Pulmonary Tuberculosis-Associated Morbidity in Africa: A Systematic Review
Collins C Okeke, Chiemezie C Ibe, Oluchi J Nduji, Chizoba J Ndulue, Onyinye Ngige, Chukwunomso C Amuchie, Chinecherem C Ezema, Afamefuna O Onyeogulu, Angela Ojo, Michael Obuseh, Omosimisola O Alli, Emmanuel I Akinteye, Kris N Idion, Ubon I Akpan-Udo, Isabella C Okereke

TL;DR
This study reviews the health problems linked to pulmonary tuberculosis in Africa, focusing on mental health, lung issues, and other comorbidities.
Contribution
The study highlights unique TB-related morbidities like secondary amenorrhea and medication-induced psychosis in African populations.
Findings
Mental illness was the most reported morbidity among pulmonary TB patients in Africa.
Comorbidities like HIV, diabetes, and chronic pulmonary conditions worsen TB outcomes.
Unique conditions such as secondary amenorrhea and medication-induced psychosis were identified as TB-related complications.
Abstract
Tuberculosis (TB) remains a global health problem despite the availability of effective medications and preventive measures. TB in humans is caused by Mycobacterium tuberculosis (MTB) and usually affects the lungs causing pulmonary TB. It is transmitted via M. tuberculosis-containing aerosol droplets and nuclei. TB has a devastating effect on Africa and this review aims to identify the most common morbidities associated with and the sequelae/complications of pulmonary TB in Africa and also explore a management option to decrease the impact of morbidity/complications and increase quality of life. A comprehensive search conducted from inception to the 5th of December 2024 on PubMed, Scopus, and African Journal Online returned 6312 for which 1441 duplicates were removed. Four thousand, eight hundred seventy-one articles were screened and 4791 articles were removed following title and…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
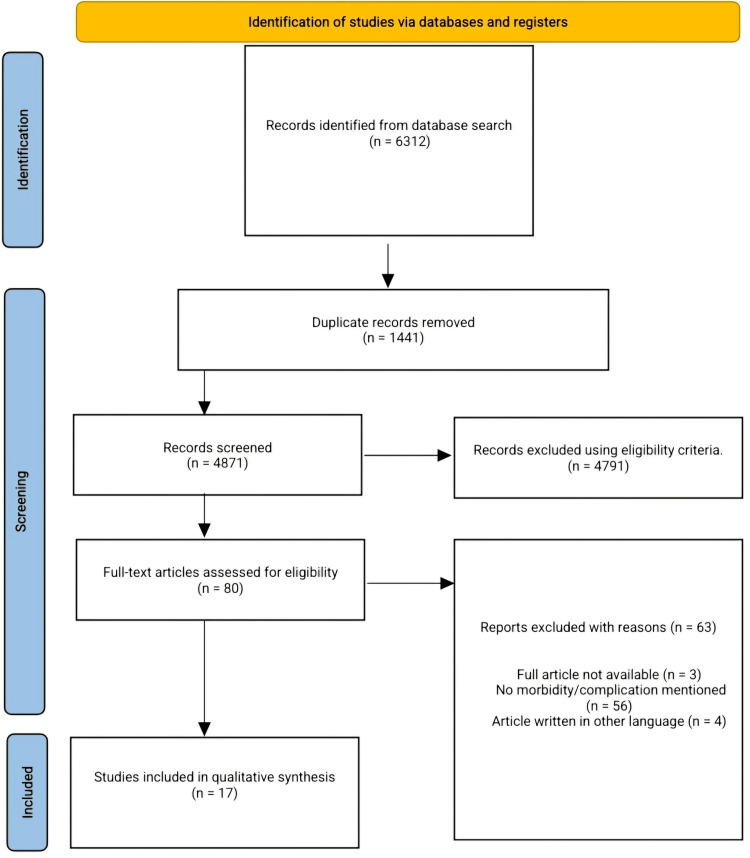 Figure 1
Figure 1| Author | Year | Country | Sample size | Mean age | Male | Female |
| Kehbila et al. [ | 2015 | Cameroon | 265 | 37 | 129 | 136 |
| Osman et al. [ | 2017 | South Africa | 51 | 40 | 32 | 19 |
| Ayana et al. [ | 2018 | Ethiopia | 365 | 36 | 205 | 160 |
| Hestad et al. [ | 2019 | Zambia | 38 | 34 | 25 | 13 |
| Ilesanmi et al. [ | 2017 | Nigeria | 152 | 41 | 85 | 67 |
| Philips et al. [ | 2014 | South Africa | 59 | 33 | 48 | 11 |
| Nkereuwem et al. [ | 2019 | Gambia | 68 | 6.5 | 36 | 32 |
| Binegdie et al. [ | 2013 | Ethiopia | 134 | 40 | 72 | 62 |
| Namusobya et al. [ | 2021 | Uganda | 162 | 30 | 97 | 65 |
| Kirenga et al. [ | 2013 | Uganda | 365 | 29 | 158 | 207 |
