Association Between Different Thyroid-Stimulating Hormone Levels and Macrovascular Complications in Subclinical Hypothyroidism Patients With Type 2 Diabetes Mellitus
N M Motachim Mahmud, Dhierin R Jagdewsing, Xiaochen Ji, Ibrahim Harine, Bahassane Adjibou, Noor Safra C Fahmy, Thomas Juby, Rafiul I Shuvo, Ausraful Alam, Saudeya Sarmin

TL;DR
This study finds that higher TSH levels in T2DM patients with subclinical hypothyroidism are linked to increased macrovascular complications like PAD and CAD.
Contribution
The study identifies specific TSH thresholds and their association with macrovascular risks in T2DM patients with subclinical hypothyroidism.
Findings
Severe SCH increases macrovascular complications risk 6.08-fold compared to mild SCH.
Moderate SCH increases macrovascular complications risk 4.35-fold compared to mild SCH.
Older age and male sex are significant predictors of macrovascular complications in these patients.
Abstract
Aim: Subclinical hypothyroidism (SCH) is frequently observed in patients with type 2 diabetes mellitus (T2DM) and may exacerbate macrovascular complications due to its impact on metabolic and thyroid function parameters. This study aims to explore the association between varying levels of thyroid-stimulating hormone (TSH) and the risk of macrovascular complications, alongside analyzing key metabolic, demographic, and clinical factors in T2DM patients with SCH. Methods: A retrospective study was conducted at the Second Affiliated Hospital of Dalian Medical University, and data was collected from 2017 to 2023. According to their TSH levels, 305 patients were divided into three groups, which were T2DM mild SCH (TSH 4.34-6.9 mIU/L), T2DM moderate SCH (TSH 7.0-9.9 mIU/L), and T2DM severe SCH (TSH levels of 10.0 mIU/L or higher). The chi-square test was used for categorical variables, while…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
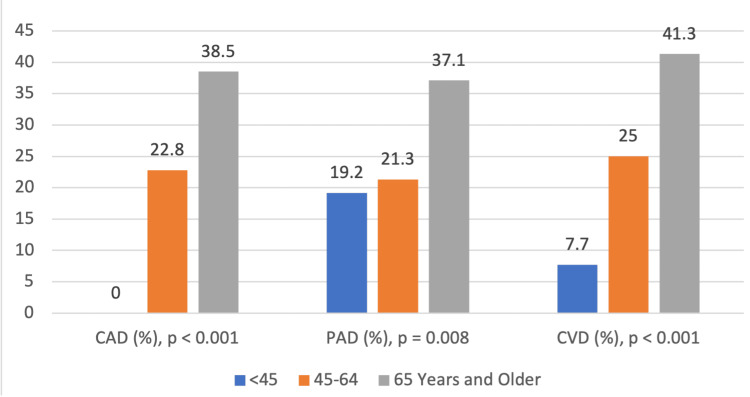 Figure 1
Figure 1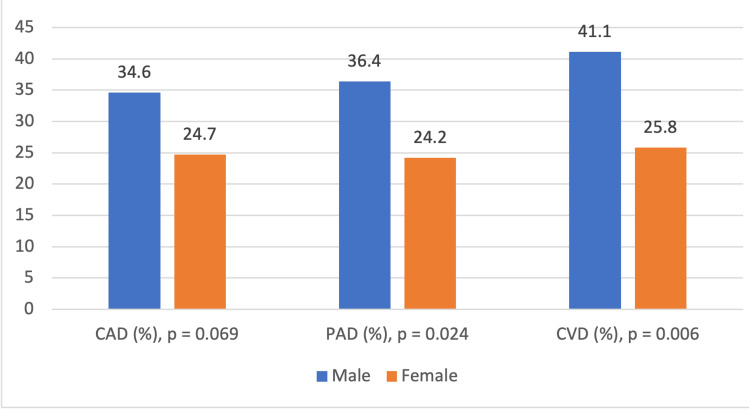 Figure 2
Figure 2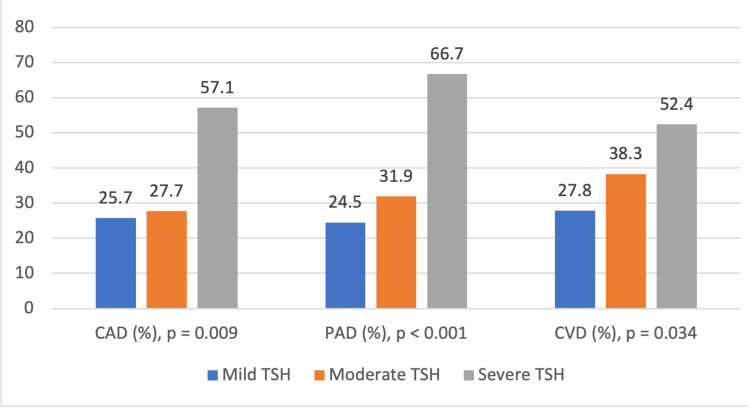 Figure 3
Figure 3| Variable | T2DM Mild SCH (n = 237) | T2DM Moderate SCH (n = 47) | T2DM Severe SCH (n = 21) | p-Value |
| Macrovascular complications, n (%) | 142 (59.9) | 38 (80.9) | 19 (90.5) | <0.001 |
| Age (years), mean ± SD | 62.80 ± 12.61 | 62.02 ± 13.1 | 68.24 ± 11.70 | 0.140 |
| Gender, n (%) | 0.685 | |||
| Female | 151 (63.7) | 33 (70.2) | 14 (66.7) | |
| Male | 86 (36.3) | 14 (29.8) | 7 (33.3) | |
| BMI, mean ± SD | 26.31 ± 3.87 | 25.49 ± 3.76 | 25.82 ± 3.36 | 0.378 |
| T2DM duration (years), mean ± SD | 10.00 ± 7.61 | 8.78 ± 8.24 | 9.48 ± 7.00 | 0.606 |
| BP systolic, mean ± SD | 141.81 ± 18.94 | 142.40 ± 20.15 | 143.38 ± 19.79 | 0.824 |
| BP diastolic, mean ± SD | 79.60 ± 11.09 | 81.04 ± 12.46 | 77.81 ± 10.91 | 0.808 |
