Effectiveness of mouthwashes to reduce the SARS-COV-2 load in saliva of adults with diagnosis of COVID-19: Systematic review and meta-analysis
Rosita Elena Espejo-Carrera, Angel Steven Asmat-Abanto, Marcos Jimmy Carruitero-Honores, José Antonio Caballero-Alvarado

TL;DR
This study reviews whether mouthwashes can reduce SARS-CoV-2 viral load in saliva of adults with COVID-19.
Contribution
It provides a meta-analysis comparing the effectiveness of three mouthwash types in reducing viral load.
Findings
Overall, mouthwashes did not significantly reduce SARS-CoV-2 viral load in saliva.
Povidone-iodine (PVP-I) showed a significant reduction in viral load compared to other mouthwashes.
Cetylpyridinium chloride (CPC) and chlorhexidine (CHX) did not show significant reductions in viral load.
Abstract
COVID-19 still represents a threat to public health. In this sense, antiseptic mouthwashes have been suggested to reduce cross-contamination and community transmission. This systematic review and meta-analysis aimed to synthesize the evidence on the effectiveness of povidone-iodine (PVP-I), cetylpyridinium chloride (CPC) and chlorhexidine (CHX) mouthwashes in reducing SARS-COV-2 viral load in the saliva of adults diagnosed with COVID-19. After the systematic search in five electronic databases, 16 clinical trials published until June 2023 were analyzed. Of these, 6 were included in the meta-analysis. The standardized mean difference (SMD) was reported with its corresponding 95% confidence intervals (95%CI). An overall SMD of 0.51 (95%CI: -0.29 to 1.32; I² = 46.0%; p = 0.047) was found. For CPC, the combined effect found in the studies was not significant (SMD = -0.07; 95%CI: -0.42 to…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
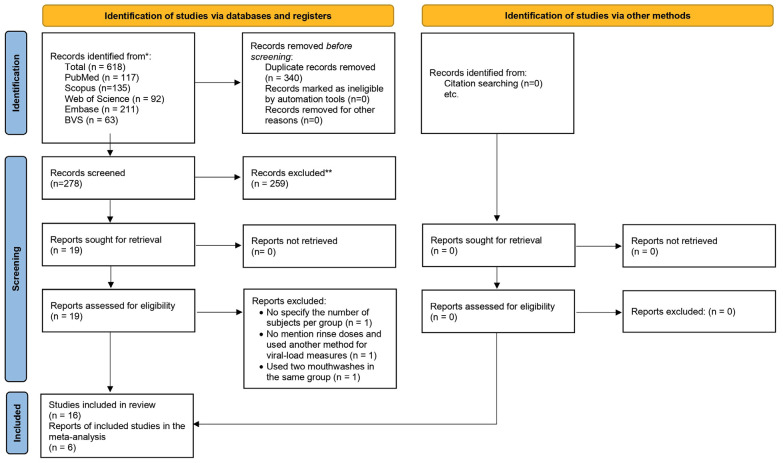 Figure 1
Figure 1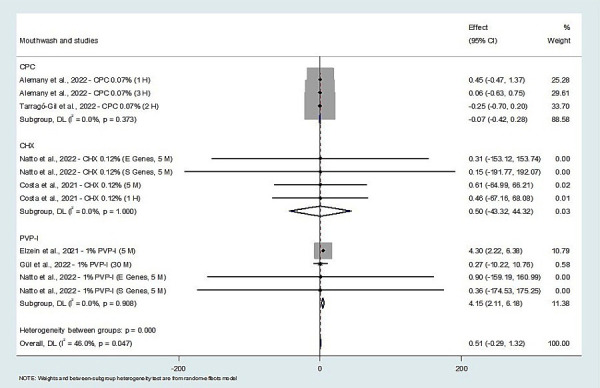 Figure 2
Figure 2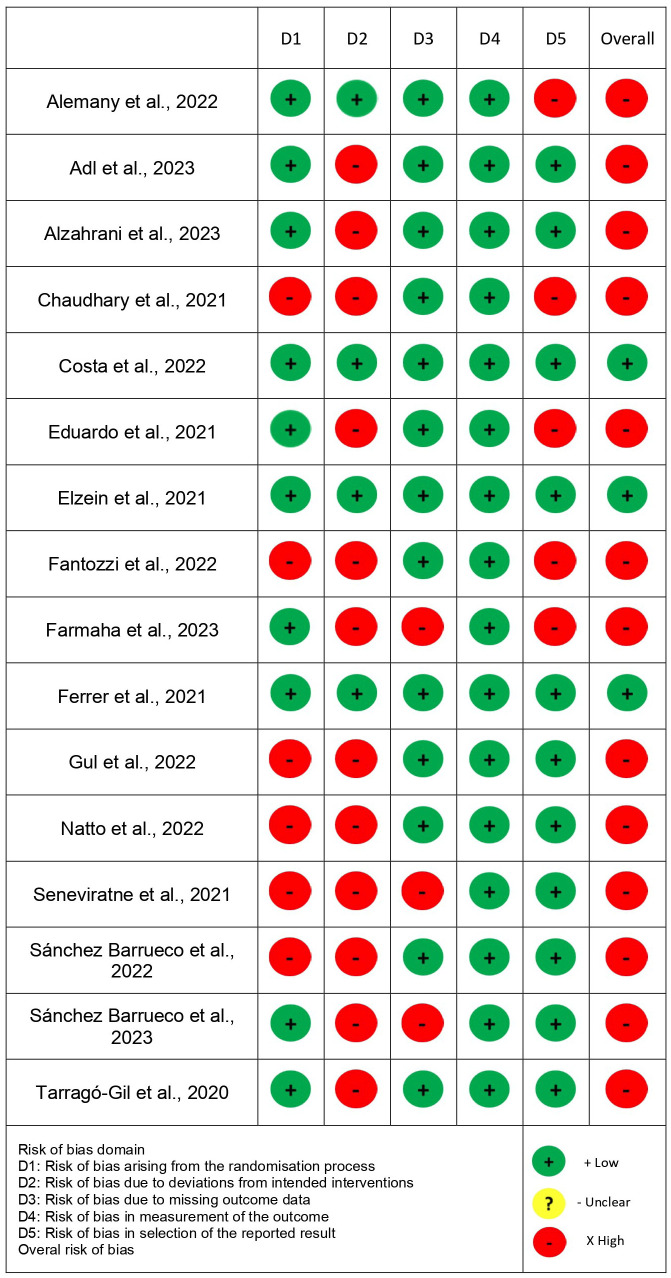 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsDental Research and COVID-19 · Scientific and Engineering Research Topics · COVID-19 diagnosis using AI
Introduction
