Aggressive Postoperative Rehabilitation With Platelet-Rich Plasma Therapy for a Lauge-Hansen Supination-External Rotation Type IV Ankle Fracture: A Case Report of Early Return to Sports
Hiroyuki Omiya, Minami Kawamura, Shinnosuke Hada

TL;DR
A high school rugby player with a severe ankle fracture returned to sports quickly using surgery, PRP therapy, and aggressive rehab.
Contribution
Demonstrates early return to sports after SER type IV ankle fracture using PRP and accelerated rehabilitation.
Findings
Patient returned to competitive rugby within 8 weeks post-injury.
PRP therapy and early weight-bearing were associated with stable fracture healing.
One-year follow-up showed no pain or functional limitations.
Abstract
Supination-external rotation (SER) type IV ankle fractures, as classified by Lauge-Hansen (L-H), are highly unstable due to frequent injuries of the deltoid and distal tibiofibular ligaments. These fractures typically require open reduction and internal fixation (ORIF), followed by prolonged immobilization and delayed weight bearing. Such protocols often result in extended recovery periods, delaying the return to competitive sports. In the clinical setting, there is a growing demand for approaches that enable athletes to resume sports quickly. Platelet-rich plasma (PRP) therapy has demonstrated the potential to enhance bone and soft tissue healing. Although PRP is widely used in ligament and tendon injuries, PRP’s role in fracture rehabilitation is less well established, and it is often considered supplementary. We report the case of a 17-year-old male high school rugby player who…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1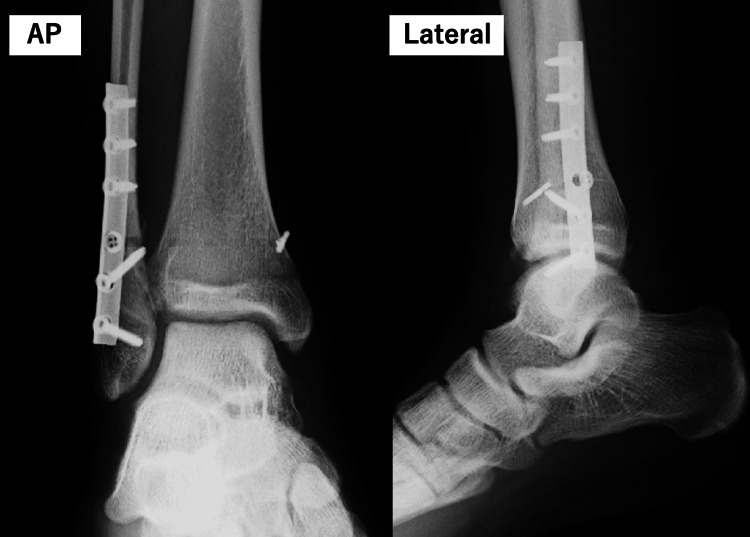 Figure 2
Figure 2| Postoperative week | Orthopedic assessment and procedures | Instructions from orthopedist | PT training (only changes highlighted) |
| Week 1-2 (days 0-14) | X-ray | Non-weight-bearing | PT not yet initiated |
| Cast immobilization | |||
| Week 3 (days 15-21) | X-ray/US | Full weight-bearing | Ultrasound therapy (3MHz, DUTY 50%) |
| Cast removal | Soft tissue mobilization | ||
| PRP therapy administered to the fracture site and ligaments | Active-passive ROM ex. | ||
| ROM: free | Towel gathering exercise | ||
| Seated calf raises | |||
| Week 4 (days 22-28) | X-ray/US | Resisted ankle joint training | Ultrasound therapy (3MHz, DUTY 100%) |
| Isometric inversion/eversion ankle training | |||
| Standing calf raises | |||
| Mini-squats | |||
| Week 5 (days 29-35) | X-ray/US/CT | Jogging and light agility training | Single-leg calf raises (isometric contraction) |
| Single-leg squats | |||
| Jogging | |||
| Week 6 (days 36-42) | X-ray/US | Sprinting | Single-leg calf raises (concentric and eccentric contraction) |
| Hydrodissection for EHL tendon | Light agility training | ||
| Week 7 (days 43-49) | No orthopedic consultation | Partial return to sport permitted | Single-leg single jumps |
| Week 8 (days 50-56) | X-ray/US | Full return to sport permitted | Single-leg continuous jumps |
| Hydrodissection for EHL tendon | Agility training |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsFoot and Ankle Surgery · Tendon Structure and Treatment · Orthopedic Surgery and Rehabilitation
Introduction
The Lauge-Hansen (L-H) classification of supination-external rotation (SER) type stage IV ankle fractures is characterized by significant instability due to the frequent involvement of deltoid ligament injuries and distal tibiofibular ligament damage. Open reduction and internal fixation (ORIF) is the recommended standard treatment, typically followed by prolonged weight-bearing restrictions and cast immobilization [1].