| FT3 (pmol/L), mean ± SD | 4.58 ± .57 | 4.61 ± .060 | 4.00 ± .49 | <0.001 |
| FT4 (pmol/L), mean ± SD | 14.86 ± 2.12 | 14.44 ± 1.78 | 13.23 ± 1.52 | 0.002 |
| LDL-C (mmol/L), mean ± SD | 2.82 ± 0.91 | 3.13 ± 1.10 | 3.13 ± 1.79 | 0.089 |
| HDL-C (mmol/L), mean ± SD | 1.20 ± 0.31 | 1.15 ± 0.26 | 1.02 ± 0.16 | 0.025 |
| TC (mmol/L), mean ± SD | 5.10 ± 1.21 | 5.49 ± 1.60 | 5.83 ± 2.34 | 0.023 |
| TG (mmol/L), mean ± SD | 2.14 ± 1.99 | 2.47 ± 3.13 | 1.88 ± 0.97 | 0.518 |
| FBG (mmol/L), mean ± SD | 8.80 ± 3.44 | 8.24 ± 3.26 | 9.58 ± 3.79 | 0.317 |
| HbA1C (%), mean ± SD | 10.25 ± 12.28 | 8.60 ± 2.28 | 8.97 ± 2.27 | 0.586 |
| Hospital stay (days), mean ± SD | 7.19 ± 1.47 | 7.55 ± 1.73 | 7.43 ± 1.54 | 0.283 |
| Variable | T2DM Mild SCH (n = 237) | T2DM Moderate SCH (n = 47) | T2DM Severe SCH (n = 21) | p-Value |
| PAD, n (%) | 58 (24.5) | 15 (31.9) | 14 (66.7) | <0.001 |
| CAD, n (%) | 61 (25.7) | 13 (27.7) | 12 (57.1) | 0.009 |
| CVD, n (%) | 66 (27.8) | 18 (38.3) | 11 (52.4) | 0.034 |
| Univariate | |||
| Variable | OR | 95% CI | p-Value |
| T2DM + moderate SCH vs mild SCH | 2.825 | 1.306-6.111 | 0.008 |
| T2DM + severe SCH vs mild SCH | 6.356 | 1.447-27.920 | 0.014 |
| Age group: 45-64 years vs <45 years | 3.731 | 1.387-10.034 | 0.009 |
| Age group: 65 years and older vs <45 years | 11.138 | 4.032-30.766 | <0.001 |
| Male vs Female | 3.630 | 2.053-6.417 | <0.001 |
| BMI ≥25 vs <25 | 0.847 | 0.522-1.373 | 0.501 |
| FT3 (pmol/L) | 0.754 | 0.501-1.136 | 0.177 |
| FT4 (pmol/L) | 0.961 | 0.858-1.077 | 0.497 |
| LDL-C (mmol/L) | 0.854 | 0.680-1.074 | 0.177 |
| HDL-C (mmol/L) | 0.658 | 0.301-1.438 | 0.294 |
| TC (mmol/L) | 0.910 | 0.769-1.077 | 0.271 |
| TG (mmol/L) | 0.854 | 0.680-1.074 | 0.177 |
| Multivariate | |||
| Variable | OR | 95% CI | p-Value |
| T2DM + moderate SCH vs mild SCH | 4.352 | 1.761-10.754 | 0.001 |
| T2DM + severe SCH vs mild SCH | 6.075 | 1.202-30.715 | 0.029 |
| Age group: 45-64 years vs <45 years | 4.531 | 1.516-13.542 | 0.007 |
| Age group: 65 years and older vs <45 years | 13.492 | 4.326-42.077 | <0.001 |
| Sex: Male | 5.488 | 2.686-11.212 | <0.001 |
| Variable | OR | 95% CI | p-Value |
| PAD | |||
| T2DM + moderate SCH vs mild SCH | 1.542 | 0.766-3.106 | 0.225 |
| T2DM + severe SCH vs mild SCH | 5.913 | 2.202-15.877 | <0.001 |
| Age group: 45-64 years vs <45 years | 1.141 | 0.388-3.353 | 0.811 |
| Age group: 65 years and older vs <45 years | 2.308 | 0.805-6.617 | 0.120 |
| Sex: Male vs Female | 1.913 | 1.116-3.280 | 0.018 |
| CVD | |||
| T2DM + moderate SCH vs mild SCH | 1.751 | 0.881-3.480 | 0.110 |
| T2DM + severe SCH vs mild SCH | 2.463 | 0.960-6.319 | 0.061 |
| Age group: 45-64 years vs <45 years | 4.546 | 1.003-20.601 | 0.050 |
| Age group: 65 years and older vs <45 years | 9.144 | 2.041-40.966 | 0.004 |
