Screw stent removal technique using a novel grasping device after inside plastic stent deployment for hilar biliary obstruction
Takeshi Ogura, Yuki Uba, Takafumi Kanadani, Kimi Bessho, Hiroki Nishikawa

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Fig. 1
Fig. 1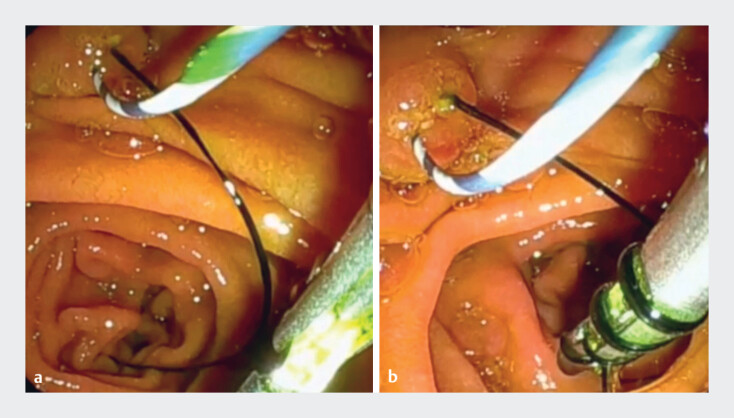 Fig. 2
Fig. 2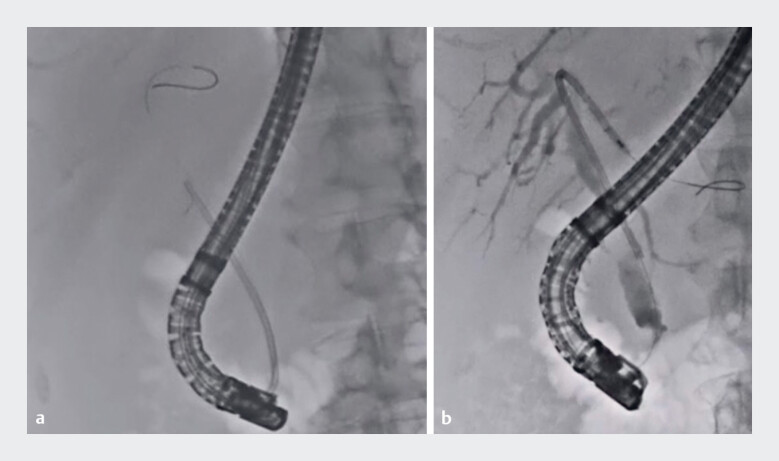 Fig. 3
Fig. 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGallbladder and Bile Duct Disorders · Pediatric Hepatobiliary Diseases and Treatments · Biliary and Gastrointestinal Fistulas
In cases of unresectable malignant hilar biliary obstruction, uncovered self-expandable metal stent (UCSEMS) deployment using a side-by-side or stent-in-stent technique may be recommended for the purpose of prolonging stent patency, according to a consensus statement and guideline 1 2 . However, because of recent improvements in systemic chemotherapy, such as immune checkpoint inhibitors 3 , the number of reinterventions required may have increased. If a UCSEMS is deployed, reintervention may be challenging, because the UCSEMS cannot be removed.
The technique of inside plastic stent deployment has also been developed with the aim of obtaining longer stent patency. According to a recent meta-analysis 4 , inside plastic stent deployment and UCSEMS deployment have been reported to have similar efficacy. To remove an inside plastic stent, the thread must be grasped, but it may break during stent removal. Yokode et al. described a technique using rotatable grasping forceps to safely remove such stents 5 ; however, the device they used has a coiled sheath, so the removal force may be weak. Recently, a novel rotatable grasping forceps has become available (ENDO Glip; AGS Med Tech, Tokyo, Japan) ( Fig. 1 ). Unlike with conventional rotatable grasping forceps, the removal force with the novel forceps can be transmitted directly because of its noncoiled sheath. In this report, a screw stent removal technique using the novel grasping device is described ( Video 1 ).
Photograph of a novel rotatable grasping forceps (ENDO Glip; AGS Med Tech, Tokyo, Japan).
A novel rotatable grasping forceps is used to remove an inside plastic stent, with the thread twisting around the forceps as the forceps is rotated, leading to successful removal of the stent without breakage of the thread.Video 1
A 71-year-old man was admitted to our hospital with recurrent biliary obstruction. He had undergone inside plastic stent deployment for cholangiocarcinoma 6 months previously. Therefore, reintervention under endoscopic retrograde cholangiopancreatography (ERCP) guidance was attempted. The duodenoscope was first inserted into the second part of the duodenum, where the thread of the inside plastic stent was identified ( Fig. 2 a ). After a 0.025-inch guidewire had been placed into the biliary tract, the thread was grasped using the novel rotatable grasping forceps. The grasping forceps was then rotated, with the thread twisting around the forceps ( Fig. 2 b ). This allowed the inside plastic stent to be successfully removed, without the thread breaking ( Fig. 3 a ). Finally, a new inside plastic stent was deployed ( Fig. 3 b ).
Endoscopic views showing: a visualization of the thread of the inside plastic stent; b the thread being grasped with the novel rotatable grasping forceps, which is then rotated, with the thread gradually twisting around the forceps.
Fluoroscopic images showing: a the inside plastic stent being successfully removed without the thread breaking; b an inside plastic stent being deployed.
In conclusion, a technique using the novel rotatable grasping forceps might be useful for the removal of inside plastic stents.
Endoscopy_UCTN_Code_TTT_1AR_2AZ
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Angsuwatcharakon P Kulpatcharapong S Chuncharunee A The updated Asia-Pacific consensus statement on the role of endoscopic management in malignant hilar biliary obstruction Endosc Int Open 202412 E 1065 E 107410.1055/a-2366-730239285860 PMC 11405119 · doi ↗ · pubmed ↗
- 2van der Merwe S Wvan Wanrooij RLJ Bronswijk M Therapeutic endoscopic ultrasound: European Society of Gastrointestinal Endoscopy (ESGE) Guideline Endoscopy 20225418520510.1055/a-1717-139134937098 · doi ↗ · pubmed ↗
- 3Kelley RK Ueno M Yoo C Pembrolizumab in combination with gemcitabine and cisplatin compared with gemcitabine and cisplatin alone for patients with advanced biliary tract cancer (KEYNOTE-966): a randomised, double-blind, placebo-controlled, phase 3 trial Lancet 20234011853186537075781 10.1016/S 0140-6736(23)00727-4 · doi ↗ · pubmed ↗
- 4Alsakarneh S Madi MY Jaber F Safety and efficacy of biliary suprapapillary metal and plastic stents in malignant biliary obstruction: a systematic review and meta-analysis Surg Endosc 2024384186419710.1007/s 00464-024-11025-038987483 · doi ↗ · pubmed ↗
- 5Yokode M Matsumori T Uza NA unique technique for the removal of threaded biliary inside plastic stents Endoscopy 202254 E 496E 49710.1055/a-1640-882934624922 · doi ↗ · pubmed ↗