Colonic stenting plus vascular plug for malignant gastrocolonic fistula
Kewei Ren, Yahua Li, Zongming Li, Zeyi Yao, Bo Ma, Jianzhuang Ren, Xinwei Han

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
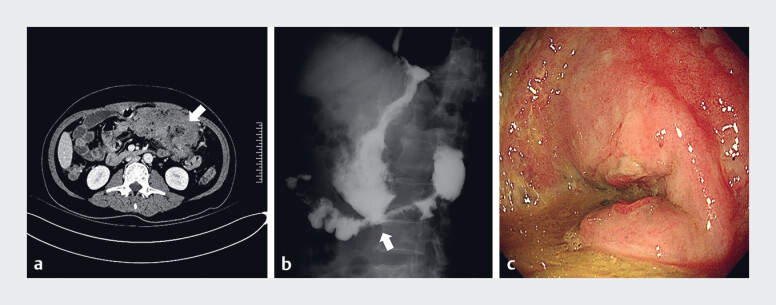 Fig. 1
Fig. 1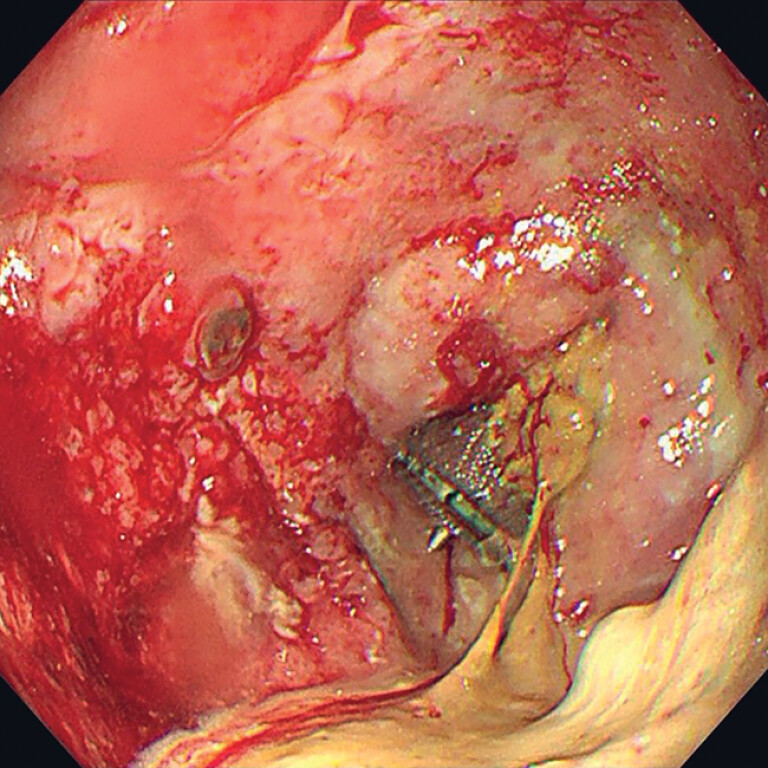 Fig. 2
Fig. 2 Fig. 3
Fig. 3- —Henan Medical Science and Technology Research Program
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsBiliary and Gastrointestinal Fistulas · Esophageal and GI Pathology · Gastrointestinal disorders and treatments
A 48-year-old man visited our department with a 3-month history of intermediate abdominal pain. In the past 2 months, he had received two cycles of chemotherapy for gastric T-cell lymphoma with colon invasion. Seven days ago, he suffered diarrhea with food debris after a liquid diet. Abdominal computed tomography (CT), gastrointestinal radiography, and gastroscopy revealed the formation of a gastrocolonic fistula and transverse colonic stenosis ( Fig. 1 ). Colonic stenting plus vascular plug placement was developed to solve this problem ( Video 1 ).
Initial imaging. a, b Abdominal computed tomography ( a ) and gastrointestinal radiography ( b ) revealed formation of a gastrocolonic fistula and transverse colonic stenosis (arrow). c The tumor and fistula (arrow) at gastroscopy.
Colonic stenting plus vascular plug for malignant gastrocolonic fistula.Video 1
For this procedure, a 5-Fr curved catheter and guidewire were first introduced to the location of the fistula through the anus. Radiography suggested stenosis of the transverse colon and gastrocolonic fistula formation. A 24 × 120 mm intestinal uncovered stent was successfully placed under fluoroscopic guidance. Then, another 5-Fr vertebral artery catheter and guidewire were introduced through the mouth to the colonic lumen via the gastrocolonic fistula and stent mesh. A 6 × 80 mm balloon was introduced to dilate the stent mesh and insert a 7-Fr sheath. A 16 × 12 mm vascular plug (9-AVP2-016; Abbott, Chicago, Illinois, USA) was introduced. The distal part was released to oppose the stent wall, and the body and proximal part were released in the fistula channel and gastric cavity. Finally, radiography demonstrated that the contrast agent did not enter the colon. Gastroscopy observed the full expansion of the vascular plug in the fistula channel ( Fig. 2 ). CT confirmed the placement of the stent plus vascular plug ( Fig. 3 ). Over the following 2 months, the symptom of diarrhea after eating disappeared. Gastrointestinal radiography did not observe the contrast agent entering the colon.
At gastroscopy, full expansion of the vascular plug in the fistula channel was observed.
Computed tomography confirmed the placement of the stent plus vascular plug.
The management of gastrocolonic fistula includes surgical repair, opposing stent 1 , and cardiac septal defect closure device 2 . This is the first report of colonic stenting plus vascular plug placement for malignant gastrocolonic fistula, which proved an effective and safe method. Furthermore, the stent acted as an anchor to avoid migration of the vascular plug.
Endoscopy_UCTN_Code_TTT_1AO_2AI
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Gupta S Chis R Mosko JD Dual-sided closure of an iatrogenic gastrocolonic fistula with over-the-scope clips Endoscopy 202456 E 609W 61010.1055/a-2351-290939009019 PMC 11250258 · doi ↗ · pubmed ↗
- 2Melmed GY Kar S Geft IA new method for endoscopic closure of gastrocolonic fistula: novel application of a cardiac septal defect closure device (with video)Gastrointest Endosc 20097054254519699982 10.1016/j.gie.2009.03.027 · doi ↗ · pubmed ↗