| Sex: Male vs Female | 2.252 | 1.330-3.813 | 0.003 |
| CAD | |||
| T2DM + moderate SCH vs mild SCH | 1.155 | 0.557-2.394 | 0.699 |
| T2DM + severe SCH vs mild SCH | 3.268 | 1.279-8.351 | 0.013 |
| Age group: 65 years and older vs 45-64 years | 1.902 | 1.120-3.232 | 0.017 |
| Sex: Male vs Female | 1.753 | 1.022-3.008 | 0.041 |
| Variable | CAD | p-Value | PAD | p-Value | CVD | p-Value |
| Age group | <0.001 | 0.008 | <0.001 | |||
| <45 years | 0 (0.0) | 5 (19.2) | 2 (7.7) | |||
| 45-64 years | 31 (22.8) | 29 (21.3) | 34 (25.0) | |||
| 65 years and older | 55 (38.5) | 53 (37.1) | 59 (41.3) | |||
| Sex | 0.069 | 0.024 | 0.006 | |||
| Male | 37 (34.6) | 39 (36.4) | 44 (41.1) | |||
| Female | 49 (24.7) | 48 (24.2) | 51 (25.8) | |||
| TSH level | 0.009 | <0.001 | 0.034 | |||
| Mild | 61 (25.7) | 58 (24.5) | 66 (27.8) | |||
| Moderate | 13 (27.7) | 15 (31.9) | 18 (38.3) | |||
| Severe | 12 (57.1) | 14 (66.7) | 11 (52.4) |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsThyroid Disorders and Treatments · Growth Hormone and Insulin-like Growth Factors · Pituitary Gland Disorders and Treatments
Introduction
Diabetes mellitus is one of the most common endocrine diseases in the world, with type 2 diabetes mellitus (T2DM) rates increasing and the number of affected people expected to reach 640 million by 2040 [1]. This disorder may be accompanied by other thyroid disorders, such as subclinical hypothyroidism (SCH), which worsens the prognosis of T2DM patients. It is thus important to establish the correlation between thyroid function, particularly thyroid-stimulating hormone (TSH), and macrovascular complications in patients with T2DM. Cardiovascular diseases, cerebrovascular diseases (CVDs), and peripheral vascular diseases (PVDs) are some of the macrovascular complications that continue to be associated with high mortality and morbidity in T2DM patients [2]. A study on diabetic patients showed a two- to four-fold increased probability of cardiovascular diseases and an independent risk factor for CVDs and myocardial infarction (MI) [3]. A large proportion of thyroid disorders in T2DM patients is related to SCH [4,5]. SCH has been reported to be present in 4-17% of the population with diabetes [6]. In typical T2DM patients often TSH levels increase, which may have a strong impact on the cardio-metabolic risk factors, suggesting that SCH is associated with adverse cardiovascular prognosis [7]. The combined impact of T2DM and SCH on lipid profile increases the risk of CVD; T2DM affects lipid metabolism and results in increased levels of low-density lipoprotein cholesterol (LDL-C) and triglycerides (TG) [8]. SCH, with increased TSH levels, continues the further progression of lipid metabolism disturbances, increasing the risk of atherosclerotic processes and cardiovascular events [9].
