Papillary thyroid carcinoma within struma ovarii: a case report and literature review
Aras J Qaradakhy, Rawa M Ali, Rebaz M Ali, Hadeel A Yasseen, Shvan M Hussein, Hiwa O Abdullah, Shko H Hassan, Harun Amanj Ahmed, Abdulwahid M Salih, Snur Othman, Fahmi H Kakamad

TL;DR
A rare case of papillary thyroid carcinoma in a woman's ovary, without thyroid issues, highlights the need for early detection in perimenopausal women.
Contribution
This case report adds to the limited literature on papillary thyroid carcinoma within struma ovarii and emphasizes diagnostic considerations.
Findings
A 50-year-old woman was diagnosed with papillary thyroid carcinoma in struma ovarii, with no thyroid abnormalities.
A review of 10 cases showed a median age of 46.5 years and symptoms like abdominal pain and vaginal bleeding.
Routine checkups and thyroid evaluation are important for early detection in similar cases.
Abstract
Struma ovarii (SO) is a rare ovarian teratoma mostly made of thyroid tissue, with papillary thyroid carcinoma (PTC) being even rarer. This report presents a 50-year-old woman with PTC in SO and a normal thyroid. A left ovarian cyst was detected by ultrasound and confirmed by MRI. Surgery included total abdominal hysterectomy with bilateral salpingo-oophorectomy, revealing focal PTC and no thyroid abnormalities. A review of 10 cases showed a median diagnosis age of 46.5 years, with symptoms like abdominal pain and vaginal bleeding. Routine checkups in perimenopausal women are key for early detection, and thyroid evaluation is important in PTC cases within SO.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
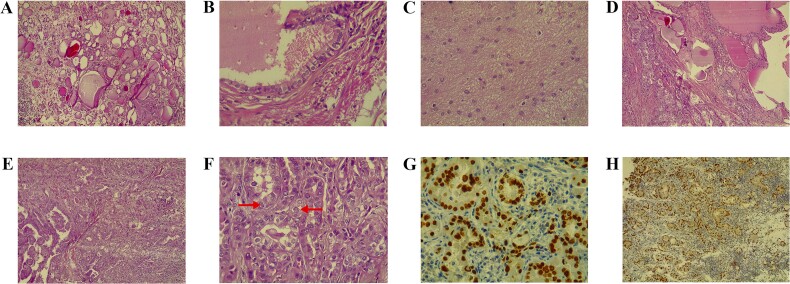 Figure 1
Figure 1|
|
|
|
|
|
|
|
|
|
|---|---|---|---|---|---|---|---|---|
| Chiu | Taiwan | 47 | F | Vaginal spotting | U/S: big cystic mass with central sand-like | TAH + BSO | PTC (12.5 × 8.0 × 4.0 cm) | No recurrence or metastasis |
| Al Hassan | Qatar | 42 | F | Lower abdominal pain | U/S: large solid cystic mass in the right adnexa region, reaching the midline (≈6 × 13 cm) with mild vascularity in the solid component. | TAH + BSO + infracolic omentectomy | PTC | No malignancy in the right fallopian tube, uterus, or cervix, and negative lymph nodes. |
| Winata | Indonesia | 50 | F | Abdominal pain | U/S: probe-sized hypo-hyperechoic image with a solid part and septa. | TAH + BSO, chemotherapy | PTC (20 × 20 cm) | Complete response and no mass residual |
| Hmidi | Tunisia | 37 | F | Incidental finding during cesarean section | NA | Cystectomy | PTC (20 × 20 × 10 mm) | No recurrence 7 years after surgery |
| Leuștean | Romania | 46 | F | Incidental finding during routine U/S examination | U/S: large right ovary (57 × 38 mm) with a relatively well-defined cystic image in the periphery (44 × 43 mm). Its size increased after six months. | TAH + left laparoscopic adnexectomy | Follicular variant of PTC. (90 mm) | No recurrence after 1-year follow-up. |
| Kabootari | Iran | 47 | F | Abnormal uterine bleeding | U/S: bilateral adnexal masses (51 × 31 mm in the right ovary and 38 × 29 mm in the left ovary). | TAH + BSO | Mixed papillary and follicular variant of PTC | No recurrence or distant metastasis after six years. |
| Rahimi | Iran | 64 | F | Abdominal pain | U/S: a large, heterogeneous mass with an irregular border (43 × 45 mm) in the left ovary. | TAH + BSO | PTC | No distant metastasis |
| Ioannidis | Greece | 65 | F | Abdominal pain | U/S: A mass (37 × 27 × 37 mm) was detected in the ovary. | TAH + BSO | Mature cystic teratoma of the right ovary, in which PTC was noted. | No signs of recurrence or any other complications after four months. |
| Alamdari | Iran | 10 | F | Palpitation | U/S: a solid mass (113 × 112 × 100 mm) with volume of 670 cc in the right ovary with no ascites. | Unilateral oophorectomy | PTC | Symptom-free following eight months after surgery and iodine therapy |
| Kim | South Korea | 22 | F | Abdominal pain | CT and U/S revealed bilateral ovarian cysts (each approximately 10 cm in size) and left ovarian torsion. | Laparoscopic bilateral ovarian cystectomy | PTC | Stable health condition during 10 months after surgery |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsOvarian cancer diagnosis and treatment · Thyroid Cancer Diagnosis and Treatment · Thyroid and Parathyroid Surgery
Introduction
Struma ovarii (SO) is a rare ovarian teratoma subtype, primarily composed of thyroid tissue (>50%), earning it the term “ovarian goiter” [1]. It can exhibit various thyroid pathologies, both benign and malignant. Malignant features are rare, occurring in <10% of cases, and may include papillary thyroid carcinoma (PTC), its follicular variant, or mixed variants, which share molecular and prognostic similarities with thyroid-origin tumors [2–4]. The cause of PTC within SO is unclear, typically affecting women aged 40–60. It is vital to differentiate primary ovarian PTC from thyroid metastasis due to differing prognoses and treatments [5, 6]. This report presents a case of primary PTC within SO in a patient with a normal thyroid, following CaReL guidelines and peer-reviewed references [7, 8].
