A Systematic Review on the Dual Role of Interleukin-1 in CAR T-Cell Therapy: Enhancer and Mitigator
Amirhosein Maali, Ahmad Noei, Saba Feghhi-Najafabadi, Zahra Sharifzadeh

TL;DR
This review explores how interleukin-1 both boosts and limits the effectiveness of CAR T-cell therapy, offering strategies to improve its safety and use.
Contribution
The paper systematically reviews the dual role of IL-1 in CAR T-cell therapy, offering insights into balancing efficacy and toxicity.
Findings
IL-1 enhances CAR T-cell activation and persistence but also drives toxicities like CRS and ICANS.
Strategies to mitigate IL-1-driven toxicities show promise in reducing adverse effects without harming therapeutic outcomes.
Understanding IL-1's role could lead to optimized treatment strategies for safer and broader CAR T-cell therapy use.
Abstract
Chimeric antigen receptor T-cell therapy is a groundbreaking approach for treating certain hematologic malignancies and solid tumors. However, its application is limited by severe toxicities, particularly CRS and ICANS, dramatically limit its broader application. IL-1 plays a crucial role in both enhancing CAR T-cell efficacy and driving these toxic effects. This review systematically examines the dual functions of IL-1, highlighting its role in promoting CAR T-cell activation and persistence while contributing to CRS and ICANS pathogenesis. Strategies to mitigate IL-1-driven toxicities, including IL-1 receptor antagonists, monoclonal antibodies, IL-1 trapping, and interference with IL-1 production, show promise in reducing adverse effects without compromising therapeutic efficacy. Understanding the complex role of IL-1 in CAR T-cell therapy may lead to optimized treatment strategies,…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
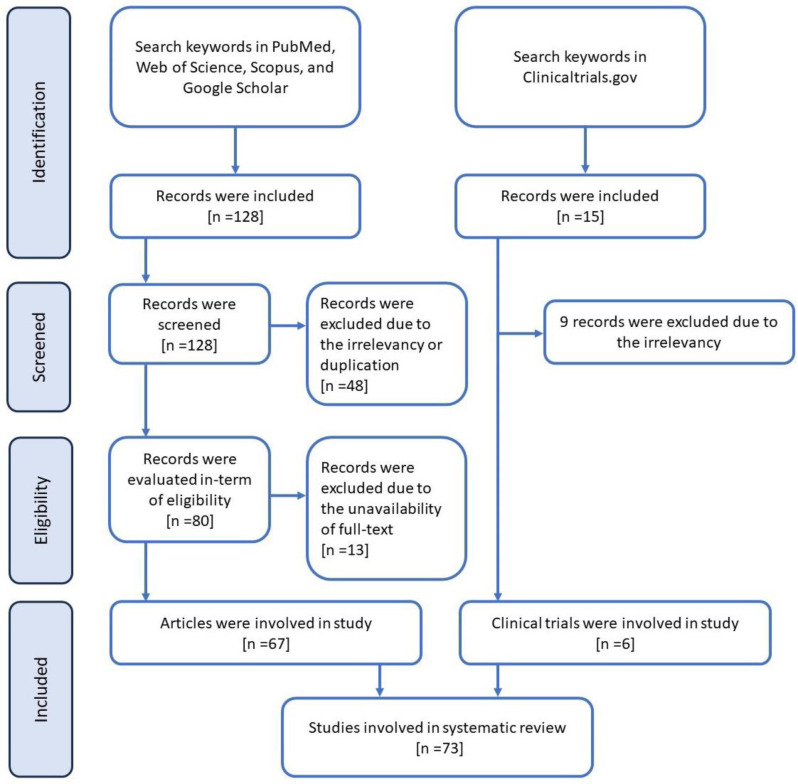 Fig. 1
Fig. 1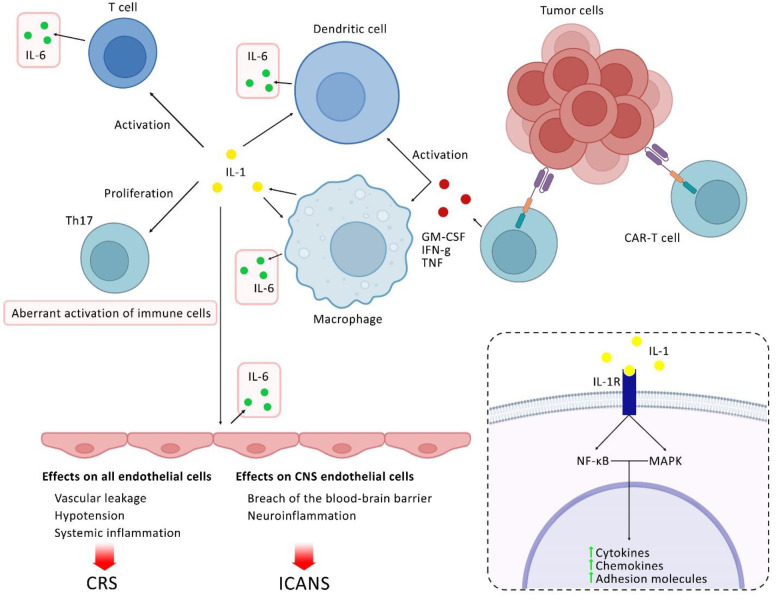 Fig. 2
Fig. 2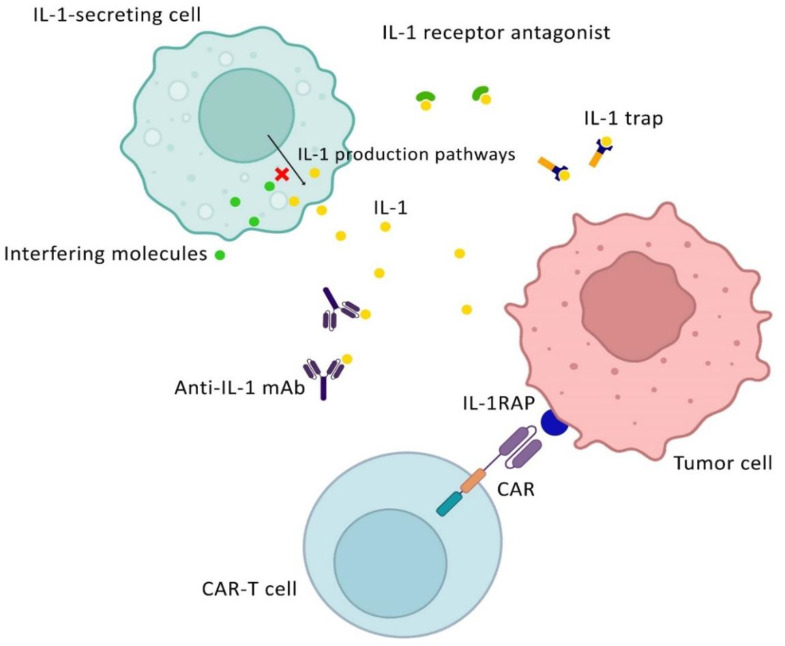 Fig. 3
Fig. 3| Study title | Study status | Conditions | Phases | Enrollment | NCT number |
|---|---|---|---|---|---|
|
| Active not recruiting | B cell ALL and B-cell non-Hodgkin lymphoma | 2 | 62 | |
|
| Active not recruiting | B-cell non-Hodgkin lymphoma | 2 | 27 | |
|
| Completed | Acute myeloid leukemia | NM | 86 | |
|
| Completed | B-cell non-Hodgkin lymphoma | 2 | 22 | |
|
| Recruiting | Diffuse large B-cell lymphoma | 2 | 36 | |
|
| Active not recruiting | Non-Hodgkin lymphoma | 2 | 15 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCAR-T cell therapy research · Viral Infectious Diseases and Gene Expression in Insects · Virus-based gene therapy research
INTRODUCTION
CAR T-cell therapy represents a breakthrough in oncology, using immune modification to target and eliminate cancer cells^[^^1^^]^. This approach involves ex vivo genetic engineering of autologous/ allogenic T cells to express CARs on their surface, thus enhancing their ability to identify and destroy cancer cells upon reinfusion into the patient. Similar to other cancer treatment modalities, CAR T-cell therapy is tailored to address different types of hematologic malignancies, particularly those that have proven resistant to standard therapies^[^^2^^,^^3^^]^. Clinically, CAR T-cell therapy has demonstrated remarkable success, particularly in treating refractory or relapsed B-cell malignancies. For instance, in cases of acute lymphoblastic leukemia, CAR T-cell therapy has achieved complete remission rates exceeding 80%, offering hope to patients who have exhausted conventional treatment options. Similarly, in large B-cell lymphoma, CAR T-cell therapy has provided durable responses, leading to its approval by regulatory agencies for specific indications. These successes underscore the transformative impact of CAR T-cell therapy in oncology, highlighting its potential to revolutionize cancer treatment paradigms^[^^3^^,^^4^^]^. The approval of CAR T-cell therapies indicates a significant advancement, marking the integration of immunotherapy into future oncologic treatments. The versatility of CAR T-cell therapy is being further explored in the context of solid tumors, expanding its implications beyond hematologic malignancies^[^^5^^-^^7^^]^.
