Use of Olaparib in the Management of Metastatic Parathyroid Carcinoma With BRCA1 Mutation
David Woodfield, Trang Le, Grace Prince, Hyun Lee, Hetal Vachhani, Priyanka Majety

TL;DR
A patient with metastatic parathyroid carcinoma and a BRCA1 mutation showed a temporary improvement with olaparib treatment.
Contribution
This is the first reported case of olaparib use in metastatic parathyroid carcinoma with a BRCA1 variant of unknown significance.
Findings
Olaparib initially reduced PTH levels by 40% in a patient with metastatic parathyroid carcinoma.
The patient's PTH levels eventually returned to baseline after 20 months of olaparib treatment.
The BRCA1 mutation was classified as a variant of unknown significance and not actionable.
Abstract
Parathyroid carcinoma (PC) is a rare cause of primary hyperparathyroidism with a highly variable clinical course. We report the case of a man with metastatic PC who presented with severe hypercalcemia, discovered incidentally after a fall. He underwent left upper parathyroidectomy with left thyroid lobectomy, and pathology confirmed PC. After a year of absence from follow-up, he developed recurrence with bilateral pulmonary metastases. Cinacalcet and denosumab were initiated due to persistent, severe hypercalcemia, followed by wedge resection and palliative radiotherapy of pulmonary metastases. Genetic analysis revealed no actionable pathogenic variants, but a BRCA1 mutation classified as a variant of unknown significance (VUS) was identified. He was started on olaparib, a poly adenosine diphosphate-ribose polymerase (PARP) inhibitor, 3 years after initial diagnosis. Following this, his…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
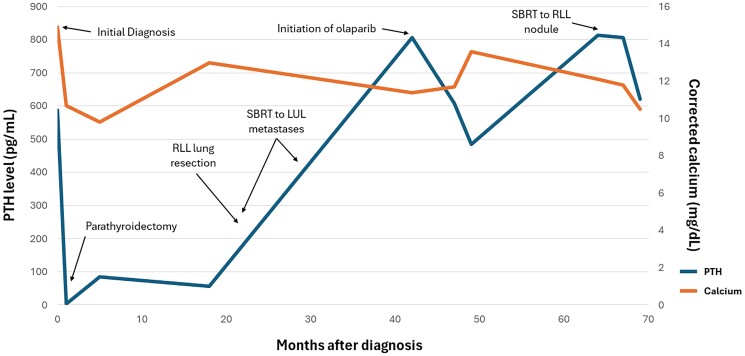 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsParathyroid Disorders and Treatments · Cancer Diagnosis and Treatment · PARP inhibition in cancer therapy
Introduction
Parathyroid carcinoma (PC) is a rare malignancy seen in 0.5% to 5% of patients with primary hyperparathyroidism [1]. Typically sporadic in occurrence, PC may also rarely occur as a feature of genetic syndromes including hyperparathyroidism-jaw tumor syndrome and multiple endocrine neoplasia types 1 and 2a. The diagnosis of PC is most commonly made postoperatively after parathyroidectomy for primary hyperparathyroidism, based on histopathological findings [1]. In patients presenting with PC, as many as 10% to 30% will have metastatic disease at the time of initial diagnosis [2]. The prognosis for metastatic PC is generally poor, though survival data are limited by the rarity of the disease. In a retrospective study of 79 patients with metastatic PC, median survival after diagnosis was 36 months, although survival ranged between 1 and 252 months [3].
Complete surgical resection of the tumor is the only known curative treatment of localized PC. Intraoperative findings suspicious for PC should prompt en bloc resection to avoid capsule rupture and excision of surrounding tissue to the lower risk of local recurrence [4]. Medical management of PC is aimed at reducing the effects of elevated PTH and, in doing so, reducing hypercalcemia, which is the primary cause of morbidity and mortality. This includes IV fluids, bisphosphonates, diuretics, and calcimimetic agents [1]. There is no clear consensus regarding the use of radiotherapy in PC. There have been no randomized controlled trials evaluating adjuvant radiotherapy, and retrospective studies have not shown benefit in survival [1]. The use of chemotherapy or immunotherapy is not part of the standard treatment of PC, as these have not been shown to be effective in either local or metastatic PC [4].
The molecular pathogenesis of PC is complex, with genetic analyses painting a highly heterogenous picture. One of the more commonly identified genetic mutations is CDC73, a tumor suppressor gene. This can be seen both as a germline mutation and, less commonly, as a somatic mutation. As a germline mutation, CDC73 is also associated with fibro-osseous jaw tumors and renal or uterine masses, collectively known as hyperparathyroidism-jaw tumor syndrome [5]. Another more frequently identified mutation is in the TP53 gene, responsible for the well-known tumor suppressor protein p53 [6]. To date, neither of these mutations has targeted therapies available.
