Experiences of attending prenatal ultrasounds during the COVID‐19 pandemic in Australia: A cross‐sectional survey
Helen J. Nightingale, Christina Watts, Kim Pham

TL;DR
This study explores how pandemic restrictions affected pregnant women's experiences during prenatal ultrasounds in Australia, finding high levels of distress and trauma.
Contribution
The study provides new insights into the psychological impact of pandemic-related changes on prenatal ultrasound experiences.
Findings
Almost 37% of respondents showed probable post-traumatic stress disorder symptoms.
Unexpected ultrasound findings and prior trauma correlated with lower satisfaction and higher expectations.
Pregnancy loss and fetal abnormalities were strongest factors linked to trauma symptoms.
Abstract
Prenatal ultrasounds form an important part of routine maternity care in Australia and indeed internationally. The COVID‐19 pandemic necessitated rapid changes in society and healthcare to curb transmission, with evidence demonstrating detrimental impacts on childbearing women associated with these restrictions. However, experiences with pandemic restrictions for prenatal ultrasounds in relation to distress, patient expectations, and satisfaction are largely unknown. This study aimed to explore the experiences of pregnant women attending prenatal ultrasound during the pandemic in Australia. A cross‐sectional online survey of people in Australia who had undergone at least one prenatal ultrasound during the period of maternity care restrictions was performed. The survey included validated tools for assessing post‐traumatic stress, satisfaction, and expectations with maternity care. A…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
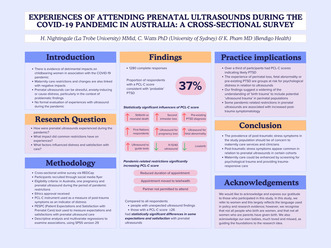 Figure 1
Figure 1|
| |
|---|---|
| Age ( | |
| 18–30 years | 387 (30.1) |
| 31–40 years | 877 (68.1) |
| 41–45 years | 22 (1.7%) |
| Older than 45 | 1 (0.1%) |
| Sex ( | |
| Female | 1271 (99.3) |
| Other | 1 (0.1) |
| Declined to respond | 7 (0.5%) |
| Region of birth ( | |
| Oceania | 995 (87.2) |
| Asia | 48 (4.2) |
| Africa | 15 (1.3) |
| Caribbean | 2 (0.2) |
| Europe | 59 (5.2) |
| North America | 17 (1.5) |
| South America | 4 (0.4) |
| Ethnicity (participants could select multiple options) ( | |
| White European | 1104 (88.6) |
| Indigenous/First Nations | 21 (2.6) |
| Black African | 1 (0.1) |
| Hispanic | 8 (0.6) |
| Northern African | 2 (0.2) |
| Middle Eastern | 10 (0.8) |
| South Asian | 6 (0.5) |
| South East Asian | 24 (1.9) |
| East Asian | 6 (0.5) |
| Māori | 8 (0.6) |
| Pacific Islander | 3 (0.2) |
| Mixed Race | 39 (3.1) |
| Other | 72 (5.8) |
| State/Territory ( | |
| Australian Capital Territory | 15 (1.2) |
| New South Wales | 343 (26.9) |
| Northern Territory | 9 (0.7) |
| Queensland | 140 (11.0) |
| South Australia | 50 (3.9) |
| Tasmania | 23 (1.8) |
| Victoria | 626 (49.0) |
| Western Australia | 71 (5.6) |
| Highest level of education ( | |
| Year 10 or equivalent | 8 (0.6) |
| Higher school certificate/Year 12 or equivalent | 84 (6.5) |
| Trade/apprenticeship | 14 (1.1) |
| Certificate/diploma | 218 (16.9) |
| Bachelor degree | 525 (40.8) |
| Postgraduate degree/Master's degree or higher | 231 (17.9) |
| Main occupation ( | |
| Professional | 717 (56.0) |
| Self‐employed | 68 (5.3) |
| Stay‐at‐home parent | 219 (17.1) |
| Manager/administrator | 152 (11.9) |
| Tradesperson | 9 (0.7) |
| Sales or Service worker | 42 (3.3) |
| Laborer | 2 (0.2) |
| Other | 71 (5.5) |
| Employment status ( | |
| Full‐time | 334 (26.0) |
| Part‐time | 579 (45.1) |
| Contract/temporary/casual | 64 (5.0) |
| Unemployed | 5 (0.4) |
| Unable to work | 4 (0.3) |
| Stay‐at‐home parent | 266 (20.7) |
| Other | 29 (2.3) |
| Declined to respond | 2 (0.2) |
| Relationship status ( | |
| Single | 6 (0.5) |
| Married/de facto | 1246 (96.7) |
| In a relationship | 31 (2.4) |
| Separated/divorced | 4 (0.3) |
| Other | 1 (0.1) |
| Annual household income, approximate ($AUD) ( | |
| 0–less than 40,000 | 14 (1.1) |