Structurally, CARs consist of three primary components: an extracellular antigen-binding domain, typically derived from a single-chain variable fragment of an antibody, a transmembrane domain that anchors the receptor to the T-cell membrane, and an intracellular signaling domain responsible for activating the T-cell upon antigen recognition. This engineered configuration enables CAR T cells to identify and eliminate cancer cells in an MHC-independent manner, thereby enhancing their therapeutic potential^[^^8^^]^. Peripheral blood mononuclear cells are collected from the patient through leukapheresis, isolating T cells for CAR T-cell manufacturing. The T cells are activated ex vivo to promote proliferation and are then genetically modified with CAR constructs using viral vectors, such as lentiviruses. After transduction, the CAR-expressing T cells are expanded, undergo rigorous quality control, and are cryopreserved until they are ready for patient infusion^[^^9^^]^.
The concept of CAR T-cell therapy recognizes that cytokines, particularly IL-1, play a crucial role in mediating immune responses, which is essential for the success of therapy. IL-1 is a proinflammatory cytokine that is pivotal in stimulating and expanding CAR T cells to enhance their anti-tumor activity^[^^10^^]^. However, IL-1 is associated with a serious, life-threatening side effect known as CRS, which is typically characterized by a significant increase in cytokine levels. This trend can lead to symptoms ranging from mild fever to severe multi-organ dysfunction^[^^11^^,^^12^^]^. Additionally, IL-1 has a dual capacity to support immune efficacy, while simultaneously influencing the development of CRS^[^^13^^]^. Moreover, ICANS is another major side effect of CAR T-cell therapy, manifesting in neural symptoms.
The design of the CAR construct can influence the incidence and severity of CRS. The intracellular signaling domain of the CAR typically incorporates co-stimulatory motifs such as CD28 or 4-1BB, which is responsible for T-cell activation and cytokine production. For instance, CARs containing CD28 co-stimulatory domains may facilitate more rapid T-cell activation and increased cytokine release, including IL-1, compared to those utilizing 4-1BB domains. Likewise, high-affinity CARs or those expressed at elevated densities on T cells can lead to robust activation upon antigen engagement, potentially resulting in excessive cytokine production, including IL-1. Modulating the affinity and expression levels of CARs can help mitigate this risk. Furthermore, the extracellular spacer or hinge region of the CAR affects its flexibility and distance from the T-cell surface, influencing the interaction of CAR with the target antigen and subsequent T-cell activation, thereby impacting cytokine release profiles^[^^14^^]^.
This newly enhanced understanding of cytokine dynamics in CAR T-cell therapy is advancing the development of ever-more-refined treatments that can balance efficacy and potentially revolutionize paradigms in treating cancer with this powerful approach to immunotherapeutics and treat a wider scope of diseases. While IL-1 enhances CAR T-cell efficacy, its role in inducing adverse events remains a significant challenge. This review aimed to systematically evaluate the dual roles of IL-1 and explored potential strategies for decreasing toxicity without compromising efficacy.
MATERIALS AND METHODS
A comprehensive search was conducted using existing databases, including PubMed, Web of Science, and Scopus, up to May 2024. The search terms used in the research entailed “IL-1”, “CAR T-cell therapy”, “cytokine release syndrome”, “neurotoxicity”, and “IL-1 blockade”'. The search identified all eligible published articles, including original articles, reviews, systematic reviews, meta-analyses, and clinical trials (available at https://clinicaltrials.gov/). This database reports the effects of IL-1 in the context of CAR T-cell therapy. All in vitro, in vivo, and ex vivo studies were included, while non-English language publications were excluded.