It is essential to obtain a clear and detailed picture of TSH and the differences and interconnections between T2DM patients with SCH and other comorbidities, which will fill the gaps in the existing knowledge of SCH-T2DM comorbidity and provide crucial information regarding risk factors, clinical significance, and interventions. SCH is a thyroid dysfunction characterized by increased TSH levels with normal free triiodothyronine (FT3) and free thyroxine (FT4) levels, affecting 4-20% of the population [10]. T2DM, which is the most common metabolic disorder, is becoming more prevalent, especially among individuals with inactive lifestyles and poor eating habits [11]. SCH has been known to relate to T2DM, and SCH can be used to predict the occurrence of T2DM [12]. Macrovascular complications of T2DM are CVD, stroke, and PVD, which are associated with atherosclerosis [13]. Peripheral artery disease (PAD) impacts the arteries that supply blood to the extremities, and T2DM patients are at increased risk due to atherosclerosis, endothelial dysfunction, and peripheral neuropathy [14]. Another study provided evidence that SCH in patients with T2DM is associated with a high prevalence of coronary heart disease [15]. On the other hand, previous studies have observed inconsistent results regarding the relationship between TSH levels and cardiovascular events in T2DM patients, suggesting that more research is required to fill knowledge gaps and provide definitive recommendations for managing TSH levels in T2DM patients [16,17]. Therefore, it is important to do this research and better understand the link between raised TSH and macrovascular complications in T2DM patients so that better clinical management strategies can be implemented to enhance the health of these patients.
Materials and methods
This study is based on the patient data from the Second Affiliated Hospital of Dalian Medical University, China, which included T2DM and SCH patients during the years 2017-2023. There were 305 participants included in this study, all of whom were T2DM patients diagnosed with SCH, subdivided by TSH values. Since TSH levels of T2DM with mild SCH patients in the Second Affiliated Hospital of Dalian Medical University started from 4.34 mIU/L, the range of mild TSH was then set to 4.34-6.9 mIU/L. Further, in patients with T2DM and moderate SCH, the TSH levels were set to 7.0-9.9 mIU/L. At last, for the patients with T2DM and severe SCH, the TSH levels were set to 10 mIU/L and higher. This study design allowed for an in-depth investigation of the long-term association between T2DM, SCH, and macrovascular complications.
Patient selection
The inclusion criteria included participants aged between 25 and 90 with confirmed T2DM and laboratory confirmation of thyroid hormone abnormalities, as well as patients with macrovascular complications, including CVD, coronary artery disease (CAD), and PAD. This study excluded patients with type 1 diabetes mellitus, other thyroid diseases (Graves’ disease or thyroid carcinoma), autoimmunity disorders, malignant tumors, infectious diseases, pregnancy, and mental illnesses. Further, patients with alcohol intake, a smoking history in the last 10 years, or a body mass index (BMI) above 40 were also excluded from the study as these factors independently cause macrovascular disease (MVC).