| Aghanwa and Erhabor [ | 1996 | Nigeria | 53 | 37 | 24 | 29 |
| Mkoko et al. [ | 2016 | South Africa | 173 | 50 | 103 | 70 |
| Goussard et al. [ | 2011 | South Africa | 250 | 1.1 | 144 | 106 |
| Lasebikan and Ige [ | 2014 | Nigeria | 115 | 35 | 44 | 71 |
| Hassan and Darwish [ | 2008 | Egypt | 429 | 41 | 85 | 67 |
| Hayes-Larson et al. [ | 2015 | Lesotho | 371 | 35 | 212 | 160 |
| Theron et al. [ | 2012 | South Africa, Zimbabwe, Zambia, and Tanzania | 1502 | 37 | 859 | 643 |
| Author | Morbidity |
|
Kehbila et al. [ | Depression |
|
Osman et al. [ | Shortness of breath, severe chest illness, wheezing |
|
Ayana et al. [ | Psychological distress |
|
Hestad et al. [ | Cognitive impairment |
|
Ilesanmi et al. [ | Depression |
|
Philips et al. [ | Insulin resistance |
|
Nkereuwem et al. [ | Lung impairment |
|
Binegdie et al. [ | Post-TB fibrosis, post-TB bronchiectasis, aspergilloma, post-TB granuloma pleural thickening, tuberculosis-related lung destruction |
|
Namusobya et al. [ | Chronic pulmonary aspergillosis |
|
Kirenga et al. [ | Parenchymal nodules, infiltrates, masses p parenchymal cavities pleural effusion |
|
Aghanwa and Erhabor [ | Depression, generalized anxiety, adjustment disorder |
|
Mkoko et al. [ | Chronic lung disease |
|
Goussard et al. [ | Airway obstruction |
|
Lasebikan and Ige [ | Schizophrenia, non-affective psychosis, medication-induced psychotic disorder |
|
Hassan and Darwish [ | Secondary amenorrhea, hypomenorrhea, intermenstrual spotting, menorrhagia, dysmenorrhea |
|
Hayes-Larson et al. [ | Depression, harmful alcohol use |
|
Theron et al. [ | Psychological distress |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsTuberculosis Research and Epidemiology · Pneumocystis jirovecii pneumonia detection and treatment · Infectious Diseases and Tuberculosis
Introduction and background
Despite the availability of effective medications and preventive measures, tuberculosis (TB) remains a deeply entrenched global health problem. Gram-positive, acid-fast bacilli belonging to the genus Mycobacterium are the cause of TB, a progressive granulomatous infectious illness. Mycobacterium tuberculosis is the main cause of TB in humans, which mostly affects the lungs and results in pulmonary TB. It can also cause extra-pulmonary TB by affecting the skin, lymph nodes, bones, joints, gut, meninges, and other bodily parts. The primary methods of human TB transmission are droplet infection and droplet nuclei [1]. Globally, individuals are afflicted by the deadly infectious TB. Even though low- and middle-income nations account for almost 80% of occurrences, TB is nevertheless a problem globally.