RESULTS
Summary of data representation
A total of 128 articles were identified through searches in different databases. Irrelevant articles were excluded, resulting in 67 articles that met the eligibility criteria for inclusion in this study. Also, 15 clinical trials were found through searches using relevant keywords, of which 6 were associated with the subject and included in the study (Fig. 1). The content of articles and trials was categorized into six major themes: (1) the role of IL-1 in immune response, (2) the impact of IL-1 on the activation and expansion of CAR-T cells, (3) the modifying role of IL-1 in modulating tumor microenvironment, (4) the related toxicities of CAR T-cell therapy and the role of IL-1, (5) strategies for IL-1 blockade, and (6) the potential benefits and challenges of IL-1 blockade.
Function of IL-1 in immune response
Central to the immune system, IL-1 serves as a crucial mediator of inflammatory processes and immune regulation. This cytokine plays an essential role in defending against infections, as well as injuries, and exists mainly in two forms, IL-1α and IL-1β. Both forms exert their effects by binding to the IL-1R on target cells, activating the NF-κB and MAPK signaling pathways, which amplify inflammation and activate immune cells. Upon IL-1 binding, MyD88 and other adaptor proteins are recruited to the receptor complex, initiating downstream signaling cascades^[15]^. Activating NF-κB leads to the transcription of numerous pro-inflammatory genes, including cytokines, chemokines, and adhesion molecules that facilitate immune cell activation and recruitment. Additionally, activation of the MAPK pathways, comprising ERK, JNK, and p38 MAPK, promotes the production of inflammatory mediators and further enhances the immune response. This process stimulates the release of secondary cytokines and chemokines, such as MCP-1, RANTES, and CXCs, which subsequently recruit and activate a broad range of immune cells, including T cells, B cells, macrophages, and neutrophils^[16-18]^. IL-1 is secreted by macrophages, dendritic cells, and endothelial cells^[10]^. It is the principal pro-inflammatory cytokine and is well-known for its fever-inducing properties. IL-1 upregulates the expression of adhesion molecules on the endothelium and recruits immune cells to the sites of injury or infection. Besides these pro-inflammatory effects, IL-1 significantly influences the activation, proliferation, and differentiation of T cells and dendritic cells, which are central to the acquired immune response^[19]^. As an example, IL-1β acts as a dominant signal for the differentiation of naïve T cells into the Th17 cells, a lineage of T helper cells that is critical for the immune response to fungal and bacterial infections and it has also been associated with various autoimmune diseases. Furthermore, IL-1 plays important roles in tissue repairing and regeneration by stimulating fibroblast proliferation and collagen synthesis, both of which are essential for wound healing^[20,21]^. However, uncontrolled IL-1 signaling can lead to tissue damage, highlighting the need to regulate its activities. Conversely, due to the potent pro-inflammatory nature of IL-1, its dysregulation is associated with many autoimmune and chronic inflammatory diseases, such as rheumatoid arthritis, gout, and systemic lupus erythematosus. This association has promoted the development of therapies targeting IL-1 to decrease exaggerated inflammation and alleviate symptoms in affected patients^[^^21^^,^^22^^]^.
Impact of IL-1 on activation and expansion of CAR T cells
IL-1 activates and expands CAR T cells through at least two essential processes that are vital for the effectiveness of cancer treatment. This behavior is primarily due to its strong pro-inflammatory and immunomodulatory activities. IL-1 functions as a critical alarm cytokine that signals danger, significantly enhancing the maturation and antigen-presenting capacity of dendritic cells. This augmentation is necessary for the successful priming of T cells, including CAR-T cells, which is essential for their activation upon encountering antigens in vivo conditions^[^^23^^]^. IL-1 also promotes T-cell proliferation by stimulating the expression of IL-2 and its receptor (IL-2R), both of which are required for T-cell expansion^[^^23^^]^. This signaling loop is necessary for the mass expansion of activated T cells and the effective eradication of tumors. In addition, by regulating apoptotic signaling, IL-1 prolongs the lifespan of CAR T cells, which is essential for sustaining antitumor activity. Furthermore, IL-1 signaling is important for the development of memory T-cell subsets, which are required for providing long-term immunity and contribute to durable responses following CAR T-cell therapy^[^^24^^]^.
Altering the function of IL-1 in modulating TME
IL-1 reprograms the TME to facilitate T-cell infiltration, activation, and maintenance, working in conjunction with other cytokines to establish an environment to support T-cell activity. This dual role of IL-1 promotes tumor progression while enhancing immune surveillance and highlights its complex involvement in CAR T-cell therapy^[10]^.
Treatment-related toxicities of CAR T-cell therapy
The most frequent and severe side effect associated with CAR T-cell therapy is CRS, which is mediated by the substantial increase in cytokine level released by activated CAR T cells. Clinical manifestations of CRS range from fever, tachycardia, and hypotension to tachypnea and hypoxia. Severe cases may lead to multi-organ failure^[25-27]^. Another significant adverse effect is ICANS, with symptoms reported as delirium, headache, aphasia, seizures, and cerebral edema. ICANS is directly related to the increased disease burden, higher doses of administered CAR T cells, and subsequent severe CRS. Other systemic effects include prolonged cytopenia, which makes the affected individual more susceptible to infections, and coagulopathies, such as disseminated intravascular coagulation. Cardiovascular effects may include hypotension and arrhythmias. Renal and hepatic effects can manifest as acute kidney injury and elevated liver enzymes, respectively. Respiratory complications may include hypoxemia and pulmonary edema, as reported in the literature^[^^25^^,^^28^^]^.