Data collection
TSH levels were the main independent variables divided into mild, moderate, and severe SCH. The main dependent variable was the presence of macrovascular complications. Macrovascular complications in this study included PAD, CVD, and CAD. Conditions such as stroke and transient ischemic attack (TIA), carotid artery disease, cerebral aneurysm including CVD, and symptoms like angina (stable and unstable), MI, heart failure, and sudden cardiac arrest come under CAD, symptoms such as intermittent claudication, critical limb ischemia, acute limb ischemia, and Buerger’s disease are included in the study as PAD. Other parameters included were age, gender, BMI, duration of T2DM, systolic and diastolic blood pressure, lipid profile, thyroid profile (FT3 and FT4), fasting blood glucose, hemoglobin A1C (HbA1C), and hospitalization days.
Data analysis
The data was analyzed using IBM SPSS Statistics for Windows, Version 29.0.2 (Released 2023; IBM Corp., Armonk, NY). Chi-square analyses were used to test the significance of the association between categorical variables, while one-way analysis of variance (ANOVA) was used to compare the mean values of continuous variables. Univariate and multivariate binary logistic regression analysis was used for the risk of macrovascular complications and their subtypes comprising PAD, CAD, and CVD. Further, a statistical significance was set at p <0.05.
Results
Table 1 compares various clinical and biochemical parameters among patients with T2DM categorized by the severity of SCH into mild (n = 237), moderate (n = 47), and severe (n = 21) groups. Notably, the prevalence of macrovascular complications increases with SCH severity, reported at 142 (59.9%) in the mild group, 38 (80.9%) in the moderate group, and 19 (90.5%) in the severe group (p < 0.001). Additionally, significant differences are observed in thyroid hormone levels: mean FT3 levels decrease from 4.58 ± 0.57 pmol/L in mild SCH to 4.00 ± 0.49 pmol/L in severe SCH (p < 0.001) and mean FT4 levels decline from 14.86 ± 2.12 pmol/L to 13.23 ± 1.52 pmol/L across the same groups (p = 0.002). Lipid profiles also show significant variations, with high-density lipoprotein cholesterol (HDL-C) levels decreasing from 1.20 ± 0.31 mmol/L in mild SCH to 1.02 ± 0.16 mmol/L in severe SCH (p = 0.025) and total cholesterol (TC) levels increasing from 5.10 ± 1.21 mmol/L to 5.83 ± 2.34 mmol/L (p = 0.023). Other parameters, including age, gender distribution, BMI, duration of T2DM, blood pressure, LDL-C, TG, fasting blood glucose (FBG), HbA1C, and length of hospital stay, do not exhibit statistically significant differences across SCH severity levels.
In the aspect of macrovascular complications, we observe compelling occurrence rates of PAD, CAD, and CVD across different SCH severity categories. The number of patients with mild SCH was 58 (24.5%), with moderate SCH being 15 (31.9%), and with severe SCH, 14 (66.7%) exhibited PAD. The trend relates to PAD occurrence and SCH severity classes, with a significant p-value of <0.001. The incidence of CAD also widens from 61 (25.7%) in people who suffer from mild SCH to 12 (57.1%) in those with severe SCH, and the people with moderate SCH stand for 13 (27.7%). Nevertheless, the p-value of 0.009 is much like the PAD for the three categories of SCH. It is also statistically significant. In patients with mild SCH, the prevalence of CVD was 66 (27.8%), and it grew to 18 (38.3%) in the moderate SCH and advanced to 11 (52.4%) in the severe SCH. A p-value of 0.034 represents the significance of the difference between the occurrence of cerebral disease and the different SCH severity categories (Table 2).
Table 3 shows the univariate and multivariate logistic regression results with significant predictors. In the univariate analysis, patients with T2DM + severe SCH show significant findings compared to those with mild SCH (OR: 6.356, 95% CI: 1.447-27.920, p= 0.014), and moderate SCH category also shows significant findings (OR: 2.825, 95% CI: 1.306-6.111, p =0.008). Age group 65 and older had the highest odds compared to <45 years (OR = 138, 95% CI: 4.032-30.766, p < 0.001), and the 45-64-year age group also showed elevated odds (OR = 3.731, 95% CI: 1.387-10.034, p = 0.009). On the other hand, male sex shows significant results (OR: 3.630, 95% CI: 2.053-6.417, p < 0.001). Multivariate analysis strongly supports these findings: T2DM with severe SCH shows higher odds (OR: 6.075, 95% CI: 1.202-30.715, p = 0.029), as well as moderate SCH (OR: 4.352, 95% CI: 1.761-10.754, p = 0.001), age 65 and older (OR: 13.492, 95% CI: 4.326-42.077, p < 0.001), and age 45-64 (OR: 4.531, 95% CI: 1.516-13.542, p = 0.007). Male sex also shows more significant findings (OR: 5.488, 95% CI: 2.686-11.212, p < 0.001). It is clear from these results that different TSH levels, age, and sex are the most significant predictors.
