The Impact of Vitamin D Deficiency on Coronary Artery Disease Severity Based on Myocardial Perfusion Imaging: A Cross-Sectional Study
Mahdi Haghighatafshar, Behnaz Shekasteband, Tahereh Firuzyar, Zahra Etemadi, Farinaz Farhoudi, Mesbah Shams

TL;DR
This study found that very low vitamin D levels are linked to severe heart artery disease based on heart imaging results.
Contribution
The study identifies a specific vitamin D threshold (<10 ng/mL) associated with severe coronary ischemia using myocardial perfusion imaging.
Findings
Vitamin D levels below 10 ng/mL were significantly associated with severe ischemia (SSS>13).
Higher Estimated Summed Stress Scores were observed in patients with Vit D levels <10 ng/mL.
Abstract
The impact of low levels of vitamin D (Vit D) on the severity of cardiovascular diseases has become a significant challenge. This study aimed to assess this impact. This pilot cross-sectional study enrolled two hundred patients referred to Namazi Hospital, Shiraz, Iran for myocardial perfusion imaging in 2019. The assessment included myocardial perfusion imaging and Vit D level evaluation. Quantitative ischemia analysis utilized Estimated Summed Stress Scores (SSS), Summed Rest Scores (SRS), and Summed Difference Scores (SDS). Myocardial Perfusion Imaging (MPI) results were categorized into normal, mild ischemia, moderate ischemia, and severe ischemia based on estimated SSS. Ischemia severity was aligned with established criteria, designating severe quantitative ischemia as SSS>13. Vit D was categorized using cutoffs at 10, 20, and 30 ng/mL. Mann–Whitney U-test was used for…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
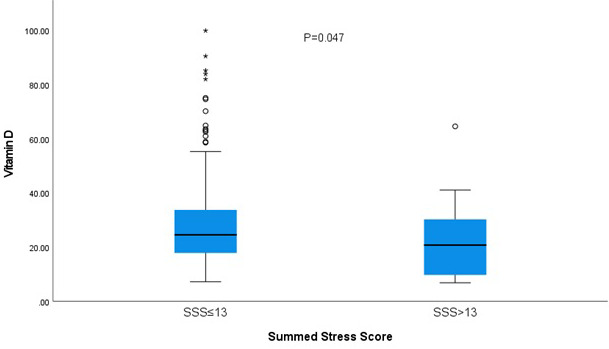 Figure 1
Figure 1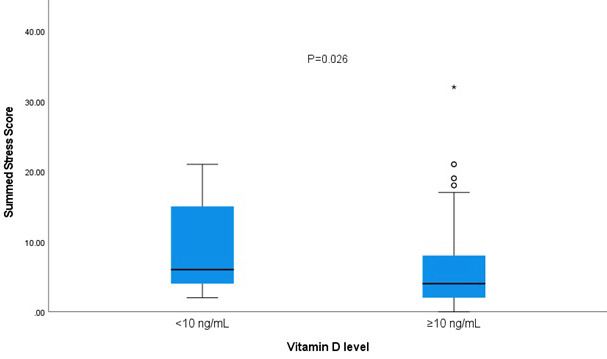 Figure 2
Figure 2| Baseline variables | Patients | |
|---|---|---|
| N=200 | ||
| Age (years), mean±SD | 59.30±11.07 | |
| Sex, n (%) | Female | 90 (45) |
| Male | 110 (55) | |
| Vit D level (mean±SD) | 28.46±17.35 | |
| Categorized Vit D level, n (%) | <20 | 69 (34.5) |
| 20-29 | 56 (28) | |
| >29 | 75 (37.5) | |
| SSS (mean±SD) | 5.78±5.15 | |
| SRS (mean±SD) | 2.19±3.43 | |
| SDS (mean±SD) | 3.59±3.58 | |
| MPI result, n (%) | Normal | 86 (43) |
| Mild ischemia | 69 (34.5) | |
| Moderate ischemia | 27 (13.5) | |
| Severe ischemia | 18 (9) | |
| Baseline variables | Patients with SSS≤13 | Patients with SSS>13 | P value | |
|---|---|---|---|---|
| N=182 | N=18 | |||
| Age (years), mean±SD | 58.65±10.75 | 65.83±12.48 | 0.018 | |
| Sex, n (%) | Female | 83 (45.6) | 7 (38.9) | 0.76 |
| Male | 99 (54.4) | 11 (61.1) | ||
| Vit D level (mean±SD) | 29.11±17.48 | 21.88±14.83 | 0.047 | |
| Categorized Vit D level, n (%) | <10 ng/mL | 9 (4.9) | 6 (33.3) | <0.001 |
| ≥10 ng/mL | 173 (95.1) | 12 (66.7) | ||
| SRS (mean±SD) | 1.60±1.96 | 8.11±7.51 | <0.001 | |
| SDS (mean±SD) | 2.95±2.56 | 10.11±5.60 | <0.001 | |
| MPI indices | Patients with Vit D level<10 ng/mL | Patients with Vit D level≥10 ng/mL | P value |
|---|---|---|---|
| (severe deficiency) N=15 | N=185 | ||
| SRS (mean±SD) | 4.13±5.55 | 2.03±3.18 | 0.084 |
| SDS (mean±SD) | 5.33±4.93 | 3.45±3.43 | 0.1 |
| SSS (mean±SD) | 9.46±6.90 | 5.48±4.88 | 0.026 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsVitamin D Research Studies · Cardiovascular Disease and Adiposity
What’s Known
- Vitamin D deficiency’s association with cardiovascular diseases is still challenging.