Role of IL-1 in CRS
IL-1 is a central mediator in the pathophysiology of CRS after adoptive CAR T-cell therapy and serves as the primary orchestrator of this hyperinflammatory response. T cells stimulate the upregulation of IL-1 from macrophages^[10,29]^. Notably, IL-1 is produced several hours earlier than IL-6 during CRS. Since IL-1 triggers the secretion of IL-6 and soluble IL-6 receptor, it is hypothesized that the release of IL-1 from peripheral monocytes and macrophages initiates the development of CRS^[^^30^^]^. The involvement of macrophages in CRS has been confirmed in vivo, and inhibition of IL-1 leads to the reduction in CRS-related mortality associated with CAR T-cell therapy. Also, IL-1 amplifies the immune response by enhancing the production and release of other pro-inflammatory cytokines and chemokines, including TNF-α and IFN-γ^[31]^. This cascade of cytokines creates a feedback loop that continuously recruits and activates immune cells, leading to an intensified and systemic inflammatory response. In addition, IL-1 influences the endothelial cells, inducing the expression of adhesion molecules that line up the blood vessels, facilitating the infiltration of more immune cells into the tissues and exacerbating inflammation. This process results in edema, hypotension, and, in severe cases, capillary leak syndrome, contributing to multi-organ dysfunction observed in severe CRS. IL-1 is a pyrogenic cytokine that mediates fever and the systemic manifestations of CRS by its effect on the hypothalamus^[32]^. Its systemic effects also lead to fatigue, myalgia, and malaise. Through its extensive pro-inflammatory actions, IL-1 exacerbates cardiovascular symptoms such as tachycardia, hypotension, and subsequent shock. Furthermore, it promotes inflammation and increases permeability in pulmonary tissues, resulting in hypoxia and complications associated with acute respiratory distress syndrome^[33,34]^. Increased levels of IL-1 after CAR T-cell infusion is strongly correlated with increased severity of CRS. Patients who developed severe CRS, exhibited higher serum levels of IL-1β shortly after infusion, suggesting that IL-1 could serve as a predictive marker for assessing the risk of CRS development. Early detection through IL-1 monitoring could facilitate the timely administration of IL-1 blocking agents to mitigate CRS severity. This predictive capability of the IL-1 level will enable proactive measures to prevent possible complications^[11]^. Additionally, the role of IL-1 extends beyond merely indicating risk; it also plays a crucial part in shaping therapeutic strategies within the complex landscape of stroke diagnosis and treatment^[^^29^^]^. Conversely, the dynamics of IL-1 in response to stimulation can exhibit significant variability among patients, necessitating continuous monitoring or a targeted approach to utilizing IL-1 as a biomarker. Indeed, the remarkable complexity of cytokine cross-talk in CRS also suggests the need for a comprehensive suite of biomarkers, with IL-1 potentially at the core, to enhance the accuracy of prediction and management of CRS^[35]^. Effective management of CRS through IL-1 modulation not only addresses immediate concerns but also enhances long-term efficacy and survival rates associated with CAR T-cell therapies. This approach may ultimately cause sustained remission in certain types of cancer. As a biomarker, IL-1 facilitates the development of personalized management strategies for CRS, enabling clinicians to offer interventions tailored to each patient's risk profile. The proactive use of IL-1 inhibitors can significantly reduce the extent and severity of CRS. Furthermore, incorporating IL-1 monitoring into post-infusion care protocols will improve the safety and accessibility of CAR T-cell therapy, hence benefiting a larger patient population^[^^36^^]^.
Role of IL-1 in ICANS
Neurotoxicity, manifested as ICANS, is a complication that can arise following CAR T-cell therapy. Several factors contribute to neurotoxicity, including mechanisms related to endothelial activation, glial injury, cytokine-mediated effects, off-tumor on-target toxicity, and CAR T-cell infiltration^[37]^. A comprehensive molecular understanding of ICANS, particularly the role of IL-1, is urgently needed to develop effective management strategies that improve patient outcomes. IL-1 may facilitate the disruption of the blood-brain barrier, allowing cytokines to infiltrate the CNS and contribute to the neuroinflammatory process^[36]^. Patients may exhibit neurological symptoms such as headache, confusion, seizures, and, in rare cases, cerebral edema, which collectively characterize the clinical features of ICANS. IL-1β is considered a key effector in the development of human autoinflammatory diseases that are not mediated by T-lymphocyte autoimmunity. Brain endothelial cells express IL-1R type 1; hence, a paracrine loop between infiltrating immune cells and the brain endothelium may enhance IL-1β activity and exacerbate neuroinflammation, contributing to the development of ICANS^[38]^. Additionally, ICANS is associated with elevated levels of other cytokines, including IL-6, IFN-γ, and IL-15. These cytokines exacerbate neurotoxicity through various mechanisms, including the cytokine-mediated trafficking of CAR T cells into the CNS. The presence of CAR T cells has been detected in cerebrospinal fluid, which correlates with neurotoxic events. This finding suggests that CAR T cell infiltration into the CNS may play a role in the development of ICANS^[31]^. The blockade of IL-1β has shown potential in inhibiting endothelial dysfunction, which is critical for mitigating neurotoxicity associated with CAR T-cell therapy. Also, increased serum IL-1 level is positively correlated with the severity of ICANS. Therefore, monitoring IL-1 level post-CAR T-cell infusion could be a vital strategy for determining the optimal timing for administering IL-1 blocking agents to mitigate ICANS severity^[33]^. The involvement of IL-1 in ICANS emphasizes its dual function in both diagnosis and therapy. Due to its early elevation, individuals at higher risk for neurotoxicity may be identified and treated proactively to prevent adverse effects. Given the complex interactions among cytokines in ICANS, a comprehensive panel of biomarkers, including IL-1, may be necessary for more precise predictions of neurotoxicity and effective treatment^[34,39]^. Furthermore, the neuro-symptom checklist and neurocognitive testing are crucial for early diagnosis and systematic assessment, leading to improved management of ICANS^[^^30^^]^ (Fig. 2).