The results of the multivariate binary logistic regression analysis for subtypes showed that sex, age, and SCH severity were independent predictors of macrovascular complications in patients with T2DM (Table 4). Male sex consistently emerged as a significant risk factor, with higher odds of developing PAD (OR: 1.913, p = 0.018), CVD (OR: 2.252, p = 0.003), and CAD (OR: 1.753, p = 0.041). Severe SCH was significantly associated with PAD (OR: 5.913, p < 0.001) and CAD (OR: 3.268, p= 0.013) but had only a borderline significance about CVD (OR: 2.463, p = 0.061); moderate SCH did not reveal significant effect. Age also played an important role, as the 65 and older age group exhibited markedly increased risks for CVD (OR: 9.144, p = 0.004) and CAD (OR: 1.902, p = 0.017) compared to younger groups, though it had no significant effect on PAD. These observations point to the fact that macrovascular complications are more common in male patients, elderly patients, and those with severe SCH in T2DM.
Table 5 shows that CAD, PAD, and CVD are distributed substantially differently among age groups, sexes, and TSH levels and are associated with these risk factors. Age shows significant correlation with macrovascular complication subtypes, p < 0.001 for CAD and CVD and p = 0.008 for PAD, respectively. The age group 65 years and older shows the highest prevalence, 55 (38.5%) for CAD, 53 (37.1%) for PAD, and 59 (41.3%) for CVD; the lowest prevalence was found in the <45 years age group. Sex differences also show notable findings, especially for PAD (p = 0.024) and CVD (p = 0.006), where male patients demonstrated higher prevalences, 39 (36.4%) and 44 (41.1%), respectively, compared to female patients, 48 (24.2%) and 51 (25.8%), respectively. Although the incidence of CAD was more common among male patients, 37 (34.6%), than female patients, 49 (24.7%), the difference was not significant (p = 0.069). All three complications were significantly associated with TSH levels, with the most prevalent in the severe SCH group with CAD (12 (57.1%), p = 0.009), PAD (14 (66.7%), p < 0.001), and CVD (11 (52.4%), p = 0.034), and the least in the mild SCH patients. Therefore, these findings suggest that advanced age, male sex, and higher TSH are independent risk factors for macrovascular complications in T2DM patients requiring a targeted intervention in high-risk populations.
Figure 1 presents the prevalence of PAD, CAD, and CVD among T2DM patients with varying degrees of SCH (mild, moderate, and severe). The prevalence of PAD significantly increases with SCH severity, rising from 24.5% in mild SCH to 31.9% in moderate SCH and 66.7% in severe SCH (p < 0.001). A similar trend is observed for CAD (25.7%, 27.7%, and 57.1%, respectively; p = 0.009) and CVD (27.8%, 38.3%, and 52.4%, respectively; p = 0.034). The statistically significant p-values indicate a strong association between increasing SCH severity and higher prevalence of PAD, CAD, and CVD in T2DM patients.
Prevalence of CAD, PAD, and CVD across different age groups in T2DM patients with SCHCAD: coronary artery disease; PAD: peripheral artery disease; CVD: cerebrovascular disease.
Figure 2 compares the prevalence of CAD, PAD, and CVD between male and female patients. For CAD, male patients show a higher prevalence of 34.6% compared to 24.7% in female patients, though this difference is not statistically significant (p = 0.069). However, significant differences are observed for PAD and CVD, with male patients having a prevalence of 36.4% and 41.1%, respectively, compared to 24.2% and 25.8% in female patients (p = 0.024 for PAD and p = 0.006 for CVD). These findings highlight that male patients have a consistently higher prevalence of PAD and CVD compared to female patients, with statistically significant differences.
Prevalence of CAD, PAD, and CVD among male and female T2DM patients with SCHCAD: coronary artery disease; PAD: peripheral artery disease; CVD: cerebrovascular disease.
