The Linear Association of Chest Radiograph Opacification With Both Respiratory Physiology and Systemic Inflammation in Hospital In‐Patients With Covid‐19 Infection
Colin J. Crooks, Dominick Shaw, Timothy R. Card, Iain Au‐Yong, Yutaro Higashi, Elisabetta Giannotti, Andrew W. Fogarty

TL;DR
This study shows that chest X-ray opacification in COVID-19 patients correlates with breathing difficulties and inflammation levels.
Contribution
It demonstrates a linear association between chest radiograph opacification and both respiratory and inflammatory markers in hospitalized COVID-19 patients.
Findings
Chest radiograph opacification correlated with oxygen saturation and supplementary oxygen requirements (r = -0.38).
Opacification also correlated with serum C-reactive protein levels (r = +0.33).
The median opacification was 20% with a wide interquartile range (5–45%).
Abstract
Chest radiographs are generally used for diagnostic purposes. They also have potential to quantify disease severity. This analysis tested the hypothesis that there was an association between chest radiograph opacification and measures of respiratory physiological status and systemic inflammation in patients with Covid‐19 infection. Data on chest radiograph opacification were compared with concurrent measures of oxygen requirements and saturation and serum C‐reactive protein. Data were available from 628 individuals. The median opacification on chest radiographs was 20% (interquartile range 5–45). This was associated both SFR (oxygen saturation/supplementary oxygen) with an r value of −0.38 (95% confidence intervals CI: −0.45 to −31, Pearson's correlation coefficient) and CRP (+0.33; 95% CI: +0.24 to +0.41, Pearson's correlation coefficient). Chest radiograph opacification scores are…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
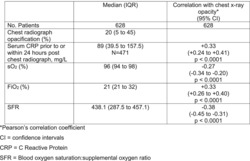 Figure 1
Figure 1| Median (IQR) | Correlation with chest X‐ray opacity | |
|---|---|---|
| No. of patients | 628 | 628 |
| Chest radiograph opacification (%) | 20 (5–45) | |
| Serum CRP prior to or within 24‐h post–chest radiograph, mg/L |
89 (39.5–157.5)
|
+0.33 (+0.24 to +0.41)
|
| sO2 (%) | 96 (94–98) |
−0.27 (−0.34 to −0.20)
|
| FiO2 (%) | 21 (21–32) |
+0.33 (+0.26 to +0.40)
|
| SFR | 438.1 (287.5–457.1) |
−0.38 (−0.45 to −0.31)
|
- —University of Nottingham 10.13039/501100000837
- —Nottingham University Hospitals NHS Trust 10.13039/100011330
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsUltrasound in Clinical Applications · Pneumonia and Respiratory Infections · Emergency and Acute Care Studies
Introduction
1
The development of chest radiographs in the early 20th century was a landmark achievement that has been seamlessly integrated into mainstream clinical practice. Clinicians use their experience to integrate the information provided by the chest radiograph into the heuristic diagnostic process that utilises all available clinical information on the patient. This will inevitably include a degree of assessment of disease severity using a variety of parameters including the amount of chest radiograph opacification. A number of studies have explored the concept of radiograph opacity scoring systems for respiratory diseases [1] including in patients with Covid‐19 infection [2, 3, 4, 5]. One study from Italy reported that radiograph opacification was negatively associated with blood oxygen saturation and positive associated with systemic inflammation in patients with Covid‐19 infection [6].
We used data on a cohort of patients admitted to hospital with Covid‐19 infection to quantify the association between objective measures of chest radiograph opacification with respiratory failure severity and systemic inflammation.
Methods
2
Data were available for all adult patients admitted to Nottingham University Hospitals NHS Trust with a diagnosis of Covid‐19 infection from June 2020 to December 2021 [7]. Chest radiographs taken on admission to hospital from a subset of this cohort were scored by the reporting radiologist using a simple visual estimate of the total percentage of lung parenchymal opacification as previously described [8]. Data were extracted on the closest pulse oximeter oxygen saturation, supplementary oxygen requirements and serum C‐reactive protein (CRP) prior to the chest radiograph. If serum CRP was not measured prior to the chest radiograph, the first measurement within 24 h following the chest radiograph was used.
Pearson's product–moment correlation coefficients were calculated between the measures of chest radiograph opacification and both of the two measures of respiratory failure and systemic inflammation. Finally, we fitted separate probit models predicting percentage opacification for SFR and CRP, with adjustment for age and sex.
Results
3
Data were available from 628 individuals with observations available (Table 1). The median opacification score on chest radiographs was 20% (interquartile range 5–45). This was associated with both the measures of severity of respiratory failure and the measures of systemic inflammation. Specifically, the SFR (oxygen saturation/supplementary oxygen and the measure of severity of respiratory failure) was associated with the chest radiograph opacification score with an r value of −0.38 (95% confidence intervals CI: −0.45 to −31, p < 0.0001, Pearson's correlation coefficient), and the serum CRP (the measure of systemic inflammation) had a r value of +0.33 (95% CI: +0.24 to +0.41, p < 0.0001, Pearson's correlation coefficient). After adjusting for age and sex in multivariate probit models, both SFR and CRP were strongly associated with the chest X‐ray appearances (SFR, p < 0.0001 and CRP, p < 0.0001).
Discussion
4
Our analysis quantified the nature and size of the associations between chest radiograph opacification and measures of both respiratory failure and systemic inflammation in patients with Covid‐19 infection.