In 2022, 46% of new cases of TB were in the Southeast Asian Region, according to the World Health Organization (WHO). Africa came in second at 23%, while the Western Pacific area had 18% of new cases [2].
An estimated 25% of people worldwide are thought to have contracted TB. Of those infected with TB, 5-10% will eventually develop symptoms and TB illness. The number of deaths from TB in 2023 was 1.25 million, including 161,000 HIV-positive individuals. In addition to being the largest cause of death for individuals with HIV and a significant contributor to antimicrobial resistance, TB has likely reclaimed its position as the world’s leading infectious agent-related cause of death. An estimated 10.8 million persons worldwide contracted TB in 2023, comprising 1.3 million children, 3.6 million women, and 6.0 million men. All nations and age groups are affected by TB. TB is preventable and cured. According to the 2023 UN high-level level meeting on TB, approximately 22 billion US dollars are required each year for TB prevention, diagnosis, treatment, and care in order to fulfill the worldwide objective by 2027 [3].
TB is the most common infectious agent and the ninth-largest cause of death globally, surpassing HIV/AIDS. Africa accounts for more than one-third of TB-related deaths. Multidrug-resistant TB (MDR-TB) is a danger to health security and raises the possibility of undoing progress in the fight against TB [2]. There were an expected 424,000 TB deaths (1.267 million worldwide) and 2.5 million TB illnesses in the African continent in 2022, which accounted for a quarter of all new TB cases worldwide. In Africa, TB accounts for more than one-third of all fatalities [2]. Between 2015 and 2022, the incidence of TB decreased by 23% globally and by -8.7% in the African region. This must be accelerated in order to meet the End TB Strategy’s 2025 goals, which include a 50% decrease in incidence from 2015. Between 2010 and 2022, TB diagnosis and treatment are predicted to have saved 44 million lives worldwide, with 10 million of those lives occurring in the African region [2]. Nigeria still holds the position of the country with the highest TB burden in West Africa with an absolute estimated incidence of 407,000 cases in 2016 [4]. Tanzania, Kenya, and Uganda are among the high TB burden countries in East Africa with reported TB incidence rates of 292, 253, and 200 per 100,000 population respectively in 2018 [5]. In North Africa, the highest prevalence rates of TB were in Egypt at 28935.42 [6]. South Africa has a particularly high burden of TB, with an incidence rate of 468 per 100,000 of the population [7].
Active TB patients can spread the disease by coughing, sneezing, or talking, which releases aerosol droplets and nuclei containing MTB. The TB bacteria enter the new host's lungs through the respiratory system after being inhaled. Alveolar macrophages then internalize the tubercle bacilli while the host's innate immune system comes in to ward off the infection. When the macrophages fail to inhibit or destroy the bacilli, the bacteria multiply within their intracellular environment, get released, and then are phagocytosed again by other alveolar macrophages and the cycle continues. Following the recruitment of lymphocytes to the infection site, a swarm of immune cells comes in an effort to contain the bacteria and prevent further growth, initiating a cell-mediated immune response. The host is still asymptomatic at this point, and the TB bacteria may either go into latency inside the granuloma or be totally eradicated. However, in the setting of impaired immunity, the disease immediately progresses into active TB with clinical symptoms [8]. Common symptoms of active lung TB are cough with sputum and blood at times, chest pains, weakness, weight loss, fever, and night sweats [9]. WHO recommends the use of rapid molecular diagnostic tests as the initial diagnostic test in all persons with signs and symptoms of TB while tuberculin skin test (TST), interferon-gamma release assay (IGRA), or newer antigen-based skin tests (TBST) can be used to identify people with infection. TB is treated with special antibiotics, commonly used are: isoniazid, rifampicin, pyrazinamide, and ethambutol. For effectiveness, medications need to be taken daily for 4-6 months [3].