Some mutations identified in PC, however, do have targeted therapies available. For example, up to 20% of PC samples have mutations in the PI3K/Akt/mTOR signaling pathway including TSC1, PTEN, and PIK3CA [7]. This pathway has been targeted in a patient with a TSC1 mutation who was treated with an mTOR inhibitor (everolimus) and vascular endothelial growth factor inhibitor (vandetanib), resulting in an improvement in hypercalcemia and lack of disease progression [6]. Beyond the mTOR pathway, case studies have shown that targeting mutated FGFR1 and RET with lenvatinib has led to complete biochemical remission. Additionally, targeting mutated BRCA2 with olaparib, a poly adenosine diphosphate-ribose polymerase (PARP) inhibitor, has resulted in 14 months of disease control [8]. BRCA1 and BRCA2 encode proteins necessary for homologous recombination (HR), a method of DNA repair, and mutations of these genes lead to the loss of HR. Inhibition of PARP, which facilitates DNA repair, results in increased double-strand DNA breaks that are unable to be repaired without HR, resulting in increased cell death in BRCA-mutated cancer cells [9]. Data from a small review of 11 patients with advanced PC suggested that as many as 54% of cases harbor potentially actionable mutations [6]. In absence of effective chemotherapy or immunotherapy regimens, evaluating the therapeutic utility of actionable mutations found in PC holds the key to developing effective systemic treatment strategies.
Case Presentation
A 36-year-old male presented to the emergency department following a right metacarpal fracture in the setting of a fall down a flight of stairs. Incidental laboratory findings showed hypercalcemia at 13.1 mg/dL (3.27 mmol/L) (normal reference range 8.2-10.2 mg/dL; 2.05-2.54 mmol/L). Following open reduction and internal fixation of a metacarpal fracture, he was discharged but subsequently returned to the emergency department 2 weeks later with a persistent headache and concern for pupillary abnormalities. Neurological evaluation was unrevealing, but laboratory assessment was notable for the progression of hypercalcemia to 14.8 mg/dL (3.69 mmol/L).
On further assessment, he reported several weeks of bone pain, constipation, and increased urinary frequency, but denied symptoms including changes in weight and abdominal pain. The patient's medical history included hypertension for which he was on amlodipine, and depression, for which he had been recently started on escitalopram. Before this, he had sustained a right hand and right ankle fracture in the setting of significant traumatic injury. He had no history of nephrolithiasis and no family history of hypercalcemia, nephrolithiasis, or malignancy.
Diagnostic Assessment
At initial hospitalization, serum calcium was 14.8 mg/dL (3.69 mmol/L), with PTH elevated at 620.9 pg/mL (65.8 pmol/L) (normal reference range 9.0-77.0 pg/mL; 1.0-8.2 pmol/L). Neck ultrasound revealed a 1.7 centimeter hypoechoic, hypervascular nodule with irregular margins, located within or adjacent to the left thyroid lobe.
He then underwent left upper parathyroidectomy with left hemithyroidectomy due to concern for invasion into the left thyroid lobe, along with autotransplantation of left lower parathyroid gland to the right sternocleidomastoid muscle. Intraoperatively, PTH levels decreased from 352 pg/mL (37.3 pmol/L) to 33 pg/mL (3.5 pmol/L). Pathology revealed PC with benign thyroid tissue. The diagnosis of PC was supported by several factors including a high mitotic rate, intralesional fibrosis, and probable vascular invasion. Immunohistochemistry and next-generation sequencing tests completed on this tissue sample showed microsatellite stability, PD-L1 combined positive score <1%, PMS2 G1552A, and BRCA1 C2869G mutations. The BRCA1 mutation was reported as a variant of uncertain significance (VUS).
Initial follow-up 4 months later revealed resolution of hypercalcemia [calcium 9.8 mg/dL (2.45 mmol/L)]. PTH was mildly elevated at 84.6 pg/mL (9.0 pmol/L), although in the context of low 25-OH vitamin D [11.1 ng/mL (27.7 nmol/L)] (normal reference range 30.0-100.0 ng/mL; 74.9-249.6 nmol/L), for which cholecalciferol 2000 international units daily was initiated.
He was lost to follow-up for over 1 year; upon re-establishing care, he was noted to have recurrent hypercalcemia [calcium 13.8 mg/dL (3.44 mmol/L)] and elevated PTH of 496.1 pg/mL (52.6 pmol/L). At that time, cinacalcet and denosumab were started for management of hypercalcemia. He had subsequent imaging, including a computed tomography chest, revealing multiple pulmonary nodules consistent with metastatic disease. He underwent wedge resection of a right lower lobe lung lesion, which confirmed metastatic PC. He also underwent stereotactic body radiation therapy to all remaining metastases in the left upper lung over the following 9 months.
Treatment
At 3 years after initial diagnosis, the patient was seen in follow-up by oncology. He remained on cinacalcet and denosumab in addition to IV fluid infusions 3 to 4 times a week. In light of data in the field of breast cancer, which suggested that some VUS mutations of BRCA1 respond at the same rates as pathologic mutations to PARP inhibitors, he was started on olaparib 300 mg twice daily.