Standard rehabilitation protocols typically include two weeks of cast immobilization, weight-bearing initiation at six weeks, and functional recovery programs after 10 weeks [2,3]. However, these protocols often result in prolonged recovery periods, delaying the return to competitive sports. Prolonged immobilization and delayed weight-bearing can cause joint contractures, muscle atrophy, and hindered recovery, emphasizing the importance of early weight-bearing [4]. From the perspective of accelerating postoperative rehabilitation, several studies have demonstrated the potential benefits of autologous biotherapy in enhancing the healing process for various musculoskeletal injuries. Specifically, platelet-rich plasma (PRP), created by centrifuging a sample of a patient’s blood to isolate the platelets, has been gaining attention [5]. The treatment depends on the ability of growth factors and anti-inflammatory cytokines contained in platelets to promote the repair of damaged tissues.
PRP delivers growth factors such as platelet-derived growth factor (PDGF), transforming growth factor-beta (TGF-β), and vascular endothelial growth factor (VEGF), which collectively contribute to promoting cell proliferation and improving tissue regeneration [6,7]. Treatments utilizing platelets, including PRP, have proven effective in promoting fracture healing by activating mesenchymal progenitor cells and osteoblasts, with a randomized controlled trial reporting an 87.5% union rate using platelet-rich fibrin compared to 50% in the control group for open tibial fractures [6,7].
While PRP therapy has been increasingly used for muscle, tendon, and ligament injuries to support an early return to sports, its application in fracture rehabilitation, particularly in aggressive protocols for SER type stage IV ankle fractures, remains underexplored. Here, we report the case of a high school rugby player with an SER type stage IV ankle fracture who underwent aggressive rehabilitation combined with PRP therapy, aiming to contribute to the understanding of its potential for expedited recovery and early return to sports.
Written informed consent for academic use and publication of this data was obtained from the patient and is available upon request.
Case presentation
A 17-year-old male high school rugby player sustained a right ankle injury when tackled during a match while his foot was fixed. Radiographs obtained, showing the anteroposterior and lateral views on the day of injury, confirmed an L-H SER type IV ankle fracture (Figure 1). Eight days post-injury, ORIF was performed using a 1/3 tubular plate and the Ziptight system (Zimmer Biomet Holdings, Inc., Warsaw, Indiana, USA) (Figure 2). The patient and his family expressed a strong desire for an early return to rugby within eight weeks of surgery. After understanding the benefits and risks, they agreed to an aggressive rehabilitation protocol incorporating PRP therapy to support early recovery and weight-bearing.
Preoperative X-rays of the right anklePreoperative anteroposterior and lateral X-ray views of the right ankle demonstrating a SER type stage IV fracture as classified by L-H.L-H, Lauge-Hansen; SER, supination-external rotation
Postoperative X-rays of the right anklePostoperative anteroposterior and lateral X-ray views of the right ankle following ORIF. The fixation was performed using a 1/3 tubular plate and Ziptight system.ORIF, open reduction and internal fixation
Postoperatively, the patient underwent two weeks of cast immobilization and non-weight bearing. After two weeks (postoperative day 15), the cast was removed. PRP therapy was administered using the GPS III system (Zimmer Biomet Holdings, Inc., USA). The PRP was injected into both the fracture site and the surrounding injured ligaments, including the deltoid ligament and distal tibiofibular ligament, under ultrasound guidance to ensure precise delivery. Radiographic and ultrasonographic evaluations confirmed fracture stability without displacement and early callus formation. Based on these findings and the initiation of PRP therapy, full weight-bearing ambulation was permitted under close supervision, as part of a structured rehabilitation plan. The rehabilitation plan (Table 1) was designed to achieve the goal of returning to competitive rugby by the eighth postoperative week. At the time of cast removal, the range of motion (ROM) was 0° dorsiflexion and 30° plantar flexion, with pain localized below the lateral malleolus under partial weight-bearing.
The rehabilitation focused on enhancing soft tissue flexibility using ultrasound therapy and progressively strengthening the peri-ankle muscles. Ultrasound therapy was performed using the EU-910 device (Ito Co., Ltd., Japan). In the third postoperative week, ultrasound therapy aimed to reduce inflammation and promote early soft tissue repair through the thermal and non-thermal effects of ultrasound. This was conducted at a frequency of 3 MHz, a duty cycle of 50%, and an intensity of 1.0 W/cm². In the fourth week, therapy settings were adjusted to a 100% duty cycle to achieve an approximate 4°C increase in the temperature of the soft tissues, enhancing flexibility. Concurrently, soft tissue mobilization was performed to further improve flexibility and reduce adhesions. By the fifth postoperative week, full ROM was restored, and jogging was commenced upon achieving unilateral calf raises.
In the sixth postoperative week, restricted gliding movement of the extensor hallucis longus (EHL) tendon caused pain. To address this issue, a hydrodissection was performed by an orthopedic surgeon under ultrasound guidance. The surgeon evaluated the EHL tendon movement and identified specific areas of adhesion with surrounding tissues. A solution consisting of 1% lidocaine (3 mL) and 5% dextrose (7 mL) was injected into the adhesion sites. This procedure effectively released the adhesions, alleviated pain, and enabled a progressive increase in the intensity of rehabilitation.
