Systemic Bacillus Calmette-Guérin (BCG) Infection in a Patient With Non-Muscle-Invasive Bladder Cancer: A Case Report
Ana S Ramoa Oliveira, Raquel Afonso, Eduardo Macedo, Bernardo Silvério, Ana Oliveira

TL;DR
A patient with bladder cancer developed a rare systemic BCG infection after treatment, highlighting the need for early diagnosis and proper care.
Contribution
This case report highlights the rare but severe complication of systemic BCG infection following standard bladder cancer therapy.
Findings
Systemic BCG infection can occur despite a normal immune system and may initially be misdiagnosed.
Antituberculosis treatment successfully resolved the infection after proper diagnosis.
Persistent fever without an obvious source should prompt consideration of BCG infection in treated patients.
Abstract
Intravesical Bacillus Calmette-Guérin (BCG) instillation is a widely used adjuvant therapy for non-muscle-invasive bladder cancer (NMIBC), typically associated with a favorable safety profile. However, severe complications such as systemic BCG infection, though rare, can occur and are potentially life-threatening. Diagnosing systemic BCG infection is challenging due to frequently negative microbiological results. We report the case of a 67-year-old immunocompetent man who developed a systemic BCG infection after undergoing BCG therapy for NMIBC. Initially misdiagnosed as a urinary tract infection, his condition worsened despite antibiotic treatment. The diagnosis of BCG sepsis was suspected after prolonged fever, asthenia, and other systemic symptoms. Prompt initiation of antituberculosis treatment with rifampicin, ethambutol, and isoniazid led to a full recovery. This case underscores…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
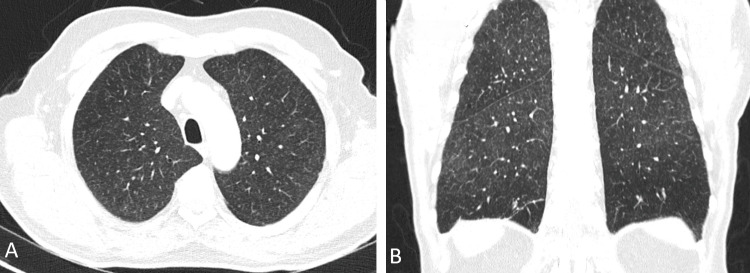 Figure 1
Figure 1| Parameter | Patient's Value | Normal Range |
| PaO2 (arterial oxygen) on admission | 50 mmHg | 75-100 mmHg |
| pH (arterial blood gas) on admission | 7.51 | 7.35-7.45 |
| pCO2 (arterial blood gas) on admission | 30 mmHg | 35-45 mmHg |
| Hemoglobin on admission | 14.4 g/dL | 13.5-17.0 g/dL |
| Leukocytes on admission | 5.100 uL | 4.0-11.0 uL |
| Aspartate aminotransferase on admission | 78 U/L | 10-40 U/L |
| Alanine aminotransferase on admission | 73 U/L | 7-56 U/L |
| Gamma-glutamyl transferase on admission | 50 U/L | 9-48 U/L |
| Alkaline phosphatase on admission | 83 U/L | 44-121 U/L |
| Total bilirubin on admission | 0.7 mg/dL | 0.1-1.2 mg/dL |
| Direct bilirubin on admission | 0.2 mg/dL | 0-0.3 mg/dL |
| Lactate dehydrogenase on admission | 318 U/L | 120-246 U/L |
| Urea on admission | 47 mg/dL | 19-49 mg/dL |
| Creatinine on admission | 1.7 mg/dL | 0.6-1.2 mg/dL |
| C-reactive protein on admission | 105.3 mg/L | <5 mg/L |
| Anti-HIV antibodies | Negative | - |
| Hepatitis B surface antigen | Negative | - |
| Anti-hepatitis B surface antibody | Negative | - |
| Anti-hepatitis B core antibody | Negative | - |
| Anti-HCV antibodies | Negative | - |
| VDRL | Negative | - |
| Antinuclear antibodies | Negative | - |
| Anti-dsDNA antibodies | Negative | - |
| Anti-LKM-1 antibodies | Negative | - |
| Anti-liver cytosol antibodies | Negative | - |
| Anti-soluble liver antigen | Negative | - |
| Anti-mitochondrial antibodies | Negative | - |
| Rheumatoid factor | Negative | - |
| Anti-cyclic citrullinated peptide antibodies | Negative | - |
| Anti-neutrophil cytoplasmic antibodies | Negative | - |
| Anti-basement membrane antibodies | Negative | - |
| IgG | 1200 mg/dL | 700-1600 mg/dL |
| IgM | 80 mg/dL | 40-230 mg/dL |
| IgA | 100 mg/dL | 70-400 mg/dL |
| C3 | 121 mg/dL | 90-180 mg/dL |
| C4 | 35 mg/dL | 10-40 mg/dL |
| Blood cultures | Negative | - |
| Urine mycobacteriological analysis | Negative | - |
| Sputum mycobacteriological analysis | Negative | - |
| Sputum microbiological analysis | Negative | - |
| Urine microbiological analysis | Negative | - |
| Detection of mycobacteria by polymerase chain reaction | Negative | - |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsBladder and Urothelial Cancer Treatments · Urinary Tract Infections Management · Urinary and Genital Oncology Studies
Introduction
Intravesical Bacillus Calmette-Guérin (BCG) therapy, utilizing a live attenuated strain of Mycobacterium bovis, is the most effective treatment for high- or intermediate-risk non-muscle-invasive bladder cancer (NMIBC) [1-3]. Administered via urethral catheterization, BCG reduces the risk of recurrence and progression, improving long-term survival [1,2]. Though generally well tolerated, BCG can cause local and systemic complications [3-7]. Acute symptoms like fever, dysuria, and mild hematuria are common, typically resolving within 48 hours [3]. However, severe complications, including granulomatous prostatitis, pneumonitis, and sepsis, are rare but can be life-threatening [5-7].