| 40,000–less than 75,000 | 66 (5.1) |
| 75,000–less than $130,000 | 451 (35.0) |
| 130,000 or more | 710 (55.2) |
| Declined to respond | 46 (3.6) |
| Disability status ( | |
| Considered or diagnosed as having a disability | 25 (2.0) |
| No disability | 1245 (98.0) |
| Declined to respond | 1 (0.1) |
|
| |
|---|---|
| Number of pregnancies, total ( | |
| 1 | 419 (33.5) |
| 2 | 421 (33.6) |
| 3 | 241 (19.2) |
| 4 | 104 (8.3) |
| 5 or more | 66 (5.3) |
| Number of pregnancies during pandemic restrictions period (March 2020 to end of 2022) ( | |
| 1 | 732 (58.6) |
| 2 | 398 (31.9) |
| 3 | 96 (7.7) |
| 4 | 14 (1.1) |
| 5 or more | 9 (0.7) |
| Number of babies birthed, total (including babies born after 20 weeks of pregnancy, and any babies not still living) | |
| 0 | 62 (5.0) |
| 1 | 650 (51.9) |
| 2 | 414 (33.1) |
| 3 | 101 (8.1) |
| 4 | 19 (1.5) |
| 5 or more | 6 (0.5) |
| Use of assisted reproduction technology ( | |
| Yes | 171 (13.7) |
| No | 1076 (86.2) |
| Declined to respond | 1 (0.1) |
| Current or prior mental health diagnosis ( | |
| Anxiety | 510 (40.0) |
| Depression | 312 (24.5) |
| Bipolar disorder | 9 (0.7) |
| Post‐traumatic stress disorder | 90 (7.1) |
| Other | 42 (3.3) |
| None of the above | 691 (54.2) |
| Planned place of birth for pregnancy/s during the time of pandemic restrictions ( | |
| Home | 73 (5.8) |
| Public hospital | 800 (63.9) |
| Private hospital | 306 (24.5) |
| Birth center | 39 (3.1) |
| I had more than one pregnancy at this time and different planned places for birth | 24 (1.9) |
| Unsure | 9 (0.7) |
| Lead carer for pregnancy/s during the time of pandemic restrictions ( | |
| Private midwife | 91 (7.3) |
| Private obstetrician | 343 (27.4) |
| Midwifery group/caseload practice | 284 (22.7) |
| Team midwifery | 85 (6.8) |
| Public hospital—clinicians on shift | 237 (18.9) |
| GP/obstetrician shared care | 152 (12.1) |
| I had more than one pregnancy at this time and different lead care providers | 50 (4.0) |
| Unsure | 10 (0.8) |
| Pregnancy outcome/s experienced during the time of pandemic restrictions (multiple outcomes able to be selected) ( | |
| Live birth | 1136 (90.8) |
| First‐trimester miscarriage | 246 (19.7) |
| Second‐trimester miscarriage | 17 (1.4) |
| Ectopic pregnancy | 11 (0.9) |
| Termination of pregnancy | 31 (2.5) |
| Stillbirth or neonatal death | 28 (2.2) |
| Premature birth | 61 (4.9) |
| Currently pregnant at the time of participating | 185 (14.8) |
| PCL‐C measures ( | |
| PCL‐C score M (SD) | 27.5 (14.7) |
| PCL‐C ≥ 26 n (%) | 384 (36.8) |
| PCL‐C 25th percentile score | 17 |
| PCL‐C 75th percentile score | 32 |
| PESPC | Mean, | Low expectation or satisfaction % | Moderate expectation or satisfaction % | High expectation or satisfaction % |
|---|---|---|---|---|
| I expected to have my ultrasound visit/s take a long time | ||||
| All | 2.94 | 28.8 | 41.4 | 29.7 |
| Those with unexpected US findings | 2.94, | 29.7 | 39.0 | 31.3 |
| Those with PCL score ≥ 26 | 3.08, | 23.8 | 44.4 | 31.9 |
| I expected to see the same provider in the case of needing more than one ultrasound | ||||
| All | 2.28 | 60.1 | 14.1 | 25.8 |
| Those with unexpected US findings | 2.34, | 59.1 | 12.7 | 28.2 |
| Those with PCL score ≥ 26 |
| 43.8 | 16.9 | 39.4 |
| I expected the provider to care how I felt mentally as well as physically | ||||
| All | 3.84 | 14.9 | 17.3 | 67.9 |
| Those with unexpected US findings |
| 11.6 | 15.8 | 72.6 |
| Those with PCL score ≥ 26 |
| 9.3 | 11.2 | 79.5 |
| I expected the provider to be gentle during the examination | ||||
| All | 4.43 | 3.2 | 5.7 | 91.1 |
| Those with unexpected US findings | 4.48, | 2.3 | 8.3 | 91.7 |
| Those with PCL score ≥ 26 | 4.48, | 3.7 | 5.0 | 91.3 |
| I expected to have my problems listened to | ||||
| All | 4.00 | 10.8 | 15.5 | 73.7 |
| Those with unexpected US findings | 4.05, | 10.2 | 14.3 | 75.4 |
| Those with PCL score ≥ 26 | 4.14, | 9.9 | 11.2 | 78.9 |
| I am satisfied with the explanation the provider gave to me of what was going to happen | ||||
| All | 3.74 | 14.9 | 20.7 | 64.4 |
