A Challenging Case of Biliary Obstruction in an 82-Year-Old Male With a History of Zollinger-Ellison Syndrome and Suspected Cholangiocarcinoma Secondary to Biliary Candidiasis
Muhammad Waqar Elahi, Mona Ghias, Asif Haris, David Shi

TL;DR
An 82-year-old man with a complex medical history had biliary obstruction caused by a rare fungal infection, highlighting the need to consider fungal infections in similar cases.
Contribution
The case highlights the importance of diagnosing biliary candidiasis in high-risk patients with biliary obstruction.
Findings
Biliary candidiasis was identified as the cause of cholangitis and sepsis in a patient with complex medical history.
A multidisciplinary approach was crucial for accurate diagnosis despite initial diagnostic challenges.
Abstract
Biliary obstruction is a serious condition with various underlying causes, including malignancy, infection, and gallstones. Fungal biliary infections are rare, frequently misdiagnosed, and carry significant morbidity and mortality. Here, we present the case of an 82-year-old male with multiple comorbidities who developed sepsis secondary to cholangitis. Despite initial diagnostic challenges and the complexity of his biliary anatomy due to prior surgeries, a multidisciplinary approach identified biliary candidiasis as the underlying cause of cholangitis and sepsis. This case underscores the importance of considering fungal infections in the differential diagnosis of biliary obstruction, particularly in high-risk and immunosuppressed patients. Early recognition is essential to enable prompt treatment and improve patient outcomes.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
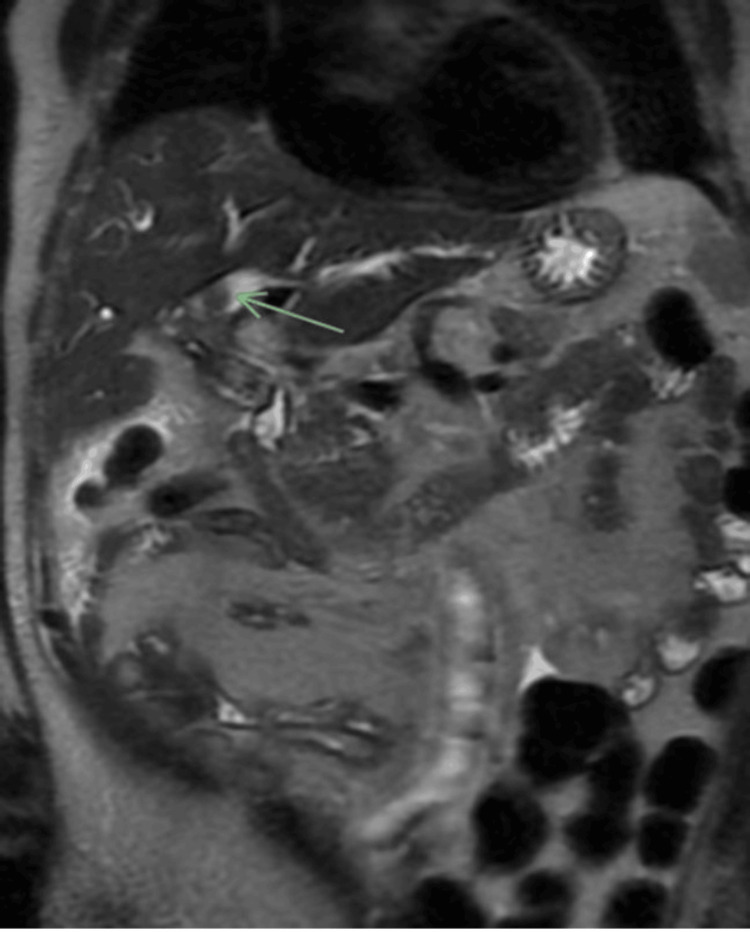 Figure 1
Figure 1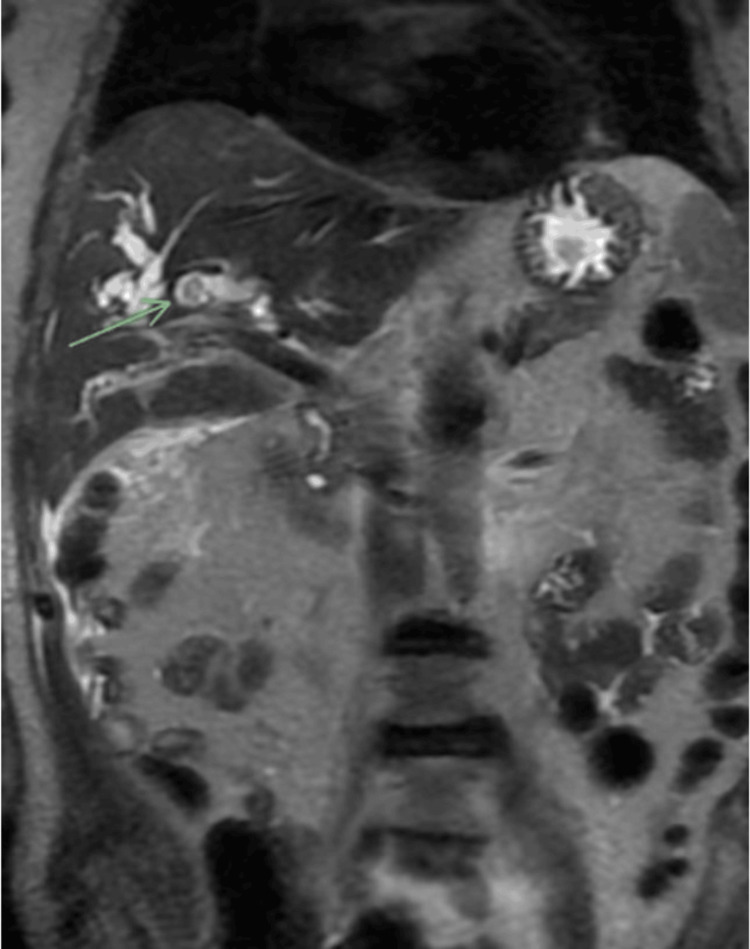 Figure 2
Figure 2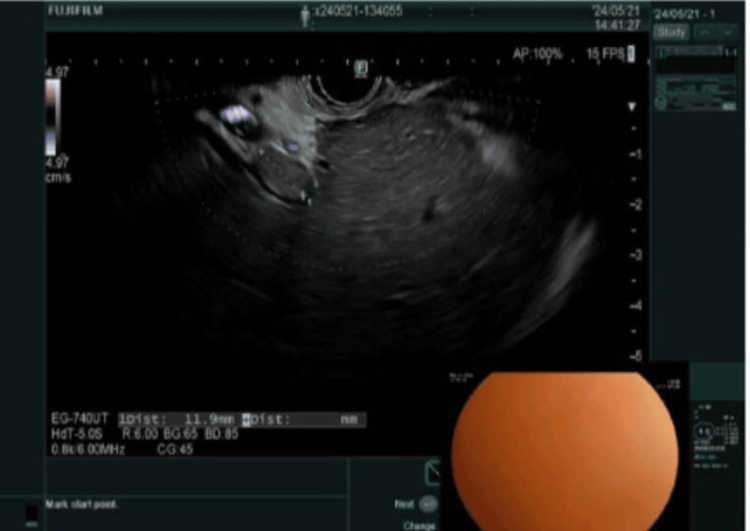 Figure 3
Figure 3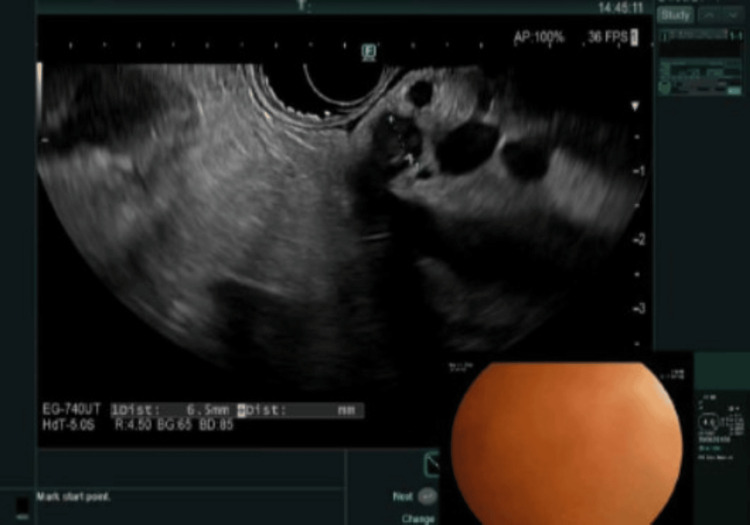 Figure 4
Figure 4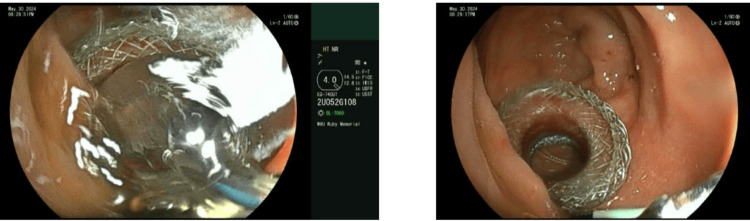 Figure 5
Figure 5| Parameter | Result | Reference value |
| White blood cell count | 14.1 × 10⁹/L | 3.7-11 × 10⁹/L |
| C-reactive protein | 117.6 mg/L | ≤8.0 mg/L |
| Procalcitonin, serum | 3.24 ng/mL | <0.5 ng/mL |