COVID-19 has had a great impact on public health due to its rapid spread and the lack of effective measures to prevent infections or reduce their severity (1). It is caused by the Severe Acute Respiratory Syndrome Coronavirus type 2 (SARS-CoV-2) and is transmitted by the respiratory route through microdroplets or by direct contact with contaminated surfaces (2,3), causing atypical pneumonia with possible involvement of multiple organs and body systems (4).
The main source of SARS-CoV-2 transmission is symptomatic patients, whose viral load in saliva is highest in the first week after the onset of symptoms. However, asymptomatic and presymptomatic patients also have the capacity to be contagious (5,6). Likewise, the viral load in saliva is associated with the severity of COVID-19 and is considered a predictor of death, and it is of even greater importance than the patient’s age (7). This is because the main cellular receptor of the virus is angiotensin-converting enzyme 2 (ACE2), which has a high level of expression in the oral mucosa, particularly in the epithelium of the tongue and salivary glands (8-11). In this sense, the viral load attains a number of up to 1.2x 108 copies/mL and is present in 91.7% of saliva samples from individuals diagnosed with COVID-19 (12,13).
As saliva is the main infection route, oral antiseptics could be very useful to reduce the burden of SARS-CoV-2 and reduce transmission between individuals (2,4,9,11). Moreover, there have been reports indicating that by reducing the viral load in saliva by means of using mouthwashes containing CHX, CPC, and PVP-I, the severity of the disease would be reduced in terms of hospitalization time, admission to intensive care, and death. (2,3,7,8). This could be useful for dentistry and medical specialties, in which procedures involve generating aerosols and working close to the patient. These professionals would be directly and constantly exposed to this infection (14,15), implying a risk to their health and community.
Because individual studies may not have sufficient statistical power to reach a reliable conclusion, and the majority of systematic reviews found included studies with heterogeneous designs; the present systematic review and meta-analysis was conducted as an update on the topic, with the aim of synthesizing the evidence on the effectiveness of CHX, CPC and PVP-I-based mouthwashes to reduce the load of SARS-CoV-2 in saliva of adult patients with a diagnosis of COVID-19.