| Those with unexpected US findings |
| 21.4 | 21.4 | 57.1 |
| Those with PCL‐score ≥ 26 |
| 30.0 | 24.4 | 45.6 |
| I am satisfied with the explanation the provider gave to me about how things were going following the ultrasound/s | ||||
| All | 3.66 | 16.4 | 22.6 | 61.1 |
| Those with unexpected US findings |
| 23.4 | 23.8 | 52.8 |
| Those with PCL score ≥ 26 |
| 19.3 | 24.2 | 46.6 |
| I am satisfied with the way I was treated | ||||
| All | 3.74 | 15.3 | 18.1 | 66.6 |
| Those with unexpected US findings |
| 20.3 | 23.8 | 57.3 |
| Those with PCL score ≥ 26 |
| 35.4 | 18.6 | 46.0 |
| I am satisfied with the quality of care I received | ||||
| All | 3.77 | 14.1 | 18.3 | 67.6 |
| Those with unexpected US findings |
| 18.5 | 22.7 | 58.8 |
| Those with PCL score ≥ 26 |
| 35.0 | 21.3 | 43.8 |
| I am satisfied with not having to repeat my story every time I had an ultrasound | ||||
| All | 2.96 | 39.9 | 21.3 | 38.8 |
| Those with unexpected US findings |
| 51.9 | 19.3 | 28.8 |
| Those with PCL score ≥ 26 |
| 63.4 | 19.9 | 16.8 |
| I am satisfied with being able to ask questions without embarrassment | ||||
| All | 3.76 | 13.6 | 21.3 | 65.1 |
| Those with unexpected US findings |
| 17.9 | 22.9 | 59.3 |
| Those with PCL score ≥ 26 |
| 22.4 | 29.8 | 47.9 |
| I am satisfied with the way the staff expressed concern about my personal situation | ||||
| All | 3.44 | 20.3 | 27.2 | 52.5 |
| Those with unexpected US findings |
| 26.7 | 26.5 | 46.9 |
| Those with PCL score ≥ 26 |
| 36.9 | 26.9 | 36.3 |
| I am satisfied with the way my medical/obstetric complications were managed | ||||
| All | 3.59 | 18.2 | 22.2 | 59.6 |
| Those with unexpected US findings |
| 27.2 | 20.6 | 52.1 |
| Those with PCL score ≥ 26 |
| 35.4 | 17.4 | 47.2 |
| I am satisfied with the amount of time I waited to be seen for my ultrasound/s | ||||
| All | 3.53 | 18.2 | 24.3 | 57.5 |
| Those with unexpected US findings |
| 23.1 | 25.6 | 51.3 |
| Those with PCL score ≥ 26 |
| 30.0 | 23.1 | 46.9 |
| I am satisfied with the total amount of time I spent at the health service in relation to the ultrasound | ||||
| All | 3.64 | 14.1 | 24.8 | 61.2 |
| Those with unexpected US findings | 3.49, | 17.9 | 28.0 | 54.1 |
| Those with PCL score ≥ 26 |
| 24.5 | 30.2 | 45.2 |
| I am satisfied with the examination room of the ultrasound/s | ||||
| All | 3.98 | 8.1 | 15.7 | 76.2 |
| Those with unexpected US findings |
| 10.3 | 18.2 | 71.6 |
| Those with PCL score ≥ 26 |
| 19.0 | 15.8 | 65.2 |
| I am satisfied with my ability to schedule ultrasound visits at a time convenient for me | ||||
| All | 3.22 | 30.8 | 22.0 | 47.1 |
| Those with unexpected US findings |
| 36.4 | 22.8 | 40.8 |
| Those with PCL score ≥ 26 |
| 44.4 | 17.5 | 38.1 |
| I am satisfied with how easy it was to reschedule my ultrasound visits | ||||
| All | 3.07 | 34.9 | 23.8 | 41.4 |
| Those with unexpected US findings |
| 41.1 | 22.9 | 36.0 |
| Those with PCL score ≥ 26 |
| 51.3 | 17.9 | 30.8 |
| I am satisfied with the number of ultrasounds I had | ||||
| All | 3.77 | 14.6 | 18.6 | 66.8 |
| Those with unexpected US findings |
| 19.4 | 19.6 | 61.0 |
| Those with PCL score ≥ 26 |
| 26.1 | 24.2 | 49.6 |
| Factor | Unstandardized B | Standardized coefficients beta | t | p |
|---|---|---|---|---|
| Stillbirth/neonatal death | 21.366 | 0.214 | 6.663 |
|
| Second‐trimester pregnancy loss | 10.765 | 0.085 | 3.008 |
|
| PTSD diagnosis | 8.466 | 0.148 | 5.024 |
|
| First Nations | 7.161 | 0.060 | 2.123 |
|
| Ultrasound for pregnancy loss | ||||
| Ultrasound for fetal abnormality | 3.863 | 0.151 | 3.287 |
|
| Ultrasound to guide for other tests | 4.387 | 0.064 | 2.183 |
|
| Live birth | −6.104 | −0.120 | −3.222 |
|
| First‐trimester ultrasound 11–14 weeks | −3.421 | −0.076 | −2.497 |
|
| Partner not permitted to attend | 2.418 | 0.075 | 2.518 |
|
| Ultrasound appointment reduced duration | 3.957 | 0.101 | 3.512 |
|
| Ultrasound appointment moved to telehealth | 2.580 | 0.058 | 2.083 |
|