| Bilirubin, total | 2.9 mg/dL | 0.3-1.3 mg/dL |
| Bilirubin, conjugated | 1.1 mg/dL | <0.3 mg/dL |
| Aspartate aminotransferase (SGOT) | 160 U/L | 8-48 U/L |
| Alanine transaminase (SGPT) | 154 U/L | <55 U/L |
| Alkaline phosphatase | 340 U/L | 45-115 U/L |
| Creatinine | 1.67 mg/dL | 0.62-1.27 mg/dL |
| Blood urea nitrogen | 29 mg/dL | 8-25 mg/dL |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAntifungal resistance and susceptibility · Pneumocystis jirovecii pneumonia detection and treatment · Cystic Fibrosis Research Advances
Introduction
Biliary obstruction, a blockage of the bile ducts, can lead to serious complications such as cholangitis (infection of the bile ducts), jaundice (yellowing of the skin and eyes), and liver damage. While cholangiocarcinoma, a cancer of the bile ducts, is a well-recognized cause of biliary obstruction, fungal infections of the biliary tree are exceedingly rare. Biliary obstruction caused by fungal infection is particularly uncommon and sparsely documented in the literature [1]. Most reported cases of biliary candidiasis have occurred in patients with underlying malignancies, diabetes mellitus, or other immunosuppressive conditions, such as cystic fibrosis [1]. Biliary candidiasis should prompt suspicion for biliary or regional malignancy, necessitating a thorough workup to confirm or rule out such diagnoses and facilitate timely treatment [1]. Here, we present the case of an 82-year-old male with multiple comorbidities who exhibited signs and symptoms of sepsis secondary to cholangitis. Further evaluation revealed biliary candidiasis as the underlying cause of his cholangitis.
Case presentation
The patient was an 82-year-old male with a complex medical history, including major depressive disorder, coronary artery disease, hypertension, cerebrovascular accident, Zollinger-Ellison syndrome status post tumor resection, Roux-en-Y gastrojejunostomy, Alzheimer’s dementia, and benign prostatic hyperplasia. He presented to the emergency room with altered mental status after nursing home staff noted increased confusion compared to his baseline. Upon presentation, the patient was alert and oriented only to person. His blood pressure was low at 86/59 mmHg, while other vital signs were within normal limits.