This systematic review aims to identify the most common morbidities associated with and the sequelae/complications of pulmonary TB in Africa and also explore a management option to decrease the impact of morbidity/complications and increase quality of life.
Review
Methods
The Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) extension for systematic reviews [10] were followed in the course of this systematic review. The study protocol was registered with Prospero CRD42024625260.
Inclusion Criteria
We included original articles published in English in peer-reviewed journals from inception to November 2024 that reported morbidity/sequelae among patients of all ages and genders in Africa diagnosed with pulmonary TB via culture and currently receiving treatment and or have completed standardized treatment.
Exclusion Criteria
Patients were managed in a hospital outside Africa, and study designs such as case reports, audits, opinions, reviews, meta-analyses, letters, comments, and editorials were excluded.
A comprehensive search was conducted from inception to the 5th of December 2024, on PubMed, Scopus, and African Journal Online(AJOL). The keywords used were ((Pulmonary tuberculosis) AND (Morbidity)) AND (Africa), ((Pulmonary tuberculosis) AND (complications)) AND (Africa), "Pulmonary Tuberculosis" "Morbidity" "Africa" and "Pulmonary Tuberculosis" "Complication" "Africa" as shown in the Appendix Table 3.
Three independent reviewers (C.C.O, C.C.I, O.J.N) performed duplicate, title, and abstract screening against the predefined eligibility criteria using the Rayyan systematic review software [11]. Potentially eligible studies were screened for full-text review. Disagreements were discussed among reviewers; in the case of no resolution, an appeal was made to another reviewer (C.J.N).
We extracted data from articles related to the author, study year, study design, sample size, mean age, gender, anti-TB medication, comorbidity, and morbidity. The risk of bias in included studies was assessed using the JBI critical appraisal tool for cross-sectional and cohort. JBI’s critical appraisal tools assist in assessing published papers’ trustworthiness, relevance, and results. This appraisal aims to assess a study's methodological quality and determine the extent to which a study has addressed the possibility of bias in its design, conduct, and analysis. Articles are assessed with a yes, no, unclear, and not applicable as shown in the appendix Tables 4-5 [12]. The randomized control trials were accessed using the Scottish Intercollegiate Guidelines Network (SIGN) assessment tool [13] and articles were assessed with a yes, no, and can’t say. A ++ is assigned to a high-quality article, + is assigned to an acceptable article, a - is assigned to a poor-quality article and 0 is assigned to an unacceptable article, as shown in Appendix Table 6.
Results
Our search returned 6312 articles, 1441 articles were removed following duplicate screening and 4871 were screened. 4791 articles were excluded after the title and abstract screening using the eligibility criteria, and 80 articles were subjected to full-text screening to determine their eligibility based on our inclusion criteria. Ultimately, 17 articles were included in the final qualitative synthesis. Exclusions were made due to various reasons, including failure to meet our inclusion criteria, unavailability of full articles, unavailability of morbidity/complications of pulmonary TB mentioned in an article, and articles written in other languages (French language). Figure 1 displays the PRISMA flow diagram.
PRISMA flow diagramThe image was created by the authors of this article.
Study characteristics
A total of 4552 patients were included in 17 articles, from 11 countries in Africa (Cameroon, South Africa, Ethiopia, Zambia, Nigeria, Gambia, Uganda, Egypt, Lesotho, Zimbabwe, and Tanzania). South Africa produced the highest number of articles (5), followed by Nigeria (3), then Ethiopia, Uganda, and Zambia producing two articles each. The study period ranged from 1996 to 2021 and the mean age of patients reported ranged from 1.1 to 50 years across the studies. There were 2358 males and 1918 females diagnosed with pulmonary TB. The study characteristics of the included articles are shown in Table 1.
The study with the largest sample size was 1502 [30], while 38 was the smallest sample size in these studies [17]. The study types included in this review are cross-sectional studies [14-23], prospective and retrospective cohort studies [24-27], randomized control trials [28], mixed-method cluster-randomized trials [29], and randomized parallel-arm, multi-centric trials [30].