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMaternal and Perinatal Health Interventions · Maternal Mental Health During Pregnancy and Postpartum · Maternal and fetal healthcare
INTRODUCTION
1
Ultrasound examinations form part of routine maternity care, and Australian practice guidelines provide guidance on timing of ultrasound examinations in pregnancy. Prenatal ultrasounds provide an important opportunity to accurately date the pregnancy, confirm normal development, or conversely, identify possible problems and enable further care1; they also offer a chance for the woman and partner to connect with their developing baby, contributing to a positive pregnancy experience, providing reassurance, strengthening their relationship, and assisting the transition to parenthood.2, 3
Unexpected, concerning, or uncertain findings during a scan (such as twin pregnancy, fetal abnormality, or placental abnormality) can prompt feelings of shock, anxiety, or stress, result in reduced attachment to the baby, and may create distress in relation to subsequent ultrasound examinations, even if the findings are normal.4, 5 Rates of psychological distress or trauma are already acknowledged to be high in perinatal settings. This is increased in high‐risk cohorts, such as those experiencing complex pregnancies, perinatal loss, fetal anomaly, or complications such as hyperemesis gravidarum, where post‐traumatic stress disorder (PTSD) prevalence can be as high as 40%.6
Patient perspectives in healthcare are an important measure of quality of care received, and a conduit to service improvement.7 Fulfillment of expectations in maternity care is a consistent predictor of satisfaction with care, and both expectations and satisfaction with care are factors that provide a reflection of quality of care received.8, 9 Negative experiences, subjective distress, low support, and obstetric factors such as pregnancy complications increase the likelihood of subsequent mental health disorders, as well as perception of a traumatic event, post‐traumatic stress symptoms, and PTSD.10, 11, 12 The presence of these factors can have significant consequences for women and families, such as reduced parenting satisfaction, increased parenting stress, problematic attachment and bonding with the baby, infant development, family planning, and even reduced fertility.13, 14
During the COVID‐19 pandemic in Australia, rapid responses were implemented by governments and health services to suppress transmission of the virus.15 Maternity services were also impacted: masks became mandated; antenatal consults were reduced in frequency, duration, or moved to telehealth; birth education classes were ceased or moved to an online format; and there were limitations on in‐person supports for appointments—often preventing the partner or non‐pregnant parent from attending.16
Internationally, a wealth of evidence has examined experiences of maternity care during this time. The pandemic exacerbated feelings of psychological distress and mood disorders that are common in pregnancy,16, 17, 18 and a meta‐analysis highlighted rates of psychological distress around 70% in pregnant women during the COVID‐19 pandemic.19 In Australia and globally, maternity care restrictions intensified stress, anxiety, and distress for pregnant people17, 20 and some groups, such as people experiencing loss or pregnancy after loss, may have been disproportionately impacted by the restrictions.21 Partners of pregnant people felt isolated, distressed, and less connected to their babies as a result of the restrictions on their participation in maternity care.22
Existing evidence has determined that disallowing support people at prenatal ultrasounds had a negative impact on parental experiences and was distressing,23 and separation of the parents at a miscarriage diagnosis carried an associated emotional cost.18 However, formal evaluation of the impact of pandemic restrictions for prenatal ultrasounds on trauma and post‐traumatic stress symptoms and expectations and satisfaction with care is lacking.