Significant laboratory values are presented in Table 1.
The patient underwent a magnetic resonance cholangiopancreatography, which revealed marked intrahepatic biliary ductal dilatation with a central filling defect, highly concerning for cholangiocarcinoma (Figure 1, Figure 2).
Intraluminal filling defect within the intrahepatic ducts observed on a coronal SSFSE sequenceSSFSE, single-shot fast spin-echo
Suggestion of an additional intraluminal filling defect within the intrahepatic ducts on coronal SSFSE sequenceSSFSE, single-shot fast spin-echo
The patient was found to be in sepsis, likely secondary to cholangitis. Blood cultures grew Escherichia coli, and he was started on ertapenem. Gastroenterology was consulted. On the fifth day of hospitalization, the patient underwent endoscopic ultrasound (EUS) and endoscopic retrograde cholangiopancreatography (ERCP), but the procedure was aborted due to difficult cannulation related to his prior Roux-en-Y hepaticojejunostomy. EUS revealed intrahepatic biliary ductal dilation with intraductal sludge (Figure 3) and an apparent surgical transection of the proximal common bile duct (CBD; Figure 4).
Intraductal sludge
Proximal CBDCBD, common bile duct
A multidisciplinary conference was held, and the decision was made to proceed with the creation of a gastrojejunostomy using a lumen-apposing metal stent (LAMS) to facilitate subsequent EUS-directed transenteric ERCP. After a few days, the advanced endoscopy team successfully created the gastrojejunostomy using LAMS, and the stent was dilated to 18 mm (Figure 5).
LAMS with dilationLAMS, lumen-apposing metal stent
A week later, EUS-directed transenteric ERCP was performed, which revealed a single localized biliary stricture in the lower third of the main bile duct, along with choledocholithiasis, which was completely removed by balloon extraction. Cytology brushing at the site of the stricture was negative for malignancy but showed fungal organisms morphologically consistent with Candida species. Biliary candidiasis was treated with a 14-day course of fluconazole.