Morbidity
From the included articles, mental illness was the most reported morbidity(depression, psychological distress, generalized anxiety, adjustment disorder, schizophrenia, psychosis), followed by lung impairment, and then airway obstruction. Other reported morbidity can be seen in Table 2. HIV, asthma, and chronic obstructive pulmonary airway disease were the most common comorbidities reported in this study [14-18,20,22,23,25,26,29,30]. Other comorbidities included diabetes [23], pneumonia [26], chicken pox [22], and heart-related disease [14].
Discussion
This systematic review synthesizes data from 17 studies across 11 African countries, encompassing 4552 patients, and provides an in-depth analysis of the morbidities and comorbidities associated with pulmonary TB. The findings align with existing global evidence and reveal unique regional and demographic patterns, offering valuable insights for clinical practice and public health interventions in African contexts. Pulmonary TB presents with varying morbidity as seen in this study which includes psychological illness(depression, psychological distress, schizophrenia, non-affective psychosis, medication-induced psychotic disorder, generalized anxiety, adjustment disorder), respiratory/lung impairments (lung impairment, post-TB fibrosis, post-TB bronchiectasis, aspergilloma, post-TB granuloma, pleural thickening, TB-related lung destruction, parenchymal nodules, parenchymal infiltrates, parenchymal masses, parenchymal cavities, pleural effusion, airway obstruction, chronic lung disease, shortness of breath and wheezing), also rare morbidities like cognitive impairment, insulin resistance, harmful alcohol use then menstrual abnormalities and comorbidity (HIV, asthma, chronic obstructive pulmonary disease (COPD), pneumonia, diabetes, chicken pox, and heart-related disease) profiles across different economic settings.
Demographic Insights: Gender, Age, and Geography
This study offers valuable insights into the demographic distribution. Male predominance (2358 males vs. 1918 females) aligns with global trends suggesting higher TB incidence in males due to biological and behavioral factors. However, the inclusion of pediatric data, such as the study by Goussard et al. [26] with a mean age of 1.1 years, highlights the often-overlooked burden of TB in children. This contrasts with many studies that predominantly focus on adult populations [31,32]. In high-income countries (HICs), TB disproportionately affects marginalized populations, including immigrants, refugees, and people experiencing homelessness, regardless of gender. Pediatric TB is rare due to effective vaccination programs and low community transmission rates. This contrasts with the findings in low- and middle-income countries (LMICs), which have a greater demographic impact according to the WHO report [2].
Geographically, South Africa’s contribution to five studies reflects its high TB burden and research capacity. The inclusion of data from less-represented countries like Gambia and Lesotho adds diversity to the analysis, addressing gaps in TB research from low-resource settings.
Psychological Morbidities: A Growing Concern
The prominence of mental health disorders, particularly depression, anxiety, and psychological distress, among TB patients in this study, is consistent with global trends. Studies such as those by Pachi et al. [33], have documented the interplay between TB and mental health, emphasizing how stigma, chronic disease burden, and socio-economic factors heighten psychological distress. However, our study expands the scope by including less commonly reported conditions like schizophrenia, psychosis, and medication-induced psychotic disorders, which have been underexplored in the literature. In LMICs, mental health morbidities are often driven by poverty, stigma, and limited access to mental health services. Less commonly reported disorders, including schizophrenia and psychosis, were also highlighted, possibly reflecting the compounded mental health burden in resource-limited settings. Similar trends of depression and anxiety have been documented among TB patients in HICs [33]. However, the severity of mental health outcomes is often lower due to robust mental health infrastructure and earlier detection and intervention. Additionally, the stigma associated with TB is less pronounced in HICs, where TB incidence is lower, and public awareness is higher [33-35]. This highlights the need for targeted mental health screening and interventions in TB care settings, particularly in resource-limited environments where mental health services are often scarce.