This study aims to describe and understand the experience of pregnant women and people attending prenatal ultrasound during the COVID‐19 pandemic and examine the variables that influence participants' satisfaction with care and distress levels in association with their experiences.
METHODS
2
Procedure
2.1
A cross‐sectional online survey was administered through a secure platform (REDCap) with recruitment commencing in December 2022 and concluding in February 2023. An advertising flyer was created with a direct link to the open, online survey. This flyer was then distributed by means of social media and the researchers' networks. The flyer could be shared and thus snowball sampling was an additional recruitment strategy. All participants provided online informed consent before accessing the survey. Question order was not randomized. Only people who were in Australia, had experienced at least one pregnancy, and at least one ultrasound for pregnancy, during the period of pandemic restrictions (for the purpose of the study, considered from March 2020 to September 2022, when restrictions were still commonly in place in Australia), were eligible to participate. The strengthening the reporting of observational studies (STROBE) in Epidemiology guidelines for reporting on cross‐sectional studies and the Checklist for Reporting Results of Internet E‐Surveys (CHERRIES) were used to report the findings of this study.24
Ethical considerations
2.2
The study received approval from [redacted in line with journal requirements]. Participation was anonymous and participants were advised that they could stop participating at any point by simply exiting their browser. The survey preamble informed participants about expected time commitment for completing the survey, and the research team gave details about data storage and confidentiality. It acknowledged that the recall of their experiences may be distressing and contact details for the research team as well as a multitude of support and counseling services were provided. Participants were not offered incentives to participate.
Measures
2.3
Biographical data were collected by means of sociodemographic questions and questions about medical, psychological, and obstetric history. We evaluated the prevalence of post‐trauma symptoms as an indicator of distress experienced in relation to prenatal ultrasounds during the period of the pandemic by administering the PCL‐C instrument, which consists of 17 questions corresponding to the DSM‐5 (Diagnostic and Statistical Manual of Mental Disorders, 5th edition) symptom criteria for PTSD.10, 25 Participants respond with a Likert‐type scale (1 = not at all, 5 = extremely) to evaluate the level of distress experienced for each item in relation to their experience with prenatal ultrasounds during the period of the pandemic in Australia. A self‐administered PCL‐C questionnaire is validated for screening for PTSD,10 including in pregnant populations.26 The PCL‐C total score ranges from 17 to 85, and a score of ≥26 is considered indicative of PTSD in pregnant populations.26 In the present study, the PCL‐C demonstrated excellent internal consistency with a Cronbach's alpha of 0.96.
Additionally, we evaluated satisfaction and expectations in relation to prenatal ultrasound by means of 19 questions drawn from the Patient Expectations and Satisfaction with Prenatal Care (PESPC) tool, a validated instrument for measuring satisfaction with prenatal care.27 The final survey consisted of 67 questions. Where possible, wording for questions was amended by the research team who have personal experiences with perinatal or baby loss to ensure questions were appropriate and sensitive. The survey was piloted with the target population to ensure sensitivity and clarity of the wording of questions.
Analysis
2.4
Data were imported to IBM Statistical Package for Social Sciences (SPSS) version 29. Descriptive analysis was performed for demographic, medical, psychological, and obstetric data. Multivariate regressions were performed to examine associations between a high PCL‐C score and independent variables. All significance levels were set at p = 0.05.
RESULTS
3
Of a total of 1416 entries, 1280 participants progressed beyond initial demographic questions. Participant demographics are shown in Table 1. The majority were of white or European background, with more than half of respondents having a Bachelor's degree or higher.
Medical and obstetric characteristics
3.1
Participant medical and obstetric characteristics are presented in Table 2. Most participants experienced 1 or 2 pregnancies over the period of pandemic restrictions. Pre‐existing mental health conditions were common, with 40% of participants reporting a pre‐existing anxiety diagnosis, 25% reporting a pre‐existing depression diagnosis, and 7% identified an existing PTSD diagnosis. Most (64%) planned to birth in a public hospital, and 64% were engaged with a model of care affording at least some degree of continuity of care. The vast majority (91%) experienced a live birth during the period of pandemic restrictions, while almost 20% reported experiencing a first‐trimester miscarriage during this period. The mean PCL‐C score was 27.5, and almost 37% of respondents had a PCL‐C score of ≥26 indicating a high probability of PTSD.
Expectations and satisfaction with prenatal ultrasounds experience
3.2
Table 3 presents the mean response scores for the PESPC instrument. For the purposes of analysis, we classified responses of ‘not at all’ and ‘a little bit’ as low expectation or satisfaction, responses of ‘quite a bit’ or ‘extremely’ as high expectation or satisfaction, with a response of ‘moderately’ representing average expectation or satisfaction. Thus, a mean score of <2 indicates lower levels of expectation or satisfaction, a score between 2 and <4 indicates moderate expectation or satisfaction, and a score of ≥4 represents a higher level of expectation or satisfaction. Mean scores for those with unexpected ultrasound findings and those with a PCL score ≥26 were compared with the mean scores for all respondents, with a p value of <0.05 indicating statistically significant differences in scores (highlighted in bold).