By the eighth week, the patient was cleared for competitive rugby. At the one-year follow-up, the patient reported no pain, deformity, or functional limitations and participated in rugby at the pre-injury level without complications.
Discussion
Several factors contributed to the patient’s successful early return to competitive sports. The first was the implementation of aggressive rehabilitation through early postoperative weight-bearing. Porter et al. outlined a phased recovery program for distal tibiofibular ligament injuries: phase I (weeks 1-4) focuses on pain reduction and ROM improvement, phase II (weeks 4-8) emphasizes further ROM and strength recovery, and phase III (week 8 onward) targets functional activities [3]. In the present case, a condensed version of these phases facilitated early functional recovery with minimal complications. Although early weight-bearing is often avoided due to concerns about risks such as fragment displacement and ligament reinjury, studies have shown that it does not adversely affect surgical outcomes and may even accelerate functional recovery. Controlled loading of soft tissues, tailored to tissue conditions, optimizes recovery by enhancing metabolic activity, blood flow, and nutrient delivery, which supports cellular regeneration and collagen remodeling [8]. For example, early weight-bearing groups have demonstrated superior dorsiflexion (15° vs. 10°) and plantarflexion (35° vs. 25°) at six weeks, faster walking capacity (Timed Up and Go test: 12 s vs. 15 s), and reduced swelling compared with delayed weight-bearing groups [4].
Traditionally, radiographic detection of callus has been the standard for determining the progression of weight-bearing stages. However, in this case, ultrasonography, reported to detect callus formation 23% earlier than radiography, was also incorporated as an assessment tool, which facilitated the decision to initiate early weight-bearing [9].
The second factor was the use of PRP therapy. PRP therapy likely supported early inflammation resolution and tissue healing by delivering growth factors such as PDGF, TGF-β, and VEGF [6]. A previous study showed that PRP increased bone healing rates by 1.6-2.2 times in bone defects [10]. While PRP appears to be beneficial, its specific contribution is challenging to isolate owing to the multifactorial nature of rehabilitation. Further studies are required to validate their effectiveness in similar contexts.
This case suggests that combining aggressive postoperative rehabilitation with PRP therapy may facilitate an earlier return to sports for athletes with SER type stage IV ankle fractures. This approach has the potential to serve as an alternative to traditional rehabilitation protocols, which often result in delayed recovery. However, further studies involving larger patient populations and controlled trials are needed to confirm these findings.
Conclusions
Aggressive rehabilitation combined with PRP therapy allowed the patient to return to competitive rugby eight weeks post-surgery for an L-H SER type IV ankle fracture, with no complications or issues arising during the recovery process. In conclusion, this case demonstrates that combining aggressive postoperative rehabilitation with PRP therapy can facilitate an earlier return to sports for athletes with SER type stage IV ankle fractures. This approach may offer a promising alternative to traditional rehabilitation protocols, which often result in delayed recovery. Further investigation involving larger patient populations and controlled trials is essential to confirm these findings.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Treatment of medial malleolus or pure deltoid ligament injury in patients with supination-external rotation type IV ankle fractures Orthop Surg Wang X Zhang C Yin JW 4248920172829622510.1111/os.12318 PMC 6584467 · doi ↗ · pubmed ↗
- 2Supination-external rotation ankle fractures: stability a key issue Clin Orthop Relat Res Gougoulias N Khanna A Sakellariou A Maffulli N 24325146820101961824710.1007/s 11999-009-0988-2PMC 2795847 · doi ↗ · pubmed ↗
- 3Optimal management of ankle syndesmosis injuries Open Access J Sports Med Porter DA Jaggers RR Barnes AF Rund AM 173182520142517715310.2147/OAJSM.S 41564 PMC 4128849 · doi ↗ · pubmed ↗
- 4Effectiveness and outcome of early weight bearing in ankle fracture: a systemic review J Pharm Res Int Albaker AB 1323332021
- 5Conservative treatment using platelet-rich plasma for acute anterior cruciate ligament injuries in highly active patients: a retrospective survey Cureus Hada S Hada M Yoshida K Kaneko H Saita Y Kubota M Ishijima M 016202410.7759/cureus.53102 PMC 1089850038414705 · doi ↗ · pubmed ↗
- 6A new way to treat forearm post-traumatic non-union in young patients with intramedullary nailing and platelet-rich plasma Injury Memeo A Verdoni F De Bartolomeo O Albisetti W Pedretti L 4184234520142411949110.1016/j.injury.2013.09.021 · doi ↗ · pubmed ↗
- 7Usefulness of platelet-rich fibrin in open fractures of tibia: a randomised comparative pilot study Apollo Med Sural S Mandal S 2024
- 8Soft-tissue injuries simply need PEACE and LOVE Br J Sports Med Dubois B Esculier J 7273542020 http://orcid.org/0000-0003-0372-4525.3137772210.1136/bjsports-2019-101253 · doi ↗ · pubmed ↗