Respiratory Morbidities: Granularity in Clinical Outcomes
Respiratory sequelae, including post-TB fibrosis, bronchiectasis, airway obstruction, and chronic pulmonary aspergillosis, emerged as critical long-term complications. These findings are consistent with prior studies such as Pasipanodya et al. [36], which underscore the high prevalence of lung impairment among TB survivors. However, the detailed categorization of respiratory morbidities in this study enhances the clinical understanding of TB's pulmonary impact, particularly in African populations. Although post-TB lung disease is also prevalent in HICs, the severity is typically lower due to earlier diagnosis, more effective treatments, and access to pulmonary rehabilitation programs [36]. Studies in HICs often report milder forms of airway obstruction or restrictive lung disease compared to the advanced structural lung damage seen in LMICs [37,38]. The inclusion of specific conditions like aspergilloma and TB-related lung destruction highlights the need for post-treatment pulmonary rehabilitation programs to mitigate long-term morbidity.
Comorbidities: HIV and Beyond
The high prevalence of HIV co-infection in the reviewed studies corroborates existing epidemiological data from sub-Saharan Africa, where HIV and TB co-epidemics continue to pose significant public health challenges. This is consistent with findings by Suthar et al [31], which demonstrated the synergistic burden of HIV and TB on morbidity and mortality. Beyond HIV, this study identifies a range of comorbidities, including diabetes, pneumonia, and cardiovascular diseases, reflecting the complex interplay of TB with non-communicable diseases. Unlike LMICs, HICs show that diabetes and COPD are the most commonly reported comorbidities, reflecting the aging populations and higher prevalence of non-communicable diseases in HICs [39]. HIV co-infection is less prominent due to widespread access to antiretroviral therapy (ART) and lower HIV prevalence. Other conditions, such as chronic kidney disease and immunosuppression related to organ transplantation, are more relevant in HIC populations [2]. These findings emphasize the importance of integrated care models that address both infectious and chronic conditions to improve patient outcomes.
Recommendation
The findings of this review emphasize the need for a multidimensional approach to addressing pulmonary TB and its associated morbidities, particularly in resource-limited settings. Based on the results, the following recommendations are proposed for improving research, clinical practice, and public health interventions: Integration of mental health services into TB care by incorporating routine mental health screening and support services into TB treatment programs. Mental health interventions, such as cognitive behavioral therapy and pharmacological treatments, can improve adherence to TB medications and patient outcomes. Healthcare workers should be trained to recognize and manage mental health disorders in TB patients, with clear referral pathways to mental health specialists. Strengthening post-treatment pulmonary rehabilitation programs through the development and expansion of post-TB rehabilitation services to address long-term pulmonary complications, such as fibrosis, bronchiectasis, and airway obstruction. Multidisciplinary teams, including pulmonologists and physiotherapists, should be established to provide rehabilitation services, including spirometry monitoring, respiratory exercises, and oxygen therapy.
Enhancing diagnostic and treatment capacity in LMICs by investing in diagnostic infrastructure and access to advanced treatment options to reduce delays in diagnosis and improve outcomes. Scaling up molecular diagnostic tools like GeneXpert MTB/RIF and ensuring equitable access to TB medications.
Expanding research into underexplored TB morbidities by conducting focused research on less commonly reported TB-related morbidities, such as menstrual irregularities, medication-induced psychosis, and secondary infections like chickenpox. Longitudinal cohort studies should track the emergence and progression of these morbidities and investigate their underlying mechanisms.
Prioritizing pediatric TB in research and policy by increasing research and policy focus on pediatric TB, with attention to the unique morbidities and management challenges in children. Developing child-specific TB diagnostic tools, strengthening vaccination programs, and studying the long-term effects of TB on child growth and development are essential steps forward.
Scaling up public health interventions to reduce TB incidence by focusing on preventive strategies, including universal bacillus Calmette-Guérin (BCG) vaccination and production of a new and effective vaccine that will reduce the incidence of TB, improve nutrition, and reduce socio-economic barriers to TB care. Community-based awareness campaigns strengthened TB contact tracing programs, and patient incentives for early diagnosis and treatment adherence are critical components of effective prevention.