In the expectations scale, the highest average score was obtained for ‘provider gentleness’ with 91% of all responses indicating high expectations for this question; the lowest average score related to the expectation of seeing the same provider in the setting of needing more than one ultrasound (60% of all respondents indicating low expectations for this). Subgroup analysis of responses demonstrated that those with a high PCL‐C score had statistically higher expectations for seeing the same provider.
In the satisfaction scale, the highest score was obtained for satisfaction with the ultrasound examination room (76% of all respondents had high satisfaction), although those with unexpected ultrasound findings or high PCL‐C scores had significantly lower satisfaction in this factor. The lowest satisfaction score was obtained for ‘not having to repeat my story every time I had an ultrasound’, with almost 40% of participants indicating low satisfaction with this factor. Satisfaction scores were significantly lower for those with unexpected ultrasound findings (52%) and/or those with a high PCL‐C score (63%).
PCL score and distress measures
3.3
A total of 361 (35%) participants completing the PCL‐C tool returned a score of ≥26, considered sufficient for a probable PTSD diagnosis.26
Multivariate analysis using standard multiple regression was used to determine the significance of association between a positive PCL‐C score (≥26) and independent variables (Table 4). Results demonstrate that the independent variables explain a significant amount of the variance in PCL‐C scores (R ^2^ = 0.426, adjusted R ^2^ = 0.375 p = <0.001). Stillbirth or neonatal death, second‐trimester pregnancy loss, and pre‐existing PTSD diagnosis were the strongest predictors for a positive PCL‐C score. First Nations status, ultrasound for pregnancy loss, fetal abnormality, or as a guide for other investigations also significantly correlated with increased PCL‐C scores. Live birth and having a first‐trimester ultrasound between 11 and 14 weeks were the only significant protective factors correlating with a decrease in PCL‐C score. Of the pandemic restrictions for prenatal ultrasounds, prohibition of partner attendance, reduced appointment duration, and appointments moved to telehealth were all significantly correlated with an increase in PCL‐C score. Collinearity diagnostics suggested only weak correlations between independent variables; multicollinearity diagnostics were within acceptable limits.
DISCUSSION
4
To our knowledge, this is the first study to specifically examine pregnant women's and people's experiences of prenatal ultrasound during the pandemic in relation to expectations, satisfaction, and distress. These findings add to existing evidence that many pandemic‐responsive maternity care restrictions, such as reduced frequency or duration of ultrasounds and the exclusion of support person attendance, were correlated with increased distress and post‐traumatic stress symptoms.
A high proportion (37%) of respondents in this study returned a PCL‐C score consistent with probable PTSD, indicating high levels of distress and post‐trauma stress symptoms in relation to their experiences. This contrasts strongly with a previous meta‐analysis, indicating a PTSD prevalence of around 3% in general prenatal populations and 19% in high‐risk populations,6 although an American study exploring the impact of maternity care changes on birth trauma during the pandemic reported 72% of their sample were partially symptomatic for PTSD.28 Distress and trauma are significantly correlated with adverse perinatal outcomes,29 and may progress to diagnosable mental health conditions such as PTSD. Stress, distress in pregnancy, post‐trauma symptoms, and PTSD can all have significant consequences for mothers, babies, and families across the lifespan, including adverse effects on fetal brain development and infant neurodevelopment,30, 31 insecure or disorganized parent–baby attachment style,32, 33 reduced parenting satisfaction,34 and negative effects on lactation35 and even on future fertility and reproductive choices.36, 37 The serious and wide‐reaching consequences of distress, trauma, and PTSD occurring in the perinatal period need greater consideration in maternity care pathways, such as improved identification, responses, and treatment of the high proportions of pregnant people experiencing these conditions, particularly in marginalized or already disadvantaged populations, as our findings indicated higher PCL‐C scores in many of these groups.
Most participants in our study demonstrated moderate levels of expectations and satisfaction with elements of their prenatal ultrasound care, however, expectations and satisfaction levels were negatively affected if participants experienced unexpected ultrasound findings or returned a high PCL‐C score. While it is conceivable that these latter cohorts would have different care needs, the study results suggest that these needs were not met. The PESPC question relating to satisfaction with ‘not having to repeat your story at each ultrasound’ was rated lowest for satisfaction, and this was reflected more strongly in those with a PCL‐C score of 26 or more. While clinical care may require practitioners to confirm the clinical history or understanding of their patients, this finding demonstrates that requiring patients to re‐tell or repeat parts of their history is likely triggering or re‐traumatizing for people with trauma, and more sensitive considerations are needed. Increasing continuity of care for prenatal ultrasounds would not only address the above factor but also address the factor with lowest score relating to expectations (seeing the same provider for multiple ultrasounds).