Material and Methods
-Protocol and Registration
The present systematic review was registered at the Postgraduate School of the Universidad Privada Antenor Orrego and approved by the Permanent Research Committee (Resolution No. 0800-2022-D-EPG-UPAO). It was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-analyses checklist (PRISMA, 2020) (16).
-Focused Question
The research question was as follows: Do povidone-iodine, cetylpyridinium chloride, or chlorhexidine mouthwashes reduce the load of SARS-CoV-2 in the saliva of adults diagnosed with COVID-19? This was proposed according to the PICOD strategy for research (population/patients, intervention, comparison, results, and design). Where P = adult patients diagnosed with COVID-19, I = povidone-iodine, cetylpyridinium chloride or chlorhexidine mouthwashes, C = placebo or no intervention, R = SARS-CoV-2 load reduction in saliva, and D = randomized controlled clinical trials
-Eligibility criteria and process of selection
Randomized, controlled, parallel-arm clinical trials were included, using distilled/sterile/tap water, saline, or no treatment as a control group, which specified dosage, duration, or frequency of mouthwashes and who measured loads as in saliva in terms of copies/ml or cycle threshold (Ct) values, before and after the intervention using PCR. Studies in which another treatment was added to the use of mouthwash or had incomplete data were excluded.
-Search Strategy
The search was conducted in the PubMed/Medline, Web of Science, Scopus, Embase, and BVS databases in December 2022 and updated in June 2023, in addition to manual searches in the reference lists of all studies included and previously published reviews. The following search terms were used: (COVID-19 OR coronavirus OR SARS-CoV-2) AND (mouthwash* OR povidone-iodine OR PVP-I OR cetylpyridinium OR chlorhexidine) AND (“viral load” OR “viral burden” OR “virus titer”). This was adapted according to the syntax rules of each database (Table 1).
Data extraction, risk of bias, and certainty of evidence
The literature search results were uploaded to the Rayyan Systematic Reviews Application (17) and duplicate records were removed. Two researchers (R.E.C. and A.A.A.) independently selected the articles to be analyzed, first by title and abstract, then by full text. Any disagreement was discussed with the participation of a third researcher (M.C.H.). Data were then extracted independently into an Excel spreadsheet (Microsoft® Excel® for Office 365). Subsequently, the articles selected and the data extracted were reviewed and approved by a fourth expert researcher (J.C.A.). Moreover, the clinical trials included were analyzed using the Cochrane Collaboration’s RoB 2.0 tool to assess the risk of bias (18).
Disagreements were resolved with the collaboration of the third and fourth investigators. The quality of evidence of the studies included in the meta-analysis was assessed using the GRADE tool, using the GRADEpro GDT software (19).
-Summary of Results
All outcome measures that assessed the reduction of SARS-CoV-2 viral load in saliva were considered. The information required for each study was collected in preliminary summary Tables. If these data were not found in the article, an email was sent to the authors to request them. Results with sufficient data to calculate an estimate of the effect were used for meta-analysis.
Results
-Selection of Studies
As presented in the PRISMA 2020 flowchart (20) (Fig. 1), 618 records were retrieved. After the removal of duplicates and selection by title and abstract, 19 articles remained for full-text evaluation. Of these, 3 were excluded for the following reasons: they did not specify the number of patients evaluated per study arm, they did not mention the dose of a rinse used and they used a method other than PCR to measure viral load and they used two of the mouthwashes in the same study arm. Finally, the qualitative analysis was carried out with 16 studies (Table 2), 6 of which were chosen for the meta-analysis.
Figure 1PRISMA 2020 flow diagram showing the entire search process.
-Characteristics of the Studies
In the 16 studies, a total of 919 subjects were evaluated. Those with the smallest number of participants evaluated 16 patients (3,21), and the study with the highest number evaluated 120 (10). The concentrations used for PVP-I were 0.25%, 0.5%, 1%, and 2%; for CPC, they were 0.07% and 0.075%. and for CHX, 0.12% and 0.2%. Three studies (3,5,22) compared PVP-I, CPC, and CHX; seven (8,21,23-27) compared at least two of them; and six (10,28-32) only one of them with the use of other study groups or placebo. All of them measured the viral load in saliva before and after the intervention at variable time intervals, the minimum time being immediately after rinsing and the maximum time interval after 6 hours.