Creating integrated care models for chronic TB sequelae via the establishment of integrated care models to address chronic TB-related conditions such as diabetes, COPD, and cardiovascular disease. Coordinated care programs that incorporate TB treatment with chronic disease management should be supported by cross-specialty training for healthcare providers.
Promoting linguistic and geographic inclusivity in research by including studies published in non-English languages to better represent francophone and other underrepresented regions in Africa. Journals should support multilingual submissions and collaborations with researchers from underrepresented linguistic regions through discounts or waivers in research publications.
Study strengths and limitations
The review encompasses a wide range of study designs, including cross-sectional studies, cohort studies, and randomized controlled trials. This methodological diversity strengthens the robustness of the findings, offering both prevalence estimates and insights into causality. However, the exclusion of French-language studies is a limitation that may have introduced regional bias, particularly given the significant TB burden in francophone African countries [40]. Future reviews should strive for linguistic inclusivity to provide a more comprehensive synthesis.
Conclusions
This study provides a comprehensive synthesis of the morbidities and comorbidities associated with pulmonary TB across African populations, highlighting significant clinical, demographic, and regional insights. The findings underscore the profound impact of TB on mental health, respiratory function, and systemic health, exacerbated by comorbidities such as HIV, diabetes, and chronic pulmonary conditions. Additionally, the review reveals unique morbidities like secondary amenorrhea and medication-induced psychosis, often overlooked in global TB research, and emphasizes the burden of TB among pediatric and underrepresented populations.
The analysis highlights critical disparities in TB outcomes between resource-limited and high-income settings, underscoring the role of healthcare infrastructure, diagnostic capacity, and social determinants in shaping disease outcomes. The persistence of severe respiratory complications, compounded by delays in diagnosis and treatment, calls for a stronger focus on rehabilitation and integrated care models to address chronic sequelae.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1An overview on epidemiology of tuberculosis Mymensingh Med J Khan MK Islam MN Ferdous J Alam MM 259266282019 https://pubmed.ncbi.nlm.nih.gov/30755580/30755580 · pubmed ↗
- 2Tuberculosis (TB) | WHO | Regional Office for Africa [Internet] 11 2024 2024 https://www.afro.who.int/health-topics/tuberculosis-tb
- 3Tuberculosis (TB) 12 2024 2024 https://www.who.int/news-room/fact-sheets/detail/tuberculosis
- 4Burden of tuberculosis and challenges facing its eradication in West Africa Int J Infect Adebisi YA Agumage I Sylvanus TD 062019 https://brieflands.com/articles/iji-92250.html
- 5Gaps related to screening and diagnosis of tuberculosis in care cascade in selected health facilities in East Africa countries: A retrospective study J Clin Tuberc Other Mycobact Dis Mnyambwa NP Philbert D Kimaro G 100278252021 https://pubmed.ncbi.nlm.nih.gov/34622035/3462203510.1016/j.jctube.2021.100278 PMC 8481961 · doi ↗ · pubmed ↗
- 6Epidemiological features of tuberculosis in the Middle East and North Africa from 1990 to 2019: Results from the global burden of disease Study 2019 Afr Health Sci Moradinazar M Afshar ZM Ramazani U Shakiba M Shirvani M Darvishi S 366375232023 https://pubmed.ncbi.nlm.nih.gov/38357127/3835712710.4314/ahs.v 23i 3.43PMC 10862560 · doi ↗ · pubmed ↗
- 7WHO: Intensifying efforts to end TB 12 2024 2024 https://www.afro.who.int/countries/south-africa/news/south-africa-intensifying-efforts-end-tb
- 8Tuberculosis: Pathogenesis, current treatment regimens and new drug targets Int J Mol Sci Alsayed SS Gunosewoyo H 5202242023 https://pubmed.ncbi.nlm.nih.gov/36982277/3698227710.3390/ijms 24065202 PMC 10049048 · doi ↗ · pubmed ↗