Reduced satisfaction with perinatal care is linked to poorer outcomes,9 similarly, increasing satisfaction with maternity care services can result in better health outcomes for mothers and babies.7 Thus, it is possible that measures to address and increase satisfaction with prenatal care, particularly in at‐risk groups, may also improve outcomes. Existing guidelines provide evidence‐based guidance in the setting of unexpected or concerning prenatal ultrasound findings.38, 39 Information quality, provider empathy, privacy, and individualized language are factors valued by consumers in these circumstances39; and health services should prioritize practices, processes, and clinical supports for sonographers in order to facilitate parent‐centered care. These factors align with trauma‐informed practice principles,40 which strengthens the argument for integrating care for trauma‐related needs into maternity care and would address the additional needs of people with trauma‐ and stress‐related symptoms and disorders without harm to clinicians or other consumers. This approach can also assist in buffering the impact of any future public health measures or changes to care. Integrating trauma‐responsive principles in maternity care would require systematic education and training for maternity care clinicians with regards to psychological trauma and its sequelae, implementation of trauma‐sensitive screening and response strategies, and policies and procedures that seek to avoid re‐traumatization of individuals.40, 41
Pregnancy in 2020, representing the initial stages of the pandemic, was associated with a high PCL‐C score, but pregnancy in 2021 and 2022 was not. Other research suggests this likely reflects the panic that was experienced at the onset of the pandemic in relation to the unknown of the pandemic on perinatal outcomes and the rapid changes to maternity care, as well as public health measures to limit virus transmission.16 However, many of these changes and measures acted to reduce social support available to pregnant women,42 and our findings add to existing evidence that removal of partners or support for pregnant people during ultrasounds had negative consequences on parental experiences, maternal support, and bonding.23 Having support during the perinatal period is a crucial element of safe and respectful maternity care, providing emotional support and comfort, improving satisfaction with the experience of perinatal outcomes,28, 43 and the presence of a support person is strongly desired by pregnant women.4 Limitation of support denies pregnant people access to this essential element of pregnancy and the benefits associated with support. Distress and post‐traumatic stress symptoms are also experienced by partners of pregnant people after traumatic events.44 Partners who feel excluded during perinatal care are more likely to develop distress, with possible subsequent implications on their relationships, parent–child bonding, and child development.10, 23 The perspectives and experiences of partners were not examined as part of this study, however, their perceptions of maternity care during the pandemic are important considerations for future research.
Additionally, results showed that vulnerable groups may be disproportionately impacted, which correlates with other research indicating social, racial, and ethnic disparities in post‐traumatic symptomatology in childbearing women.45, 46 In particular, anxiety and depressive symptoms are predictive of low social support in pregnant women46; the restriction of accompanying support in prenatal care may have exacerbated mental health symptomatology or perception of poor support in many pregnant women. The inconsistency of ultrasound restrictions across health services also likely exacerbated existing inequalities and those who could access and afford private maternity care with fewer restrictions, such as those where partners were able to be present, did so.18
Implications for practice and policy
4.1
Notably, the findings of this study that relate to post‐trauma symptoms in association with prenatal ultrasound highlight the phenomenon of ‘ultrasound trauma’, affecting a considerable number of people accessing maternity care. Maternity care clinicians need to be aware of the potential for previous trauma in relation to prenatal ultrasounds, and, in alignment with trauma‐informed practice (TIP) principles, provide consumers with safe, individualized, and flexible choices for decision‐making and care relating to prenatal ultrasounds. Early and universal screening for traumatic stress conditions would allow maternity care clinicians to detect, support, and offer treatments and trauma‐responsive care options.47 However, most clinicians have little to no prior education and training relating to perinatal trauma and would require education to equip them with knowledge and skills to confidently implement trauma‐informed care.48
Strengths and limitations
4.2
This cross‐sectional study benefits from a large sample size which includes representation from many diverse groups of society. Importantly, this study contributes important knowledge to the available literature on perinatal psychological trauma and trauma symptomatology during pregnancy and in relation to prenatal ultrasounds.
Recall, response, and selection biases may impact our findings. Convenience sampling increases risk of selection bias by assessing a less representative sample of the study population,49 and our sample was highly educated and predominantly of white/European ethnicity. However, participant characteristics in this sample were in many ways reflective of the general childbearing population in Australia, but further research could examine other diverse populations such as First Nations, and culturally and linguistically diverse groups.