Outcome and Follow-up
Following initiation of olaparib, PTH levels declined from 806.4 pg/mL (85.5 pmol/L) to a nadir of 484.0 pg/mL (51.3 pmol/L) within 7 months (Fig. 1). He continued receiving IV fluid infusions at the same frequency, as well as cinacalcet and denosumab at the same doses. Despite this initial response, his PTH began to climb subsequently and 20 months after initiation of olaparib had risen to 814.3 pg/mL (86.4 pmol/mL). Follow-up whole-body computed tomography scans revealed an enlarging right lower lobe lung nodule measuring 18 × 15 mm. He underwent stereotactic body radiation therapy of this nodule with a subsequent decline in PTH, 2 months after treatment, to 621.8 pg/mL (65.9 pmol/mL).
Timeline of PTH and albumin-corrected calcium in relation to diagnosis, procedural interventions, and olaparib therapy.Abbreviations: LUL, left upper lobe; RLL, right lower lobe; SBRT, stereotactic body radiation therapy.
Discussion
Metastatic PC is an aggressive disease with limited established treatment options, currently focused on palliative treatment of the associated comorbidities related to hypercalcemia. We present a case of a patient with metastatic PC who was treated with a PARP inhibitor olaparib after being found to have a VUS mutation of BRCA1. There are very limited data in the literature regarding BRCA mutations in PC. Another case has been reported of a patient with PC who was found to have a pathogenic, somatic BRCA2 mutation and was treated with PARP inhibitor olaparib with sustained partial response at 20 months [10]. In the case of the patient we reported, the BRCA mutation noted was BRCA1 and was a VUS, rather than pathogenic. A retrospective study in 2019 showed no significant difference in progression-free survival between patients treated with olaparib in the setting of BRCA mutations that were either known to be pathogenic vs those that were classified as VUS [11].
This patient had an initial partial response with an approximately 40% decline in PTH levels following initiation of olaparib. The response was sustained for about 20 months before PTH returned to pretreatment levels, at which time a newly enlarging lung nodule was detected. This case adds to the body of literature that underscores the importance of investigating targeted therapies based on genetic mutations in the treatment of metastatic PC.
Learning Points
Genetic testing in rare malignancies such as PC may reveal actionable targets, providing the potential for additional therapeutic options.PARP inhibitors, such as olaparib, are a reasonable systemic treatment option to consider for metastatic PC with BRCA1 mutation.Patients with VUS mutation of BRCA1 may still benefit from therapies targeting defective homologous recombination DNA repair.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Rodrigo JP, Hernandez-Prera JC, Randolph GW, et al Parathyroid cancer: an update. Cancer Treat Rev. 2020;86:102012.32247225 10.1016/j.ctrv.2020.102012 · doi ↗ · pubmed ↗
- 2Fingeret AL . Contemporary evaluation and management of parathyroid carcinoma. JCO Oncol Pract. 2021;17(1):17‐21.32040373 10.1200/JOP.19.00540 · doi ↗ · pubmed ↗
- 3Alberti A, Smussi D, Zamparini M, et al Treatment and outcome of metastatic parathyroid carcinoma: a systematic review and pooled analysis of published cases. Front Oncol. 2022;12:997009.36226055 10.3389/fonc.2022.997009 PMC 9550213 · doi ↗ · pubmed ↗
- 4Roser P, Leca BM, Coelho C, et al Diagnosis and management of parathyroid carcinoma: a state-of-the-art review. Endocr Relat Cancer. 2023;30(4):e 220287.36621911 10.1530/ERC-22-0287 · doi ↗ · pubmed ↗
- 5Li Y, Zhang J, Adikaram PR, et al Genotype of CDC 73 germline mutation determines risk of parathyroid cancer. Endocr Relat Cancer. 2020;27(9):483‐494.32590342 10.1530/ERC-20-0149 PMC 8802173 · doi ↗ · pubmed ↗
- 6Kutahyalioglu M, Nguyen HT, Kwatampora L, et al Genetic profiling as a clinical tool in advanced parathyroid carcinoma. J Cancer Res Clin Oncol. 2019;145(8):1977‐1986.31309300 10.1007/s 00432-019-02945-9PMC 11810207 · doi ↗ · pubmed ↗
- 7Marini F, Giusti F, Palmini G, Aurilia C, Donati S, Brandi ML. Parathyroid carcinoma: molecular therapeutic targets. Endocrine. 2023;81(3):409‐418.37160841 10.1007/s 12020-023-03376-w · doi ↗ · pubmed ↗
- 8Teleanu MV, Fuss CT, Paramasivam N, et al Targeted therapy of advanced parathyroid carcinoma guided by genomic and transcriptomic profiling. Mol Oncol. 2023;17(7):1343‐1355.36808802 10.1002/1878-0261.13398 PMC 10323885 · doi ↗ · pubmed ↗