The studies analyzed were conducted in Spain (5,22,28,31,32), Brazil (24,29), United States (21,23), Saudi Arabia (26,27), Italy (25), Singapore (3), Turkey (30), Lebanon (8) and Iran (10). The ages of the subjects studied ranged between 20 and 83 years old. Seven of the studies (3,5,10,22,25,26,32) did not mention adverse drug reactions. With respect to possible conflicts of interest, two (28,31) declared financing by DENTAID SL., one (24) by Colgate-Palmolive Company and another (23) did not submit the declaration. Seven of the studies (5,8,10,22,24,25,30) were conducted with hospitalized patients, and the other nine (3,21,23,26-29,31,32) were conducted with outpatients.
-Meta-analysis of the synthesis
The results of the meta-analysis are presented in the forest plot of Fig. 2, in which the standardized mean difference (SMD) is observed as a measure of the effect. Overall, a mean of 0.51 SMD (95% CI: -0.29; 1.32), which reflects the standardized effect size for all studies (I² = 46.0%; p = 0.047).
Figure 2. Forest plot of mouthwashes effects in reducing the viral load of SARS-CoV-2 in saliva. (Legend: *CPC = cetylpyridinium chloride, CHX = chlorhexidine, PVP-I = povidone-iodine.).
The studies included that evaluated CPC and CHX offered mixed results. For CPC, Alemany et al. (28) found an effect of 0.45 when they measured at one hour and 0.06 at three hours, while Tarragó-Gil et al. (31) reported an effect of -0.25 for a measurement after two hours. The subgroup analysis for CPC showed a non-significant medium combined effect (-0.07); likewise, the variability of the studies was not significant (I² = 0.0%; p = 0.373) with low certainty of evidence. With respect to CHX, Natto et al. (26) observed effects of 0.31 and 0.15 for specific genetic variants, while Costa et al. (29) reported effects of 0.61 and 0.46 for different measurement time intervals. The CHX subgroup had a non-significant mean combined effect (0.50), with non-significant perfect homogeneity (I² = 0.0%; p = 1.000) and very low certainty of evidence.
For the PVP-I-based mouthwashes, the results were more homogeneous. Elzein et al. (8) showed an effect of 4.30, while Gül et al. (30) reported a more modest effect (0.27). The studies of Natto et al. (26) also supported the effectiveness of PVP-I with effect sizes of 0.90 and 0.36. The subgroup analysis for PVP-I concluded with a significant mean combined effect in viral load reduction (4.15), with very low heterogeneity between studies, statistically non-significant (I² = 0.0%; p = 0.908), and low certainty of evidence.
Egger’s regression indicated the absence of publication bias (p=0.56). It is worth mentioning that the meta-analysis initially included seven studies. However, after performing the sensitivity analysis to evaluate the robustness of the results, the researchers found that the study by Fantozzi et al. (25) reported their values in medians and interquartile ranges, unlike the rest of the studies selected, which reported them in means and standard deviations. Since it significantly altered the overall results, it was excluded from the main combined analysis. This exclusion led to greater consistency in the results. Despite this exclusion, the variability of reporting methods was considered an important factor in the qualitative interpretation of the results.
Risk of bias and quality of evidence
The RoB 2.0 tool was used for risk of bias assessment (Fig. 3). Three studies presented low risk (5,8,29), and the others presented high risk of bias. The quality of the evidence of the studies included in the meta-analysis, according to GRADE, is presented in Table 3.
Figure 3. Summary of the risk of bias assessment – Cochrane tool (RoB 2.0).
Discussion
COVID-19 continues to be a threat that requires the development of effective and cost-effective intervention measures to prevent cross-contamination and community transmission (33). This systematic review with meta-analysis aimed to evaluate the effectiveness of three mouthwashes in reducing the viral load of SARS-CoV2 in the saliva of adult patients diagnosed with COVID-19.
In the clinical trials analyzed, CHX was the substance most frequently studied, followed by PVP-I and CPC. Ferrer et al. (5), Sánchez et al. (22), and Seneviratne et al. (3) included all three mouthwashes in their studies. The first two found no differences when compared with the controls; while Seneviratne et al (3) observed a significant decrease in viral load between groups, at 5 minutes for CPC and at 6 hours for CPC and PVP-I, compared with the control. It is worth mentioning that they only worked with 2 subjects as a control group. The three studies had a small sample size and no statistical basis. Attention is drawn to the fact that in the two studies in which the mouthwashes did not affect the viral load (5,22), the concentration of PVP-I was much higher (PVP-I 2%) than in the study where an effect was obtained (PVP -I 0.5%) (3). In the latter, the rinsing time was even shorter. Only the study of Ferrer et al. (5) showed a low risk of bias, while the other two studies had a high risk of bias. Therefore, it could not yet be concluded that there was real effectiveness; in agreement with the systematic review by Hernández-Vásquez et al. (1) but disagreeing with the reviews by Mezarina et al. (2), García-Sánchez et al. (4) and Ziaeefar et al. (34), possibly because they evaluated a smaller number of studies and with methodological deficiencies as they were the first clinical trials. In contrast, Ting et al. (35), despite declaring the effectiveness of these mouthwashes, mentioned the importance of distinguishing whether they were better than water and saline solution. These statements were contradictory.