Clinical management strategies for CRS and ICANS
In addition to CAR T-cell therapy, autoimmune disorders, severe infections, COVID-19, hematopoietic stem cell transplantation, and other medical conditions may lead to CRS and ICANS^[40]^. Effective management techniques are crucial in CAR T-cell therapy to reduce the incidence of CRS and ICANS while enhancing patient outcomes. Corticosteroids, such as methylprednisolone and dexamethasone, are frequently employed in CAR T-cell treatment to suppress inflammation and alleviate the severity of CRS^[41,42]^. However, the use of corticosteroids may diminish the effectiveness of CAR T cells and impair their functionality, necessitating careful management of their administration. Tocilizumab and other anti-IL-6 medications are often used to treat CRS. However, tocilizumab may not adequately penetrate the CNS and are unable to consistently reduce neurotoxicity. Furthermore, given the complex cytokine environment driving CRS and ICANS, inhibiting IL-6 alone may be inadequate. Also, broad cytokine blocking may excessively suppress the immune system in cases of sepsis and severe infections, potentially resulting in secondary infections^[^^43^^]^. By reducing brain inflammation and edema, corticosteroids are beneficial in managing ICANS; however, they might suppress the immune system and cause long-term adverse effects, such as myopathy and increased susceptibility to infections. Prolonged use of corticosteroids may also result in diabetes and osteoporosis^[44]^. Intrathecal injection of corticosteroids, e.g., hydrocortisone, has been used to rapidly decrease CNS inflammation in severe cases; nevertheless, this invasive procedure has its own risks and complications^[45]^. Furthermore, antipyretics, antiepileptics, and benzodiazepines serve as supportive care for managing ICANS. Patients experiencing seizures are often treated with antiepileptic medications such as levetiracetam; nonetheless, these medications may produce adverse effects, including fatigue and dizziness. Therefore, targeting and effectively reducing CRS and ICANS through IL-1 blockade offers substantial advantages over conventional therapies, with fewer side effects. This strategy is a crucial component of the evolving field of immune-based therapies, as it not only improves short-term clinical outcomes but also promotes long-term safety and efficacy^[^^30^^]^.
IL-1 blockade strategies
The management of CRS and ICANS remains a significant barrier to the wider application of CAR T-cell treatments, highlighting the need for advancements such as IL-1 blockade to enhance patient outcomes^[10]^. By reducing the inflammatory reactions that can result in severe CRS or ICANS, IL-1 inhibition strategies aim to improve treatment efficacy and patient safety.
IL-1 receptor antagonists
The human IL-1 receptor antagonist is available in recombinant form as anakinra. It functions similarly to the natural antagonist of the IL-1 receptor by competitively preventing IL-1 molecules, including both IL-1α and IL-1β, from binding to the type I receptor, which is found on a variety of cell types, including endothelium and immune cells^[46]^. Anakinra effectively stops the cascade of cellular signaling events that lead to systemic inflammation by obstructing this pathway. Its broad regulatory effects on inflammation are shown by its use in treating rheumatoid arthritis, neonatal-onset multisystem inflammatory disease, hemophagocytic lymphohistiocytosis, and macrophage activation syndrome, as well as its application in alleviating CRS symptoms following CAR T-cell therapy^[30,47,48]^. Anakinra has been shown to significantly lessen the severity of CRS and decrease the likelihood of progression to severe neurotoxicity when administered promptly after CAR T-cell infusion or at the onset of early CRS symptoms^[49]^. In a study conducted by Gazeau et al., the safety and effectiveness of anakinra in treating patients with refractory B-cell or plasma cell malignancies who experienced CRS and ICANS after CAR T-cell treatment were evaluated. From 2019 to 2022, 43 patients from the United States and Spain participated in this retrospective study. Overall, anakinra was found to be safe, with very few patients discontinuing the medication due to adverse effects. Higher doses of anakinra were associated with significantly decreased treatment-related mortality and a quicker resolution of CRS/ICANS, indicating that anakinra may be beneficial in managing severe side effects of CAR T-cell therapy without compromising its efficacy^[49]^. Anakinra is also well-known for its exceptional penetration into CSF. Preclinical research indicates that IL-1 is directly linked to the neurotoxicity caused by CAR T cells, as shown in humanized mice treated with human CD19 CAR T cells. In this research, mice that received pretreatment with anakinra were able to avoid convulsions and widespread paralysis. Meningeal infiltration of human monocytes accompanied these neurological symptoms, which appear long after the remission of CRS but do not cause any alterations to the CNS parenchyma^[50]^. In the context of CAR T-cell therapy, a mouse model described by Norelli et al. closely resembles important features of CRS and ICANS observed in leukemia CAR T-cell treatment. The administration of CAR T cells to the humanized mice with significant leukemia burdens resulted in severe CRS, characterized by fever and elevated levels of IL-6, primarily produced by human monocytes. Tocilizumab mitigated CRS by inhibiting the IL-6 receptor; however, it had no effect on neurotoxicity. In contrast, anakinra therapy effectively reduced both neurotoxicity and CRS, thereby improving the leukemia-free survival of the mice. This model suggests potential strategies for enhancing the safety of CAR T-cell treatments^[30]^. Wehrli et al. performed a retrospective analysis of 14 patients who received anakinra treatment for steroid-refractory ICANS with or without CRS following tisagenlecleucel (Kymriah) or axicabtagene ciloleucel (Yescarta) CAR T-cell therapy^[35]^. Their research indicated that fever, inflammatory cytokines, and indicators of ICANS/CRS all decreased significantly and quickly after the administration of anakinra. Anakinra was administered as three subcutaneous doses per day; it did not have a discernible effect on neurotoxicity and did not speed up the tapering of corticosteroids. While thrombocytopenia and neutropenia were frequent side effects at the time of dosing, no anakinra-related infections or delays in hematological recovery were reported. Although anakinra appears to be a beneficial adjunct to steroids and tocilizumab in these conditions, further prospective trials are necessary to thoroughly evaluate its efficacy in