Given the effect of trauma on memory, it is plausible that participants in this study who experienced acute stress disorder or PTSD also remember their experiences in a different way (e.g., vivid, distorted, or repressed memory) than those unaffected by post‐trauma disorders. Similarly, time since the experience/s with prenatal ultrasound was not assessed, and this can affect recall and post‐trauma symptomatology. People with perceived positive or negative experiences with pregnancy ultrasounds during the pandemic may be more motivated to share their experience and participate; PTSD symptoms such as avoidance tendencies or intrusions may affect willingness to participate and/or disclose their experiences. Nonetheless, our sample comprised a higher proportion of individuals with a PTSD diagnosis, or a PCL‐C score consistent with probable PTSD, which is greater than the estimated prevalence of PTSD in pregnant or postpartum populations.6 This finding alone warrants serious consideration from maternity services, policymakers, and researchers with respect to provision of safe and trauma‐responsive care.
Participants needed to be able to read and write in English in order to complete the survey; the experiences of those without sufficient English language skills are not known. There are individual and organizational circumstances, such as practice variations, that influence experiences with prenatal ultrasounds and thus more research is required to determine the global generalizability of this study's findings. Our study comprised a high proportion of people with PTSD or a high PCL‐C score. The study design did not allow for gold‐standard clinical interviewing to confirm a PTSD diagnosis, however, while some contention exists suggesting that the PCL self‐report measure can inflate prevalence estimates of PTSD, a large systematic review and meta‐analysis demonstrated this measure produces results consistent with clinical interviewing and assessments for diagnosis and monitoring of post‐traumatic symptoms.6
CONCLUSIONS
5
This study provides a meaningful insight into the experiences of prenatal ultrasound during the pandemic in Australia. Of significant concern are the large numbers of participants returning PCL‐C scores consistent with PTSD, and the trauma and stress experienced in relation to pandemic ultrasound restrictions, including the limitation of support persons attending ultrasounds.
Prenatal ultrasounds where uncertain or abnormal findings were experienced, or involving pregnancy loss, were significantly associated with high PCL‐C scores, highlighting that ‘ultrasound trauma’ is a very common and valid phenomenon contributing to perinatal psychological trauma and stress‐related disorders.
The findings of this study represent an important opportunity to consider approaches to enhancing prenatal care in ways that would meet consumer expectations, optimize experiences, and reduce distress. Implementation of trauma‐informed education and practice across the spectrum of maternity care would result in service delivery that is truly person centered, safe, and compassionate, reduce the likelihood of situations that may prompt distress or a trauma response in traumatized individuals, and will not result in harm for clinicians or consumers.
CONFLICT OF INTEREST STATEMENT
The authors declare no conflicts of interest.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Clinical Practice Guidelines: Pregnancy Care (Australian Government Department of Health). 2020.
- 2WHO antenatal care recommendations for a positive pregnancy experience. Maternal and fetal assessment update: imaging ultrasound before 24 weeks of pregnancy (World Health Organization). 2022.35442602 · pubmed ↗
- 3Skelton E , Webb R , Malamateniou C , Rutherford M , Ayers S . The impact of antenatal imaging on parent experience and prenatal attachment: a systematic review. J Reprod Infant Psychol. 2022;42:22‐44. doi:10.1080/02646838.2022.2088710 35736666 · doi ↗ · pubmed ↗
- 4Van der Zalm JE , Byrne PJ . Seeing baby: women's experience of prenatal ultrasound examination and unexpected fetal diagnosis. J Perinatol. 2006;26(7):403‐408. doi:10.1038/sj.jp.7211540 16801957 · doi ↗ · pubmed ↗
- 5Cristofalo EA , Di Pietro JA , Costigan KA , Nelson P , Crino J . Women's response to fetal choroid plexus cysts detected by prenatal ultrasound. J Perinatol. 2006;26(4):215‐223. doi:10.1038/sj.jp.7211489 16554849 · doi ↗ · pubmed ↗
- 6Yildiz PD , Ayers S , Phillips L . The prevalence of posttraumatic stress disorder in pregnancy and after birth: a systematic review and meta‐analysis. J Affect Disord. 2017;208:634‐645. doi:10.1016/j.jad.2016.10.009 27865585 · doi ↗ · pubmed ↗
- 7Galle A , Van Parys A‐S , Roelens K , Keygnaert I . Expectations and satisfaction with antenatal care among pregnant women with a focus on vulnerable groups: a descriptive study in Ghent. BMC Womens Health. 2015;15(1):112. doi:10.1186/s 12905-015-0266-2 26627054 PMC 4667492 · doi ↗ · pubmed ↗
- 8Perriman N , Davis D . Measuring maternal satisfaction with maternity care: a systematic integrative review: what is the most appropriate, reliable and valid tool that can be used to measure maternal satisfaction with continuity of maternity care? Women Birth. 2016;29(3):293‐299. doi:10.1016/j.wombi.2015.12.004 26782087 · doi ↗ · pubmed ↗