Farmaha et al. (21), Elzein et al. (8), Chaudhary et al. (23), Natto et al. (26), and Fantozzi et al. (25), only compared two of the mouthwashes of our interest, CHX and PVP-I. Farmaha et al. (21) and Elzein et al. (8) found the effectiveness of both mouthwashes compared with the control immediately after and after 5 minutes, respectively. Furthermore, for Farmaha et al. (21), CHX maintained its effect for up to 2 hours. However, Chaudhary et al. (23), Natto et al. (26) and Fantozzi et al. (25), concluded that none of the mouthwashes demonstrated effectiveness. All the studies mentioned had a very limited number of subjects per study group, which would affect the internal validity of the clinical trials. Moreover, their results have been reported confusingly, with the exception of the study of Elzein et al. (8), which showed a low risk of bias. These findings were consistent with the systematic reviews and meta-analyses of Zhang et al. (36) and Hasan et al. (37), who concluded that both PVP-I and CHX were effective, mainly within the first 30 minutes after rinsing, and that PVP-I was better.
Eduardo et al. (24) evaluated CPC and CHX and reported that both reduced the viral load immediately afterward, at 30 min, and up to 1 hour later. However, it is important to assess the conflict of interest reported by the authors. In contrast, Ebrahimi et al. (38), in their systematic review and meta-analysis, indicated that there was insufficient evidence about the effects of CPC and CHX on the reduction of SARS-CoV-2 viral load. Alzahrani et al. (27) evaluated PVP-I and CPC and found differences between the groups and the control with distilled water versus the control without rinsing at 60 minutes, which would imply a mechanical washing effect but not an antiviral effect. The aforementioned studies showed a high risk of bias.
Among the studies that evaluated at least one of the mouthwashes required for this review, Tarragó-Gil et al. (31) and Alemany et al. (28) found no differences between the CPC and control groups. It is important to emphasize that the sample size for these studies was larger than forty patients per group, which would mean an improvement in statistical power compared with most studies analyzed. In this regard, Sbricoli et al. (39), in their systematic review and meta-analysis, observed inconsistent results regarding the reduction of viral load in saliva induced by this active ingredient, while D’Amico et al. (7), in their systematic review, indicated that CPC was effective.
Costa et al. (29) and Sánchez et al. (32) reported that CHX was effective in decreasing the viral load in saliva for at least 1 hour. Moreover, Sánchez et al. (32), when comparing two concentrations of CHX, 0.12% and 0.2%, unexpectedly found the lower concentration to be more effective, indicating that the ingredients that accompany the active principle could have some effect on the results. These two studies showed a small number of participants, and only that of Costa et al. (29) showed a low risk of bias. Therefore, studies with better methodological design are required. These findings contradict the systematic review by Sbricoli et al. (39), who indicated that CHX at 0.2% was associated with a reduction in viral load, agreeing with Fernández et al. (40) and Rahman et al. (14), who also mentioned that the effect lasted for a short period, and Ting et al. (35), who reported a maximum reduction after 60 minutes.
The studies of Gül et al. (30) and Adl et al. (10), found that PVP-I was not effective in reducing the viral load. The risk of bias for both was high; for this reason, it is also recommended that studies with better methodology and larger sample sizes be conducted. Conversely, Ebrahimi et al. (38), in their systematic review, recommended the use of PVP-I mouthwashes to reduce the viral load of SARS-COV-2 in the oral cavity of patients before and during dental procedures.
Some of the clinical trials analyzed in this systematic review’s results were contradictory. Chaudhary et al. (23), Fantozzi et al. (25), and Ferrer et al. (5) observed significant reductions in viral loads in their control groups; while in the study by Alzaharani et al. (27), a reduction was observed in the control group compared with the group without rinsing. These results suggested a possible mechanical washing effect of viral particles due to the rinsing process.