managing CRS and/or steroid-refractory ICANS after CAR T-cell treatments. Anakinra was investigated in patients undergoing CD19 CAR T-cell therapy for mantle cell lymphoma and relapsed/refractory large B-cell lymphoma in a phase II clinical study. Anakinra was given from day 2 to at least day 10 after the infusion, significantly reducing the incidence of severe ICANS without impairing the effectiveness of the treatment. With a complete response rate of 65% and an overall disease response rate of 77%, anakinra may serve as a valuable treatment for neurotoxicity in CAR T-cell patients^[46]^. A further clinical study (NCT04148430) was conducted to assess the efficacy of prophylactic anakinra in mitigating the side effects linked to CAR T-cell therapies. Starting on the second day of CAR T-cell infusion, patients received anakinra, which successfully decreased the incidence of severe CRS and ICANS. After moderate use of corticosteroids and tocilizumab for one month, 74% of individuals demonstrated a response to treatment. Preliminary research suggests that serious complications arising from CAR T-cell treatment may be significantly reduced through IL-1 suppression^[51]^. In another clinical trial, anakinra is administered intravenously daily from days 0 to 13, in addition to the CAR T-cell infusion on day 0 (NCT04359784). The issues associated with CRS and ICANS are specifically addressed in this experiment. The main outcome measure employs a Bayesian optimal phase II design for evaluation, focusing on the absence of any grade of CRS within 28 days post-infusion. Additionally, as a phase II trial, NCT04432506 aimed to determine the optimal dose and efficacy of anakinra in reducing adverse effects related to axicabtagene ciloleucel (axi-cel) CAR T-cell treatment in patients with relapsed or refractory large B-cell lymphoma. Another phase II, single-center, open-label clinical trial, NCT04150913, evaluated the effectiveness of anakinra in preventing neurotoxicity in patients undergoing CAR T-cell treatment for relapsed or refractory large B-cell lymphoma. Eligible participants for this trial must not have received prior CAR T-cell treatment or had a CNS disease. According to the treatment protocol of the study, participants received anakinra starting 4 hours before the axi-cel infusion and continued daily administration for seven days after completing lymphodepleting chemotherapy. The primary research metrics include the rate and severity of neurotoxic events during the first 30 days post-infusion, which are compared against historical data from the Zuma-1 cohorts. Secondary measures include the overall response to the illness, the occurrence and severity of CRS, and the assessment of various biomarkers, such as blood cytokines. These results indicated that patients experienced low-grade CRS, none had severe CRS, and two individuals experienced neurotoxic episodes. All patients in this preliminary cohort exhibited a positive response to the therapy, with a 100% response rate at day 28, and the majority sustaining a complete response at the most recent follow-up, every patient in this preliminary cohort responded positively to the therapy. When comparing the findings of the study to past data, a decrease in inflammatory biomarkers after infusion was observed, suggesting that anakinra may help mitigate the adverse effects of axi-cel therapy^[52]^. Anakinra is currently being evaluated in a phase II clinical trial (NCT04205838) to determine its potential to protect patients with recurrent or refractory large B-cell lymphoma from developing severe CAR T-cell-related encephalopathy syndrome while undergoing CAR T-cell therapy. This is particularly significant as it addresses a critical need for managing neurotoxicity, which can greatly affect patient outcomes following CAR T-cell treatment. However, no published results are available at this time. Also, IL-1 blocking with anakinra has shown effectiveness in treating hemophagocytic lymphohistiocytosis and macrophage activation syndrome, both of which share laboratory and clinical characteristics with CRS^[^^30^^,^^47^^,^^48^^]^.
Monoclonal antibodies against IL-1
Canakinumab is an example of a targeted strategy that specifically inhibits IL-1β to modify the immune response^[53]^. It is a human monoclonal antibody that prevents the binding of IL-1β to its receptors. The high affinity and specificity of this antibody for IL-1β provide the added advantage of selectively targeting IL-1β without affecting other cytokines in the IL-1 family, which may help maintain certain aspects of the immune response while reducing inflammation. The ability of canakinumab to lower inflammatory markers and enhance clinical outcomes has been shown in the treatment of systemic juvenile idiopathic arthritis and other inflammatory diseases^[54]^. As mentioned previously, vascular endothelial activation is essential for the development of CRS and ICANS following CAR-T therapy. Research conducted by Chen et al. focused on TNF-α and IL-1β as the main causes of endothelial activation. They explored the potential of blocking TNF-α and IL-1β signaling as a therapeutic strategy to address endothelial dysfunction induced by CAR T-cell treatment. Their findings revealed that the interventions, including the use of a focal adhesion kinase inhibitor, an anti-IL-1β antibody, and adalimumab to decrease TNF-α levels effectively reduce endothelial activation resulting from the interaction of CAR T cells, tumor cells, and myeloid cells. Interestingly, a synergistic effect was observed between adalimumab and the anti-IL-1β antibody in blocking endothelial activation^[55]^. Therefore, the use of anti-IL-1β antibodies, such as canakinumab, shows promise in mitigating CRS and ICANS following CAR T-cell therapy.
IL-1 trapping
By fusing the human IL-1R with the Fc region of human IgG1, rilonacept (also referred to as IL-1 trap) performs a dual function by capturing and neutralizing IL-1β. This mechanism allows rilonacept to act as a decoy receptor, effectively binding to IL-1β and preventing it from interacting with its natural receptors on cell surfaces in an antagonistic manner^[56]^. Rilonacept efficiently blocks IL-1β before it can initiate inflammatory signaling pathways by sequestering the cytokine. This action decreases the overall inflammatory response and lowers the bioavailability of IL-1β, making rilonacept a valuable therapeutic option for conditions such as cryopyrin-associated periodic syndromes, which are characterized by elevated IL-1 activity. The ability of rilonacept to inhibit and reduce the impacts of IL-1β provides significant potential benefit in managing cytokine-mediated symptoms, such as CRS, in the context of CAR T-cell treatment^[^^57^^]^.