Systemic BCG infection, although uncommon, may arise when the attenuated bacteria disseminate beyond the bladder [3-6]. It often presents with nonspecific symptoms such as fever, weight loss, and night sweats, making diagnosis challenging [3-6]. Without prompt treatment, it can lead to severe outcomes [3-6].
This case underscores the importance of vigilance in patients undergoing BCG therapy, particularly when symptoms persist despite standard antibiotic treatment. Early recognition and intervention are crucial to prevent severe outcomes associated with systemic BCG infections.
Case presentation
A 67-year-old man with a history of hypertension, dyslipidemia, type 2 diabetes, and heavy smoking (50 pack-year) underwent transurethral resection of the bladder. Histological analysis revealed high-grade papillary urothelial carcinoma. Imaging studies confirmed the absence of locoregional or metastatic disease. He was prescribed a three-year adjuvant schedule of intravesical immunotherapy with BCG instillations, consisting of a six-week induction course (once weekly), followed by maintenance doses (once weekly for three weeks) at three, six, 12, 18, 24, 30, and 36 months. Follow-up cystoscopies were scheduled every three months.
The initial treatments were uneventful. However, 12 months into therapy, two days after the 14th treatment, he developed macroscopic hematuria, suprapubic pain, and fever. Major complications were ruled out, and he was discharged with a course of amoxicillin/clavulanic acid (875 mg/125 mg every 12 hours). Despite treatment, his symptoms persisted, prompting a return to the emergency department.
A computed tomography (CT) scan of the thorax, abdomen, and pelvis excluded significant complications, and he was discharged with a second antibiotic, considering a possible urinary tract infection (ciprofloxacin 500 mg every 12 hours). When symptoms continued unabated, he was hospitalized and treated with a seven-day course of intravenous ceftriaxone (2 g once daily) for a possible urinary infection. Urine cultures remained consistently negative throughout.
Despite multiple courses of antibiotics, the patient’s symptoms persisted, warranting further evaluation. Further questioning revealed significant weight loss over the previous month, worsening asthenia, occasional fever spikes (maximum 38.9ºC), and night sweats.
On physical examination, he presented with hypotension (BP: 90/35 mmHg), tachycardia (HR: 120 bpm), and inspiratory crackles on pulmonary auscultation. Arterial blood gas analysis showed hypoxemia with respiratory alkalosis (Table 1). Thoracic CT imaging showed "diffuse micronodular peribronchovascular interstitial thickening in both lungs, suggestive of a nonspecific inflammatory process" (Figure 1). Laboratory tests (Table 1) indicated hepatitis without cholestasis, as well as acute kidney injury. Multiorgan dysfunction was evident, with cardiovascular, hepatic, renal, and pulmonary involvement.
Computed tomography. Axial (A) and coronal (B) images showing expanded lungs with peribronchovascular interstitial thickening of diffuse micronodular appearance in both lungs, suggestive of a nonspecific inflammatory process of the small airways. No pulmonary consolidations are present.
Despite extensive evaluation, including serological and immunological tests, all markers were negative, and cultures failed to identify an infectious agent. Based on the clinical findings and the patient’s history, a diagnosis of systemic BCG infection was strongly suspected.
Given the temporal association with BCG instillation and the presence of multiorgan dysfunction, a presumptive diagnosis of BCG sepsis was made. Antituberculosis therapy was initiated with rifampicin (600 mg once daily), ethambutol (1200 mg once daily), and isoniazid (300 mg once daily). The patient showed rapid improvement and was discharged after 23 days of hospitalization. Antituberculosis therapy was continued for six months without side effects, and BCG immunotherapy was permanently discontinued. There was no evidence of infection recurrence or cancer at the one-year follow-up.
Discussion
Intravesical instillation of BCG is a widely effective adjuvant therapy for NMIBC [1,2]. It is generally well tolerated, with limited and self-limiting adverse effects [1,2,7]. However, severe complications, such as systemic BCG infection, are rare but life-threatening [5-7]. Despite these complexities, BCG immunotherapy remains the most effective treatment for NMIBC [1,2].
The exact mechanism of systemic BCG infection remains unclear, with proposed hypotheses including Mycobacterium bovis dissemination and immune hypersensitivity reactions [3,8]. Histopathological and clinical distinctions between infection and hypersensitivity remain difficult in many cases [8].