The strength of this analysis is that data were collected on an unselected population of all patients admitted with Covid‐19 infection, with no awareness of the hypothesis to be tested, thus reducing the risk of bias. The quantification of the chest radiograph opacification by radiologists, again with no awareness of the hypothesis being tested, minimises the risk of bias. The analysis was done in patients with Covid‐19 infection and hence may not be generalisable to individuals outside this patient group. One limitation of the analysis was the absence of baseline premorbid radiographs to quantify preexisting opacification that is not due to Covid‐19 infection. This introduces the possibility of some measurement error for the radiograph opacification attributable to Covid‐19 infection, which may reduce the strength of some of the correlations we observed.
The analysis shows relatively strong associations between the extent of chest radiograph opacification and both the degree of respiratory failure and systemic inflammation. A correlation coefficient of 0.3 suggests that the opacification is associated with approximately 9% of the variance in respiratory failure and systemic inflammation observed in patients with Covid‐19 infection. This is of a similar magnitude to that reported in a population of patients with Covid‐19 infection from Italy [6]. The use of the SFR [9] provided a measure of hypoxaemia that has been validated in Covid‐19 patients [10] and is a prognostic measure of the risk of clinical deterioration [11]. Systemic serum CRP is also an independent risk factor for mortality in Covid‐19 patients [12].
Conclusion
5
These data demonstrate that as well as providing qualitative or diagnostic clinical information, chest radiographs' utility in patients with Covid‐19 infection extends to providing quantitative insights into concurrent disease severity, as measured in terms of both respiratory failure and systemic inflammation levels. This scoring complements and probably contributes to the ability of the chest radiograph scoring to contribute to the understanding of the clinical status of patients with Covid‐19 infection [8].
Author Contributions
The concept was developed by AF and DS. I A‐Y, EG and YH provided scores for the radiographs. CC did the analysis. All authors contributed to the manuscript.
Ethics Statement
Approval for this work was granted via an NUH Clinical Effectiveness Team audit (Reference: 21‐294C) and IRAS (REC: 20/WM/0142, project ID: 282490, Amendment No. SA02 20/07/21).
Conflicts of Interest
The authors declare no conflicts of interest.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1M. A. Warren , Z. Zhao , T. Koyama , et al., “Severity Scoring of Lung Oedema on the Chest Radiograph Is Associated With Clinical Outcomes in ARDS,” Thorax 73, no. 9 (2018): 840–846, 10.1136/thoraxjnl-2017-211280.29903755 PMC 6410734 · doi ↗ · pubmed ↗
- 2M. Hanley , C. Brosnan , D. O'Neill , et al., “Modified Brixia Chest X‐Ray Severity Scoring System and Correlation With Intubation, non‐invasive Ventilation and Death in a Hospitalised COVID‐19 Cohort,” Journal of Medical Imaging and Radiation Oncology 66, no. 6 (2022): 761–767, 10.1111/1754-9485.13361.34845851 · doi ↗ · pubmed ↗
- 3R. Kaleemi , K. Hilal , A. Arshad , et al., “The Association of Chest Radiographic Findings and Severity Scoring With Clinical Outcomes in Patients With COVID‐19 Presenting to the Emergency Department of a Tertiary Care Hospital in Pakistan,” P Lo S ONE 16, no. 1 (2021): e 0244886, 10.1371/journal.pone.0244886.33400723 PMC 7785233 · doi ↗ · pubmed ↗
- 4A. Venugopalan Nair , D. Kumar , M. Mc Innes , et al., “Utility of Chest Radiograph Severity Scoring in Emergency Department for Predicting Outcomes in COVID‐19: A Study of 1275 Patients,” Clinical Imaging 95 (2023): 65–70, 10.1016/j.clinimag.2022.12.002.36623355 PMC 9794386 · doi ↗ · pubmed ↗
- 5R. A. Reeves , C. Pomeranz , A. A. Gomella , et al., “Performance of a Severity Score on Admission Chest Radiography in Predicting Clinical Outcomes in Hospitalized Patients With Coronavirus Disease (COVID‐19),” AJR American Journal of Roentgenology 217, no. 3 (2021): 623–632, 10.2214/ajr.20.24801.33112201 · doi ↗ · pubmed ↗
- 6C. G. Monaco , F. Zaottini , S. Schiaffino , et al., “Chest x‐Ray Severity Score in COVID‐19 Patients on Emergency Department Admission: A Two‐Centre Study,” European Radiology Experimental 4, no. 1 (2020): 68, 10.1186/s 41747-020-00195-w.33319321 PMC 7735892 · doi ↗ · pubmed ↗
- 7C. Crooks , J. West , A. Fogarty , et al., “Predicting Need for Escalation of Care or Death From Repeated Daily Clinical Observations and Laboratory Results in Patients With SARS‐Co V‐2,” American Journal of Epidemiology 191 (2022): 1944–1953.35872596 10.1093/aje/kwac 126PMC 9384527 · doi ↗ · pubmed ↗
- 8I. Au‐Yong , Y. Higashi , E. Giannotti , et al., “Chest Radiograph Scoring Alone or Combined With Other Risk Scores for Predicting Outcomes in COVID‐19,” Radiology 302, no. 2 (2022): 460–469, 10.1148/radiol.2021210986.34519573 PMC 8475750 · doi ↗ · pubmed ↗