IL-1RAP targeting
As the IL-1, IL-33, and IL-36 signaling pathways are involved in inflammation and carcinogenesis, the IL-1RAP) has emerged as a promising target for tumor-associated antigens. IL-1RAP is overexpressed in various malignancies and has a role in tumor growth, making it a promising target for future therapeutic research^[58]^. To address the challenge of epitope masking resistance in AML, Warda et al. developed a switchable CAR T-cell platform. This platform incorporates a safety iCASP9/rimiducid suicide gene system together with monoclonal anti-IL1RAP single-chain variable fragment antigen-binding sequences, all delivered via a lentiviral vector. The resulting CAR T cells exhibited specific cytotoxicity against IL1RAP-expressing AML stem cells without adversely affecting CD34^+^ stem cells. This observation suggests that IL1RAP is a viable tumor-associated antigen for targeted immune therapy. When activated in the presence of primary AML cells or IL1RAP-positive cell lines, these CAR T cells demonstrated selective cytotoxicity and produced pro-inflammatory cytokines in vitro and mouse xenograft models^[59]^. In a related study, Trad et al. developed a third-generation of IL-1RAP CAR T cells to effectively eradicate AML stem cells. These CAR T cells indicated notable cytotoxicity against primary patient cells, as well as AML cell lines in vitro and in vivo conditions. Importantly, IL-1RAP CAR T cells enhanced overall survival in patient-derived xenograft models of recurrent AML by efficiently targeting primary AML cells in the spleen and bone marrow. These preclinical findings highlight the potential of IL-1RAP CAR T-cell therapy as a powerful treatment for AML; however, further clinical studies are necessary^[^^60^^]^. To manage potential side effects, Bouquet et al. developed a novel CAR treatment that targets IL-1RAP, incorporating the inducible suicide gene systems RapaCasp9-G or RapaCasp9-A. These genes, triggered by rapamycin to increase safety, are influenced by a polymorphism in caspase 9^[61]^. In this context, Nicod et al. focused on creating a CAR T-cell therapy that targets IL-1RAP for treating AML, using the CliniMACS Prodigy^TM^ system to meet good manufacturing practice-like standards. The manufacturing process was validated using research-grade lentiviral particles, and the resultant CAR T cells were evaluated in a xenograft AML murine model, demonstrating improved survival and effective tumor cell eradication. By confirming the readiness of CAR T cells for a phase I clinical trial, this validation established a reproducible procedure for producing therapeutic-grade CAR T cells^[62]^. Aiming to evaluate the developed IL-1RAP CAR T cells, a recent study by Da Rocha et al. investigated the functionality of these CAR T cells using a novel assay containing coated recombinant IL-1RAP protein to activate them. This approach serves as a substitute for the use of live cell lines. Following interaction with the coated IL-1RAP, it was shown that IL-1RAP CAR T cells could be effectively generated and stimulated ex vivo, exhibiting distinct cytotoxic responses and causing the release of IFN-γ^[63]^. Another interventional clinical trial (NCT04169022) was performed on AML using CAR T cells that target IL1RAP on leukemic cells. This study was carried out by the Centre Hospitalier Universitaire de Besancon. The trial was designed as a non-randomized, open-label, parallel assignment research and enrolled a total of 86 participants. It measured IL1RAP protein expression over two years using cytometry. Notably, this trial excluded patients with AML-M3, a specific subtype of AML associated with promyelocytic leukemia. Although this clinical trial has been completed, no data are currently available (Table 1).
Interfering with IL-1 production
Liu et al. investigated the molecular mechanisms underlying the production of IL-1, specifically focusing on the role of the AIM2 inflammasome and the α1-AR in macrophages following CAR T-cell therapy. The study demonstrated that the activation of AIM2 inflammasome, facilitated by α1-AR-mediated signaling and the presence of tumor DNA, leads to the production of bioactive IL-1β. Moreover, interactions among macrophages, CAR T cells, and tumor cells induced a shift in the macrophage phenotype, which diminished the effectiveness of CAR T cells and T cell proliferation by upregulating the expression of immune inhibitors such as PD-L1 and IDO. These effects may be reversed by inhibiting AIM2 or α1-AR, indicating possible strategies to reduce IL-1β-related toxicities and enhance the efficacy of CAR T-cell treatment^[^^64^^]^ (Fig. 3).
Potential benefits of IL-1 blockade and challenges
In extreme situations, IL-1 blocking strategies may significantly reduce the frequency and severity of CRS, thereby decreasing the need for immediate medical intervention. Furthermore, IL-1 inhibition may mitigate the likelihood and severity of neurotoxicity associated with CAR T-cell treatment. By blocking a major inflammatory pathway linked to neurotoxicity, these strategies could lead to improved neurological outcomes and reduce the need for aggressive treatments^[^^10^^,^^11^^]^. However, these approaches may prevent the ability of CAR T cells to identify and eradicate cancer cells by specifically triggering anti-inflammatory responses. Therefore, determining the optimal timing and dosage of IL-1 blockade can be challenging. The preemptive administration of medication must be carefully calibrated to ensure that it does not compromise the CAR T cell-mediated immune response, and early intervention is essential to prevent severe inflammatory reactions^[^^30^^]^. Clinical studies are vital for developing effective timing and dosage regimens. Patients exhibit considerable variability in their responses to CAR T-cell therapy due to several factors, including disease severity, prior medical interventions, and individual immune system characteristics^[26]^. This variation highlights the necessity for an individualized treatment plan, complicating the standardization of IL-1 blocking procedures. Although the main objective is to reduce side effects without compromising the anticancer efficacy of CAR T cells, there is a possibility that IL-1 inhibition may change other aspects of the immune response. Such modifications could impact the longevity and long-term effectiveness of CAR T-cell therapy. Moreover, incorporating IL-1 inhibition into CAR T-cell therapy protocols may complicate and increase the cost of treatment^[41]^. To ensure the practicality and accessibility of this approach for patients, it is essential to assess its logistical consequences and cost-effectiveness. Implementing IL-1 blocking strategies also demands close monitoring of patients to identify any possible adverse effects and evaluate the treatment efficacy. Consequently, patient management and follow-up care become more challenging due to the additional monitoring requirements. While IL-1 can enhance CAR T-cell activation and proliferation, it also contributes to the immunosuppressive characteristics of the TME, thereby inhibiting CAR T-cell function. IL-1 promotes the production of extracellular matrix components, leading to a dense stroma that impedes CAR T-cell infiltration into solid tumors. Additionally, IL-1 facilitates the recruitment and activation of regulatory T cells, myeloid-derived suppressor cells, and tumor-associated macrophages within the TME. These cells secrete inhibitory cytokines such as transforming growth factor-β and IL-10, which suppress the activity of CAR T cells. Furthermore, IL-1 contributes to the establishment of hypoxic and nutrient-deprived conditions in the TME, further limiting CAR T-cell function and persistence. Moreover, IL-1 upregulates the expression of checkpoint ligands, such as programmed death-ligand 1, on tumor cells, which inhibit CAR T-cell activity through receptor engagement. Several strategies are under investigation to mitigate the inhibitory effects of IL-1 within the TME and enhance the efficacy of CAR T cells. These include IL-1 blockade, engineering CAR T cells to resist IL-1-mediated suppression, combination therapies, and localized delivery of IL-1 inhibitors. Addressing IL-1-mediated inhibition within the TME is crucial for enhancing the effectiveness of CAR T-cell therapy against solid tumors. Ongoing research into these strategies aims to improve patient outcomes by overcoming the suppressive nature of the TME^[^^65^^]^.
