremia.
A systematic review reported that S. ventriculi has been isolated from the gastrointestinal tract (88%), respiratory tract (5%), urine (4%), and blood (3%) [9]. Various antibiotics and other gastrointestinal agents have been used for the treatment of S. ventriculi infections [9]. Regarding the pathogenic roles of S. ventriculi, it has been detected in both clinically stable patients with gastrointestinal symptoms and in patients with life-threatening conditions such as emphysematous gastritis or gastric perforation [4]. Common symptoms of S. ventriculi infection include abdominal pain, distention, nausea and vomiting, diarrhea, and dyspepsia, but some cases are asymptomatic. Consequently, it is generally treated with gastrointestinal agents, with or without antibiotics, and gastric surgery is rarely required [9]. For the treatment of bacteremia, various antibiotics, including oral AMPC, LVFX, intravenous VCM and PIPC/TAZ, and CTRX (as in the current case), have been used (Table 2) [7,15-17].
In all previous case reports of bacteremia, the gastrointestinal tract was presumed to be the portal of entry, and the cases had favorable outcomes [7,15-17]. In this case, the patient developed aspiration pneumonia, and the characteristic bacterial morphology was observed in organisms in his sputum; therefore, we presume that *S. ventriculi *entered the patient’s blood via the lungs, which were damaged owing to severe COPD.
Conclusions
We described a unique case of bacteremia caused by S. ventriculi as a complication of aspiration pneumonia in a man with a history of cerebral infarction, atrophic gastritis, and COPD. S. ventriculi is a rare cause of bacteremia. A literature review revealed only three previous case reports of S. ventriculi bacteremia. In previous case reports, the gastrointestinal tract was the presumed portal of entry into the blood. To our knowledge, S. ventriculi bacteremia has not previously been reported as a complication of lower respiratory tract infection. This case suggests that the respiratory tract can serve as a portal of entry for* S. ventriculi* into the blood. Further case studies are required to improve understanding of the pathogenicity and optimal antimicrobial treatment of S. ventriculi.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Pathogenic Sarcina in urine BMJ Case Rep Bommannan K Gaspar BL Sachdeva MU 02016201610.1136/bcr-2016-216991 PMC 507369727737866 · doi ↗ · pubmed ↗
- 2Sarcina ventriculi in human faeces J Med Microbiol Crowther JS 34335041971511625510.1099/00222615-4-3-343 · doi ↗ · pubmed ↗
- 3Sarcina organisms in the gastrointestinal tract: a clinicopathologic and molecular study Am J Surg Pathol Lam-Himlin D Tsiatis AC Montgomery E 170017053520112199769010.1097/PAS.0b 013e 31822911 e 6PMC 3193598 · doi ↗ · pubmed ↗
- 4A rare case of Sarcina ventriculi of the stomach in an asymptomatic patient Int J Surg Pathol Haroon Al Rasheed MR Kim GJ Senseng C 1421452420162645367410.1177/1066896915610196 · doi ↗ · pubmed ↗
- 5Sarcina ventriculi a rare pathogen Autops Case Rep Marcelino LP Valentini DF Machado SM Schaefer PG Rivero RC Osvaldt AB 011202110.4322/acr.2021.337PMC 853053634692571 · doi ↗ · pubmed ↗
- 6Sarcina -like bacteria, Clostridium fallax and Clostridium sordellii in lambs with abomasal bloat, haemorrhage and ulcers J Comp Pathol Vatn S Tranulis MA Hofshagen M 19320012220001068468810.1053/jcpa.1999.0363 · doi ↗ · pubmed ↗
- 7Clostridium ventriculi bacteremia following acute colonic pseudo-obstruction: a case report Anaerobe Bortolotti P Kipnis E Faure E 32345920193110353010.1016/j.anaerobe.2019.05.005 · doi ↗ · pubmed ↗
- 8History of a case in which a fluid periodically ejected from the stomach contained vegetable organisms of an undescribed form Edinb Med Surg J Goodsir J Wilson G 430443571842 https://pubmed.ncbi.nlm.nih.gov/30330668/PMC 579129030330668 · pubmed ↗