The meta-analysis showed a significant combined effect only for PVP-I, (8,26,30) while for CPC (28,31) and CHX (26,29), the effects were not significant. However, taking into consideration the level of certainty of the evidence according to GRADE, these results would indicate that confidence in the effect estimate was limited or unreliable; that is, the true effect could differ substantially from the estimated effect. Moreover, it is important to mention the variability in the allocation times of the mouthwashes; for PVP-I, the measurement was immediately and 5 minutes after the rinse, and for CPC and CHX, the measurements were recorded between 1 and 3 hours after the rinse.
Within the limitations of this review, it should be considered that the majority of clinical trials conducted to date showed inadequate sample sizes, high risk of bias, variable intervention times, and even some studies with a possible conflict of interest, making it difficult to perform a more robust meta-analysis. However, randomization for the distribution of treatments and control groups could be considered a strength of the analyzed studies. In general, the recommendation to conduct clinical trials with a better methodological design and a larger number of patients is reiterated. As an additional point, the studies included only evaluated the presence of viral particles but not their viability or capacity for being infectious.
The present systematic review and meta-analysis concluded that when evaluating all mouthwashes simultaneously, no significant effect was found. However, when evaluated separately, only PVP-I effectively reduced the SARS-CoV-2 load in saliva. The results should be considered with great caution due to the high risk of bias shown in the clinical trials analyzed and the low level of certainty of the evidence.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Hernández-Vásquez A Barrenechea-Pulache A ComandéD Azañedo D Mouthrinses and SARS-Co V-2 viral load in saliva: a living systematic review Evid Based Dent 202224173561047910.1038/s 41432-022-0253-z PMC 9128317 · doi ↗ · pubmed ↗
- 2Mezarina Mendoza JPI Trelles Ubillús BP Salcedo Bolívar GT Castañeda Palacios RDP Herrera Lopez PSG Padilla Rodríguez DA Antiviral effect of mouthwashes against SARS-COV-2: A systematic review Saudi Dent J 202234(3)167933512583510.1016/j.sdentj.2022.01.006PMC 8806023 · doi ↗ · pubmed ↗
- 3Seneviratne CJ Balan P Ko KKK Udawatte NS Lai D Ng DHL Efficacy of commercial mouth-rinses on SARS-Co V-2 viral load in saliva: randomized control trial in Singapore Infection 202149(2)305113331518110.1007/s 15010-020-01563-9PMC 7734110 · doi ↗ · pubmed ↗
- 4García-Sánchez A Peña-Cardelles JF Ruiz S Robles F Ordonez-Fernandez E Salgado-Peralvo AO Efficacy of Pre-Procedural Mouthwashes against SARS-Co V-2: A Systematic Review of Randomized Controlled Trials J Clin Med 202211(6)16923533001610.3390/jcm 11061692 PMC 8955331 · doi ↗ · pubmed ↗
- 5Ferrer MD BarruecoÁS Martinez-Beneyto Y Mateos-Moreno MV Ausina-Márquez V García-Vázquez E Clinical evaluation of antiseptic mouth rinses to reduce salivary load of SARS-Co V-2Sci Rep 202111(1)243923493785510.1038/s 41598-021-03461-y PMC 8695582 · doi ↗ · pubmed ↗
- 6Tadakamadla J Boccalari E Rathore V Dolci C Tartaglia GM Tadakamadla SK In vitro studies evaluating the efficacy of mouth rinses on Sars-Cov-2: A systematic review J Infect Public Health 202114(9)1179853439918910.1016/j.jiph.2021.07.020PMC 8339500 · doi ↗ · pubmed ↗
- 7D'Amico F Moro M Saracino M Marmiere M Cilona MB Lloyd-Jones G Efficacy of Cetylpyridinium Chloride mouthwash against SARS-Co V-2: A systematic review of randomized controlled trials Mol Oral Microbiol 202338(3)171803680888910.1111/omi.12408 · doi ↗ · pubmed ↗
- 8Elzein R Abdel-Sater F Fakhreddine S Hanna PA Feghali R Hamad H In vivo evaluation of the virucidal efficacy of chlorhexidine and povidone-iodine mouthwashes against salivary SARS-Co V-2. A randomized-controlled clinical trial J Evid Based Dent Pract 202121(3)1015843447966810.1016/j.jebdp.2021.101584 PMC 8080510 · doi ↗ · pubmed ↗