Disseminated BCG infection, although rare, represents a potentially fatal complication of BCG therapy [3,5-7]. It is not always preceded by visible traumatic catheterization, although this is a known risk factor [3,9]. Adverse effects from intravesical BCG instillation can manifest immediately or even years after the procedure [7,9].
BCG infection typically presents with persistent fever, weight loss, and night sweats, often weeks to months after therapy [3]. Symptoms may mimic tuberculosis or other systemic infections. Diagnosis relies heavily on clinical suspicion, as the sensitivity of acid-fast bacillus smear and mycobacterial culture is limited [3,5,10,11]. The development of a new, highly sensitive, and specific real-time PCR assay can improve the detection of Mycobacterium tuberculosis complex isolates in specimens [11,12]. However, in our case, as in other reviewed cases, the PCR test yielded negative results [3]. Therefore, in cases with high clinical suspicion, treatment should be initiated promptly, as was done for our patient, without waiting for laboratory confirmation.
When evaluating the risk of systemic infection, it is crucial to recognize that BCG instillation immediately following transurethral resection of a bladder tumor or traumatic catheterization is an absolute contraindication [9]. Furthermore, BCG therapy should be postponed in patients presenting with fever or suspected urinary tract infections until these symptoms resolve [9]. Routine pre-procedure urinalysis is recommended to enhance patient safety, even in asymptomatic individuals [9]. While immunosuppression, such as in HIV-positive patients, is frequently considered a relative contraindication to BCG therapy, studies by Herr and Dalbagni have demonstrated that BCG immunotherapy remains both effective and safe for immunocompromised cancer patients [13].
This case highlights a disseminated BCG infection evolving with multiorgan dysfunction due to delays in diagnosis. It is important to emphasize the delay in diagnosis and the potential dangers of not suspecting systemic BCG infection early, especially when symptoms are misattributed to more common conditions like a urinary tract infection, leading the patient to undergo multiple cycles of antibiotic therapy unnecessarily. We use this case to highlight to all general clinicians that a high index of suspicion should be raised for systemic dissemination in patients presenting with persistent fever, accompanied by fatigue and night sweats, who are currently under BCG treatment or have undergone it in the past.
Treatment typically involves a combination of antituberculosis medications, although the optimal duration of therapy has not yet been definitively established [8]. In cases of multisystemic involvement, corticosteroid therapy should also be considered, although no standardized regimen has been recommended [3].
Conclusions
Disseminated BCG infection is a rare but serious complication of intravesical BCG therapy. Early diagnosis is challenging due to the frequent absence of positive cultures, making clinical history crucial. Prompt initiation of antituberculosis therapy often leads to rapid recovery. Clinicians should maintain a high index of suspicion in patients with persistent fever and other systemic symptoms, as early intervention significantly improves outcomes.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Terapêutica intravesical com bacilo de Calmette-Guérin no tratamento do carcinoma da bexiga: o que sabemos até agora Acta Urol Port Santos JC Rolim N Rodrigues T 7581312014
- 2Efficacy and safety of bacille Calmette-Guérin immunotherapy in superficial bladder cancer Clin Infect Dis Lamm DL 09031 Suppl 3200010.1086/31406411010830 · doi ↗ · pubmed ↗
- 3Systemic infection following intravesical therapy with BCGBMJ Case Rep Oliveira AA Morais J Ribeiro J Gouveia PF 014202110.1136/bcr-2021-243641 PMC 857893634753717 · doi ↗ · pubmed ↗
- 4Systemic Bacillus Calmette-Guérin (BCG) infection with renal involvement: A rare complication of BCG immunotherapy Cureus Afonso R Fontes J Pinto P Romano M Esteves A 014202210.7759/cureus.33134 PMC 988637736726926 · doi ↗ · pubmed ↗
- 5Favorable outcome in a patient with systemic BC Gitis after intra-bladder instillation of Calmette-Guerin Bacillus highlighting the importance of making the correct diagnosis in this rare form of sepsis J Transl Int Med Attou R Albrich T Kadou J Redant S HonoréPM De Bels D 3438720193099735510.2478/jtim-2019-0007 PMC 6463824 · doi ↗ · pubmed ↗
- 6Granulomatous hepatitis following intra-vesical instillation of Bacillus Calmette-Guérin for treatment of bladder cancer Infect Dis Rep Branco EA Duro R Brito T Sarmento A 6116181320213428734010.3390/idr 13030057 PMC 8293128 · doi ↗ · pubmed ↗
- 7Incidence and treatment of complications of Bacillus Calmette-Guerin intravesical therapy in superficial bladder cancer J Urol Lamm DL van der Meijden PM Morales A 5966001471992153843610.1016/s 0022-5347(17)37316-0 · doi ↗ · pubmed ↗
- 8Uncommon but clinically significant: Bacillus Calmette-Guerin (BCG) infection of the urinary tract and its impact on quality of life Am J Case Rep Shibutani K Ishikawa K Mori N 024202310.12659/AJCR.940375 PMC 1040534737537854 · doi ↗ · pubmed ↗