Case presentation
A 50-year-old unmarried woman presented for a routine checkup due to amenorrhea. Ultrasound (U/S) incidentally detected a left ovarian cyst. She had no significant medical, surgical, or family history and was vitally stable with normal physical and lab findings. Pelvic U/S showed a left ovarian cyst (84 × 52 × 55 mm), an anteverted uterus with 8 mm endometrial thickness, no free fluid, and an empty uterine cavity. MRI identified three fibroids (largest 65 × 63 × 57 mm) and a left ovarian cystic-solid lesion (74 × 65 × 48 mm) suggestive of a cystic adenofibroma. No pathological pelvic lymph nodes were observed.
Under general anesthesia, a total abdominal hysterectomy with bilateral salpingo-oophorectomy was performed. Histopathology revealed a 7.5 × 7 × 6 cm mass resembling thyroid tissue. Microscopy showed a cyst lined by ciliated epithelium and various mature elements, including thyroid follicles, glial tissue, and lymphoid follicles. A small invasive glandular area exhibited papillary structures with nuclear features of PTC. Stromal changes included hyalinization, histiocyte aggregation, calcification, and luteinization. Immunostaining showed >90% positivity for PAX8 and TTF1, 50% for CK7, and < 5% for Napsin-A. These findings confirmed PTC arising within SO (Fig. 1).
A) The teratoma predominantly comprises benign thyroid tissue (hematoxylin and eosin stain, magnification 100×). B) Higher magnification shows a focal duct-like structure lined by ciliated epithelium (hematoxylin and eosin stain, magnification 400×). C) Another focus demonstrates mature glial tissue (hematoxylin and eosin stain, magnification 40×). D) The section depicts normal thyroid tissue on the right transitioning into papillary thyroid carcinoma on the left (hematoxylin and eosin stain, magnification 100×). E) A small focus of papillary projections with numerous crowded follicular structures, indicative of papillary thyroid carcinoma (hematoxylin and eosin stain, magnification 100×). F) High-power view shows crowded follicular structures with enlarged, optically clear nuclei that show occasional pseudoinclusions (arrows), features characteristic of papillary thyroid carcinoma (hematoxylin and eosin stain, magnification 400×). G) Immunohistochemical stain for TTF1 demonstrating strong, diffuse, nuclear staining in the crowded follicles (diaminobenzidine chromogen, magnification 400×). H) Immunohistochemical stain for PAX-8 showing a strong, diffuse, nuclear staining pattern in the crowded glands (diaminobenzidine chromogen, magnification 100×)
Postoperative recovery was uneventful. Further evaluation showed euthyroid status and normal thyroid U/S findings.
Discussion
Teratoma, the most common ovarian germ cell tumor, is usually benign, with malignant transformation (<2%) often as squamous cell carcinoma (80%) and rarely as thyroid carcinomas (0.1%–0.2%) [6, 9]. SO, where thyroid tissue forms >50% of a teratoma, accounts for 2%–5% of teratomas and 0.5%–1% of ovarian tumors. Malignancy in SO (<10%) is mainly PTC (53%), followed by its follicular variant (41%) and follicular thyroid carcinoma (FTC) (6%) [2, 6, 10]. PTC pathogenesis in SO is unclear, with theories involving germ cells, ectopic thyroid, somatic transformation, hormones, and immunity [6].