Figure 3 shows the prevalence of CAD, PAD, and CVD across patients with varying levels of TSH categorized as mild, moderate, and severe. The prevalence of CAD increases from 25.7% in mild TSH to 27.7% in moderate TSH and 57.1% in severe TSH (p = 0.009). Similarly, the prevalence of PAD rises significantly from 24.5% in mild TSH to 31.9% in moderate TSH and 66.7% in severe TSH (p < 0.001). For CVD, the prevalence also increases from 27.8% in mild TSH to 38.3% in moderate TSH and 52.4% in severe TSH (p = 0.034). These findings highlight a strong association between increasing TSH levels and the prevalence of CAD, PAD, and CVD.
Prevalence of CAD, PAD, and CVD by different TSH levels in T2DM patients with SCHCAD: coronary artery disease; PAD: peripheral artery disease; CVD: cerebrovascular disease; TSH: thyroid-stimulating hormone; T2DM: Type 2 diabetes mellitus.
Discussion
T2DM and the various stages of SCH were found to have a very close relationship regarding the macrovascular complications of the patients. In our study, we found that the severe SCH cohort had the highest macrovascular event of 19 (90.5%), approximately 6.4 times higher odds of developing macrovascular complications compared to those with mild SCH. The results obtained from the univariate and multivariate logistic regression analysis support the importance of TSH levels, age, and sex in determining the outcomes investigated. Elevated TSH levels, particularly in the severe SCH category, were strongly associated with increased odds of the outcome in both univariate (OR: 6.356, 95% CI: 1.447-27.920, p = 0.014) and multivariate analyses (OR: 6.075, 95% CI: 1.202-30.715, p = 0.029). A study that outlined macrovascular complications of diabetes demonstrated that the prevalence of PAD was significantly higher in patients with SCH compared to euthyroid T2DM patients [12]. Others found that SCH has been associated with increased cardiovascular mortality due to adverse effects mainly on lipids and blood pressure and also evidence that SCH, especially in patients with TSH >10 mU/L, may increase cardiovascular risk [18].
Regression analysis was not statistically significant for FT3, FT4, HDL-C, LDL-C, TC, and TG in our study, which could be due to the small sample size of these variables or their lesser correlation with the outcomes under the study. Although these results do not negate the clinical relevance of these factors, they indicate that their expression may be more conditional or influenced by other factors. Further, another important predictor was age; the patients aged 65 years and older had significantly higher risks of developing CVD or CAD than those of a younger age. These findings indicate that age is an important modifier most likely because of cumulative vascular injury and other diseases in the elderly population. Age was not associated with the development of PAD, which may indicate that the processes that lead to this complication are different. Taken together, these data highlight the need to take into account sex, age, and SCH severity when evaluating and treating T2DM patients at risk of macrovascular complications.
The findings of the multivariate binary logistic regression analysis of subgroups reveal significant risk factors that led to macrovascular complications in T2DM patients. SCH was found to be independently associated with PAD and CAD. The result of the study is also in line with the research work, which states that the pathological condition of PAD has significantly increased in patients with SCH against the euthyroid individuals [19]. Such discovery is in line with our study, which showed that individuals with SCH had high chances of CAD, particularly those with higher TSH levels. Furthermore, in the SCH-CAD risk study conducted, there was an association between heart disease and SCH. This study also follows the same trend that there is a stronger tendency to develop strokes and heart diseases in patients with SCH, mainly as exhaustion of TSH rises [20]. The majority of patients diagnosed with T2DM and SCH experienced MVC, specifically TIA/stroke (23.3%), angina pectoris (16.7%), PAD (10.0%), and abnormal lipid profile [17]. These findings provide significant evidence for our study. Another research also noticed that SCH is a risk factor for ischemic stroke and affects recovery [21].
This study also found age as a significant factor; groups 45-64 years and 65 and older had significantly higher odds ratios than those below 45 years. The strongest association was observed in the 65 years and older age group (multivariate OR: 13.492, 95% CI: 4.326-42.077, p < 0.001), indicating the need for appropriate intervention in the elderly. This is in line with the previous research showing that older adults are at a higher risk of experiencing adverse health outcomes because of comorbidities, decreased physiological reserve capacity, and slow healing rates. A meta-analysis published in 2020 concluded that SCH in older age is a high-risk risk factor for the onset of macrovascular complications and mortality [22].
