Electrocardiogram challenge: pericardial effusion
Sinead Rosser, William Orr, C Fielder Camm

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
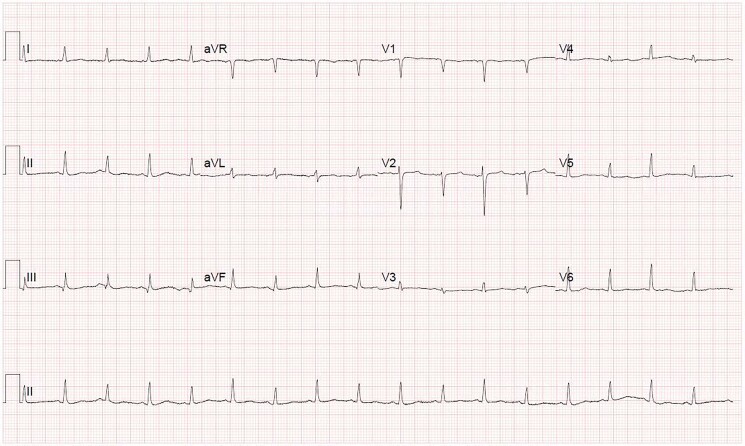 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPericarditis and Cardiac Tamponade · Cardiac Structural Anomalies and Repair · Cardiac pacing and defibrillation studies
A 41-year-old female presented to the emergency department with vomiting and shortness of breath. She has a background history of lung cancer with bone and brain metastases. A CT head showed progressive disease with new cerebral metastases, a chest X-ray showed a large left pleural effusion, and her blood tests showed an acute kidney injury. She was started on i.v. dexamethasone and was awaiting urgent drainage of the pleural effusion. Despite appropriate management, she had ongoing tachycardia of 120 b.p.m., blood pressure 140/100, and a 2L O2 requirement. An electrocardiogram (ECG) was done, which is demonstrated below.
Correct answer: B) Electrical alternans—electrical alternans is an ECG finding of alternating size of the QRS complex between beats. This can be identified in any or all leads on an ECG.^1^ In the ECG seen above, electrical alternans is most evident in lead V2. Alternating amplitude of the T waves can sometimes be present as well.
Correct answer: A) Pericardial effusion—in large pericardial effusions and cardiac tamponade, the heart swings in a pendulum-like motion as it beats, and therefore it alternates between moving towards the ECG electrode, and away from it, hence creating the variation in amplitude of the QRS complexes detected by the ECG and resulting in electrical alternans.^1^ This can be evidenced further in the supplementary video provided (see Supplementary material online, Video S1).
Correct answer: E) Pericardial window—when there is recurrence of pericardial effusion despite pericardiocentesis, the option of a pericardial window should be considered. This can be achieved either surgically or via percutaneous balloon pericardiotomy.^2^ This creates a direct communication between the pericardial sac and the pleural fluid to allow the pericardial fluid to drain and prevent accumulation and tamponade.^3^ Management should also involve addressing the underlying aetiology of the pericardial effusion to prevent recurrence if possible.
Supplementary Material
ytaf055_Supplementary_Data
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Ingram D , Strecker-Mc Graw MK. Electrical Alternans. Treasure Island (FL): Stat Pearls Publishing. Stat Pearls—NCBI Bookshelf; 2023. Available from: https://www.ncbi.nlm.nih.gov/books/NBK 534229/30480962 · pubmed ↗
- 2Imazio M , Adler Y. Management of pericardial effusion. Eur Heart J 2012;34:1186–1197.23125278 10.1093/eurheartj/ehs 372 · doi ↗ · pubmed ↗
- 3Adler Y , Charron P, Imazio M, Badano L, Barón-Esquivias G, Bogaert J, et al 2015 ESC Guidelines for the diagnosis and management of pericardial diseases. Eur Heart J 2015;36:2921–2964.26320112