CONCLUSION
The dual role of IL-1 in CAR T-cell therapy highlights its significance in enhancing therapeutic efficacy and contributing to severe side effects such as CRS and ICANS. IL-1 is pivotal in the initiation and progression of CRS and ICANS, orchestrating the inflammatory response characteristic of both conditions. This cytokine not only increases the immune responses required for CAR T cells to exhibit anti-tumor activity but also triggers a cascade of pro-inflammatory processes that leads to severe neurological and systemic symptoms. One possible strategy to lessen these side effects while maintaining the antitumor efficacy of CAR T-cell treatment is the inhibition of IL-1. The IL-1Ra, anakinra, has shown considerable promise in reducing the severity of CRS and ICANS. Clinical studies have shown that IL-1 inhibition can diminish inflammation, lower cytokine levels, and enhance patient outcomes without compromising the therapeutic benefits of CAR T cells. Early intervention with IL-1 blocking agents may provide a crucial opportunity to prevent serious side effects and improve the safety profile of CAR T-cell treatments. The evidence strongly supports IL-1 blockade as an effective management strategy for CRS and ICANS. Anakinra, in particular, has been shown to have a major impact on the effectiveness of CAR T-cell treatment by reducing life-threatening complications and enhancing patient’s quality of life. The timing of administration is crucial. To stop the progression of CRS and ICANS, early identification of the increased IL-1 level following CAR T-cell infusion may facilitate the prompt administration of IL-1 inhibitors. This strategy not only addresses short-term inflammatory issues for patients undergoing CAR T-cell therapy but also enhances long-term effectiveness and survival rates. Hence, it is strongly recommended that CAR T-cell treatment procedures incorporate IL-1 blocking strategies. By lessening the severity of CRS and ICANS, this strategy has the potential to significantly improve patient outcomes while maximizing the therapeutic advantages of CAR T cells and minimizing the associated adverse effects. To refine these strategies, it is essential to determine the optimal timing and dosage, as well as to validate the long-term benefits of IL-1 blockade in CAR T-cell treatment, though further investigation and clinical studies are required. For patients at high risk of CRS or ICANS, IL-1 blockade offers a targeted strategy to mitigate these toxicities. For those identified as high-risk, targeted IL-1 inhibition could significantly reduce the incidence and severity of these life-threatening complications, improving patient safety and treatment outcomes. However, it is crucial to determine the optimal dosing and timing of IL-1 blockade to avoid compromising the antitumor efficacy of CAR T cells. Further research is needed to balance effective toxicity management with sustained therapeutic activity, ensuring that interventions can be tailored to the individual patient profile and clinical scenario. Likewise, further research is warranted to establish biomarkers that predict IL-1 response and assess the impact of IL-1 blockade across different CAR T-cell types, particularly in the treatment of solid tumor.
Systematic review flowchart of this study.
Role of IL-1 in the pathophysiology of CRS and ICANS associated with CAR T-cell therapy. Upon CAR T-cell activation, IL-1 is released by various immune cells, including macrophages and monocytes. This release initiates a cascade of pro-inflammatory cytokines, notably IL-6, which amplifies the systemic inflammatory response, characteristic of CRS. In the context of ICANS, IL-1 contributes to endothelial activation and blood-brain barrier disruption, facilitating neurotoxic effects. Understanding the signaling pathways of IL-1 and its downstream effects is crucial for developing targeted interventions to mitigate these toxicities without compromising the therapeutic efficacy of CAR T-cell treatments.
Overview of IL-1 blockade strategy in CAR T-cell therapy. These strategies include IL-1Ra antagonists, anti-IL-1 mAbs, IL-1RAPs, and molecules interfering with IL-1 production.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Vanegas YM Mohty R Gadd ME Luo Y Aljurf M Qin HCAR-T cell therapies for B-cell lymphoid malignancies: identifying targets beyond CD 19 Hematol Oncol Stem Cell Ther 202215381933653790610.56875/2589-0646.1026 · doi ↗ · pubmed ↗
- 2Sharifzadeh Z Rahbarizadeh F Shokrgozar MA Ahmadvand D Mahboudi F Jamnani FR Genetically engineered T cells bearing chimeric nanoconstructed receptors harboring TAG-72-specific camelid single domain antibodies as targeting agents Cancer Lett 20133342237442290250710.1016/j.canlet.2012.08.010 · doi ↗ · pubmed ↗
- 3Azad M Bakhshi Biniaz R Goudarzi M Mobarra N Alizadeh Sh Nasiri H Short view of leukemia diagnosis and treatment in iran Int J Hematol Oncol Stem Cell Res 201592889425922649 PMC 4410294 · pubmed ↗
- 4Maali Ah Maroufi F Sadeghi F Atashi A Kouchaki R Moghadami M Induced pluripotent stem cell technology: trends in molecular biology, from genetics to epigenetics Epigenomics 2021138631473382361410.2217/epi-2020-0409 · doi ↗ · pubmed ↗
- 5Maali Ah Gholizadeh M Feghhi-Najafabadi S Noei A Seyed-Motahari SS Mansoori Sh Nanobodies in cell-mediated immunotherapy: On the road to fight cancer Front Immunol 20231410128413676175110.3389/fimmu.2023.1012841 PMC 9905824 · doi ↗ · pubmed ↗
- 6Hajari Taheri F Hassani M Sharifzadeh Z Behdani M Arashkia A Abolhassani MT cell engineered with a novel nanobody-based chimeric antigen receptor against VEGFR 2 as a candidate for tumor immunotherapy IUBMB Life 20197191259673072445210.1002/iub.2019 · doi ↗ · pubmed ↗
- 7Sahmani M Vatanmakanian M Goudarzi M Mobarra N Azad M Microchips and their significance in isolation of circulating tumor cells and monitoring of cancers Asian Pac J Cancer Prev 2016173879942703971410.7314/apjcp.2016.17.3.879 · doi ↗ · pubmed ↗
- 8Gumber D Wang LD Improving CAR-T immunotherapy: Overcoming the challenges of T cell exhaustion E Bio Medicine 2022771039413530117910.1016/j.ebiom.2022.103941 PMC 8927848 · doi ↗ · pubmed ↗