Sex was another significant predictor, with male patients demonstrating higher odds compared to female patients (multivariate OR: 5.488, 95% CI: 2.686-11.212, p < 0.001). This is in line with a study that suggests that male patients are at a higher risk of macrovascular complications with T2DM [23]. In general, the results of this study contribute to the understanding that factors like age, male sex, and severe TSH levels can increase the risk of macrovascular complications in T2DM patients with SCH.
Limitations and recommendations
This study provides valuable insights into the association between TSH levels and macrovascular complications in T2DM patients with SCH. However, certain limitations must be acknowledged. First, the retrospective single-center design may restrict the generalizability of the findings, as variations in healthcare settings, genetic predispositions, and environmental factors were not accounted for. Additionally, the sample size, particularly the severe SCH group (n = 21), was relatively small, which may affect the statistical power of the analysis. Another limitation is the cross-sectional nature of the study, which prevents conclusions about causality or the progression of macrovascular complications over time. Furthermore, some important confounders, such as inflammatory markers, thyroid hormone replacement therapy (THRT), and lifestyle factors, were not included in the analysis, which may influence the observed associations.
To address these limitations, future research should include prospective cohort studies to track TSH fluctuations over time and assess their long-term impact on macrovascular complications. Additionally, multicenter studies with larger, diverse populations can improve the validity of these findings. Investigating the potential benefits of THRT on cardiovascular outcomes in T2DM patients with SCH through randomized controlled trials is also recommended. Further studies should explore inflammatory and metabolic pathways, including oxidative stress markers, to better understand the mechanisms linking SCH, T2DM, and MVC. By addressing these gaps, future research can provide more robust clinical guidelines for the management of SCH in T2DM patients at risk for cardiovascular complications.
Conclusions
Patients with T2DM and moderate or severe SCH are at a significantly higher risk of macrovascular complications, particularly PAD and CAD, compared to those with mild SCH. Elevated TSH levels strongly contribute to these risks, with older age and male sex further increasing the likelihood of adverse outcomes. These findings emphasize the importance of close monitoring and timely intervention for T2DM patients with elevated TSH levels. Tailored risk management strategies focusing on these high-risk groups can play a vital role in improving long-term vascular health and overall outcomes.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1A wake-up call for type 2 diabetes?N Engl J Med Persaud SJ Jones PM 1090109237520162762652410.1056/NEJ Mcibr 1607950 · doi ↗ · pubmed ↗
- 2Macrovascular complications of type 2 diabetes mellitus Curr Vasc Pharmacol Viigimaa M Sachinidis A Toumpourleka M Koutsampasopoulos K Alliksoo S Titma T 1101161820203096149810.2174/1570161117666190405165151 · doi ↗ · pubmed ↗
- 3Type 2 diabetes mellitus and cardiovascular disease: Genetic and epigenetic links Front Endocrinol (Lausanne) De Rosa S Arcidiacono B Chiefari E Brunetti A Indolfi C Foti DP 2920182938704210.3389/fendo.2018.00002 PMC 5776102 · doi ↗ · pubmed ↗
- 4Prevalence of undiagnosed hypothyroidism in Europe: A systematic review and meta-analysis Eur Thyroid J Mendes D Alves C Silverio N Batel Marques F 130143820193125915510.1159/000499751 PMC 6587201 · doi ↗ · pubmed ↗
- 5Thyroid status in patients with type 2 diabetes attending a tertiary care hospital in Eastern India Indian J Endocrinol Metab Pramanik S Ghosh S Mukhopadhyay P 1121152220182953594810.4103/ijem.IJEM_572_17PMC 5838889 · doi ↗ · pubmed ↗
- 6Prevalence and progression of subclinical hypothyroidism in women with type 2 diabetes: The Fremantle Diabetes Study Clin Endocrinol (Oxf) Chubb SA Davis WA Inman Z Davis TM 4804866220051580788010.1111/j.1365-2265.2005.02246.x · doi ↗ · pubmed ↗
- 7Subclinical hypothyroidism ups the risk of vascular complications in type 2 diabetes Alexandria J Med Mohamed GA Elsayed AM 285288532017
- 8Dyslipidemia in type 2 diabetes mellitus Nat Clin Pract Endocrinol Metab Mooradian AD 150159520091922923510.1038/ncpendmet 1066 · doi ↗ · pubmed ↗