Discussion
Biliary obstruction and cholangitis are common clinical issues, with bacterial infections being the typical cause. However, in recent years, involvement of the biliary tract by *Candida *and other fungal species has been increasingly reported [2]. “Biliary candidiasis” refers to yeast infection within the biliary tract, although cases remain limited to a few reports and case series.
The clinical manifestations of *Candida *infection can range from localized disease to widespread, disseminated infections with multisystem organ failure. Candida albicans is the most common species implicated, although other species can also cause severe infections [3]. Fungal infections have also been associated with CBD obstruction [4,5].
Risk factors for biliary candidiasis include immunosuppression, diabetes, prolonged antibiotic therapy, extended critical care stays, ERCP [6], and the use of external biliary shunts/endoprostheses [7]. Other independent risk factors for intra-abdominal candidiasis include intra-abdominal surgeries, gut perforation, anastomotic leakage, and the presence of an abdominal drain [8].
Due to challenges in obtaining bile samples, our knowledge of bile duct microbial flora remains limited. Moreover, it is unclear whether positive fungal findings represent true infection or simple colonization, as Candida is considered part of the normal microbiota in the gastrointestinal and genitourinary tracts of humans [3]. A prospective observational study by Lenz et al. [2] concluded that positive fungal cultures are not mere contamination artifacts, especially in patients with significant risk factors. The study also suggested that previous biliary tract manipulation may increase the risk of biliary tract infections [1,9]. Treatment typically involves bile duct drainage and antifungal therapy.
This case underscores the complexities of managing biliary obstruction, particularly in patients with confounding medical histories and altered biliary anatomy. Biliary candidiasis can closely mimic cholangiocarcinoma, complicating the diagnostic process. This case highlights the importance of considering both possibilities, especially in patients with risk factors for fungal infections. Furthermore, EUS-guided techniques, such as gastrojejunostomy creation, can be valuable tools in overcoming anatomical challenges and achieving successful biliary intervention.
Conclusions
This case illustrates the successful application of a multidisciplinary approach, including EUS with gastrojejunostomy creation followed by transenteric ERCP, to manage a challenging biliary obstruction in a patient with a complex medical history. The patient was septic and diagnosed with biliary candidiasis. This case emphasizes the importance of considering biliary candidiasis as a potential cause of biliary obstruction, particularly in high-risk patients.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Intractable biliary candidiasis in patients with obstructive jaundice and regional malignancy: a retrospective case series Clin Exp Gastroenterol Al Manasra AR Jadallah K Aleshawi A 83891420213370796210.2147/CEG.S 301340 PMC 7941053 · doi ↗ · pubmed ↗
- 2Prevalence, associations, and trends of biliary-tract candidiasis: a prospective observational study Gastrointest Endosc Lenz P Conrad B Kucharzik T 4804877020091955593510.1016/j.gie.2009.01.038 · doi ↗ · pubmed ↗
- 3Candida infections of the abdomen and thorax Baddley JW, Hall KK, ed. Up To Date. Waltham MA: Up To Date 7 2024 Kauffman CA 2024202024 https://www.uptodate.com/contents/candida-infections-of-the-abdomen-and-thorax
- 4Common bile duct obstruction due to candidiasis Scand J Gastroenterol Domagk D Bisping G Poremba C Fegeler W Domschke W Menzel J 444446362001 https://pubmed.ncbi.nlm.nih.gov/11336173/1133617310.1080/003655201300051397 · doi ↗ · pubmed ↗
- 5Common bile duct obstruction due to an intraluminal mass of candidiasis in a previously healthy child Pediatrics Carstensen H Nilsson KO Nettelblad SC Cederlund CG Hildell J 858861771986 https://pubmed.ncbi.nlm.nih.gov/3520470/3520470 · pubmed ↗
- 6Candida cholecystitis as an unusual complication of endoscopic retrograde cholangiography Endoscopy Takano H Yoshikawa T Nishida K 79079128199610.1055/s-2007-10056179007446 · doi ↗ · pubmed ↗
- 7Gallbladder and biliary tract candidiasis Surgery Diebel LN Raafat AM Dulchavsky SA Brown WJ 7607641201996886238910.1016/s 0039-6060(96)80028-6 · doi ↗ · pubmed ↗
- 8Risk factors for intra-abdominal candidiasis in intensive care units: results from EUCANDICU study Infect Dis Ther Bassetti M Vena A Giacobbe DR 8278401120223518235310.1007/s 40121-021-00585-6PMC 8960530 · doi ↗ · pubmed ↗