Risk factors for PTC include radiation, diabetes, female gender (three times higher risk), obesity, smoking, alcohol, genetic factors, and excessive dietary nitrates and iodine. Thyroid carcinomas often coexist with breast, colon, stomach cancers, and non-Hodgkin lymphoma [11, 12], but thyroid carcinoma linked to ovarian disease is rare [2, 3]. SO, symptoms range from asymptomatic to abdominal pain, palpable masses, ascites, abnormal vaginal bleeding, hyperthyroidism, and Meigs syndrome [4]. Kabootari et al. reported a 47-year-old woman with abnormal uterine bleeding, diagnosed with PTC in SO [13]. Al Hassan et al. described a 42-year-old with intermittent abdominal pain and regular cycles [3].
In 10 reviewed cases [1, 3, 5, 6, 10, 13–17], the median age at diagnosis was 46.5 years, with abdominal pain and vaginal bleeding as common symptoms (Table 1). This report describes a 50-year-old woman with menstrual cessation and menopausal signs after a routine checkup, with no notable medical history.
SO, on U/S may appear as a heterogeneous, unilocular or multilocular solid mass, or multilocular cystic masses, with “struma pearls” as key features, vascularized on Doppler [3]. MRI can resemble ovarian carcinomas, showing mixed cystic and solid components or adnexal masses with ascites, but lacks specificity for malignant transformation except in cases of rapid tumor growth with irregular borders [10]. U/S was the primary diagnostic tool in the reviewed cases, supplemented by CT and MRI. In this case, U/S and MRI showed a multiloculated cyst with no vascularity, pelvic fluid, or abnormal lymph nodes.
The optimal treatment for malignant SO is debated. Surgical options include bilateral salpingo-oophorectomy with omentectomy and lymph node sampling, often with total abdominal hysterectomy, especially for postmenopausal women [15, 16]. For younger patients, unilateral oophorectomy may be considered [4, 17]. Post-operative histopathology confirms SO by identifying thyroid follicles with patterns like micro- and macro-follicles [3]. In malignant SO, distinguishing primary ovarian tumors from secondary thyroid tumors is essential [5]. Thyroidectomy is recommended for monitoring, though a stable case was reported without thyroidectomy for seven years [6]. PTC in SO shares mutations like BRAF, RET, and RAS with primary thyroid cancers [6]. This case showed mostly benign thyroid tissue with a small area of papillary carcinoma.
When SO is found incidentally, thyroid function tests and neck U/S are key to check for coexisting pathology. PTC within SO generally has a good prognosis [1, 5, 6, 13]. In this case, thyroid function was normal, and neck U/S showed no issues, so the patient was placed on follow-up. A limitation of this report is the lack of radiologic images. Routine checkups, especially in perimenopausal women, are important for detecting silent conditions like SO, and thyroid assessment may be needed in PTC cases to rule out metastasis.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Chiu MT, Yang CY, Yeh NC, et al. Papillary thyroid carcinoma in malignant struma ovarii with negative findings in thyroid gland: a case report and literature review. Formosan Journal of Endocrinology and Metabolism 2020;11:67–72.
- 2Stanojevic B, Dzodic R, Saenko V, et al. Unilateral follicular variant of papillary thyroid carcinoma with unique KRAS mutation in struma ovarii in bilateral ovarian teratoma: a rare case report. BMC Cancer 2012;12:1–5. 10.1186/1471-2407-12-224.22682753 PMC 3407026 · doi ↗ · pubmed ↗
- 3al Hassan MS, Saafan T, el Ansari W, et al. The largest reported papillary thyroid carcinoma arising in struma ovarii and metastasis to opposite ovary: case report and review of literature. Thyroid Res 2018;11:1–9. 10.1186/s 13044-018-0054-9.30061934 PMC 6056926 · doi ↗ · pubmed ↗
- 4Selvaggi F, Risio D, Waku M, et al. Struma ovarii with follicular thyroid-type carcinoma and neuroendocrine component: case report. World J Surg Oncol 2012;10:1–5. 10.1186/1477-7819-10-93.22613573 PMC 3586957 · doi ↗ · pubmed ↗
- 5Winata IG, Suardika A, Marta KF, et al. Papillary thyroid carcinoma within mature teratoma ovarian: A rare case report. Asian Journal of Engineering, Social and Health 2023;2:580–6. 10.46799/ajesh.v 2i 7.114. · doi ↗
- 6Hmidi A, Sahraoui G, Charfi L, et al. Unexpected finding: papillary thyroid carcinoma arising in a mature ovarian teratoma-A case report and literature review. Int J Surg Case Rep 2023;112:108944. 10.1016/j.ijscr.2023.108944.37852093 PMC 10667761 · doi ↗ · pubmed ↗
- 7Prasad S, Nassar M, Azzam AY, et al. Ca Re L guidelines: A consensus-based guideline on case reports and literature review (Ca Re L). Barw Med J 2024;2:13–9. 10.58742/bmj.v 2i 2.89. · doi ↗
- 8Hiwa O. Abdullah, Berun A. Abdalla, Fahmi H. Kakamad, et al. Predatory publishing lists: A review on the ongoing battle against fraudulent actions. Barw Med J 2024;2:26–30. 10.58742/bmj.v 2i 2.91. · doi ↗