What’s New
- According to the results of the current study, severe vitamin D deficiency (below 10 ng/mL) is associated with severe myocardial ischemia.
Introduction
Coronary artery disease (CAD) is the main culprit of sudden cardiac death. The global prevalence of CAD ranges from 5-8%, imposing a significant socioeconomic burden. ^ 1 ^ Hypertension (HTN) and diabetes are among the main cardiovascular disease (CVD) risk factors with a high prevalence worldwide. ^ 2 ^ Hyperlipidemia is highly prevalent and has been shown as a strong risk factor for cardiovascular disease. ^ 3 ^
The prevalence of vitamin D (Vit D) deficiency varies worldwide with the highest prevalence reaching 80%. ^ 4 ^ The phenomenon of hypovitaminosis D, in addition to its negative effect on skeletal development and calcium homeostasis, has been associated with a wide range of diseases, including cancers, certain cardiometabolic risk factors, ^ 5 , 6 ^ diabetes, ^ 7 ^ HTN, and CVD in observational studies. ^ 8 , 9 ^ Vit D deficiency may impact cardiovascular mortality and morbidity through several mechanisms. It is linked to endothelial dysfunction, which can result in atherosclerosis and vascular stiffness. On the other hand, Vit D has a beneficial effect on platelet function in acute coronary syndrome. ^ 10 ^ Due to the expression of Vit D receptors in cardiomyocytes, vascular smooth muscle, and the endothelium, the suggested direct mechanisms of coronary atherosclerosis include the enhancement of endothelial cell-dependent vasodilation, the inhibition of vascular smooth muscle proliferation, and the promotion of vascular calcification processes. ^ 11 ^
There are different modalities to assess cardiovascular status including angiography, computed tomography angiography, and Myocardial perfusion imaging (MPI). MPI with Tc-99m sestamibi (^99m^Tc-MIBI) is a non-invasive imaging method that plays a major role in the diagnosis, therapy guidance, and prognosis determination of patients with CAD. ^ 12 ^
As Vit D deficiency is easily preventable, according to the hypothetic role of Vit D deficiency in the development of CAD and cardiovascular health, and the inconsistency of the results of different studies, this study aimed to investigate the association of Vit D deficiency on perfusion/function of the left ventricle in myocardial perfusion Single Photon Emission Computed Tomography (SPECT) imaging.
Patients and Methods
Patient Selection and Sample Collection
Two hundred patients with clinical suspicion of CAD who were 30 years old and above and were referred to Namazi Hospital’s nuclear medicine department for SPECT MPI, were prospectively enrolled in this pilot cross-sectional study from May 2019 to September 2019. Exclusion criteria included neoplastic and paraneoplastic diseases, renal or liver dysfunction, and a history of primary hyperparathyroidism, sarcoidosis, or tuberculosis. Routine blood sampling measured serum Vit D (25-OHD) levels using High-Performance Liquid Chromatography at the Endocrine and Metabolism Research Center of Shiraz University of Medical Sciences.
The study was approved by the Ethics Committee (IR.SUMS.MED.REC.1398.125) of Shiraz University of Medical Sciences. Written informed consent was obtained from all patients enrolled in the study.
Myocardial Perfusion Image Acquisition
A two-day rest-stress protocol involving exercise or dipyridamole was employed, injecting 20 mCi of 99mTc-MIBI (Parsisotope, Iran). SPECT emission data, acquired by a dual-head γ-camera (GE Infinia, USA) covering a 180ᵒ arc in 32 steps, were reconstructed using the ordered-subset expectation maximization (OSEM) algorithm in a 64*64 matrix.
MPI Parameters
Quantitative assessment of left ventricular perfusion utilized QPS software (Cedar-Sinai, USA), evaluating Summed Stress Scores (SSS), Summed Rest Score (SRS), and Summed Difference Score (SDS). Categorized from 0 to 4 based on 20-segment polar maps, MPI images were classified as normal (SSS<4), mild (SSS=4-8), moderate (SSS=9-13), and severe (SSS>13) ischemia. ^ 13 ^
Vit D Level Categorization
Vit D deficiency (<20 ng/mL) and insufficiency (20-29 ng/mL) followed the US Endocrine Society guideline. ^ 14 ^ Severe deficiency was defined as <10 ng/mL based on previous studies. ^ 15 ^
Statistical Analysis
SPSS software version 26 (IBM Corp., USA) was used for conducting data analysis, presenting continuous variables as descriptive statistics) Mean±SD (and categorical variables as frequency percentages. Nonparametric tests were applied due to non-normal distribution. Spearman rho correlation, Mann-Whitney U test, and Chi Square test were employed to assess the association between MPI variables, Vit D levels, and categories of ischemia. A P value less than 0.05 was considered as significant.
Results
In this investigation encompassing 200 participants, comprising 90 women and 110 men, the mean age of the participants was 59.30±11.07 years (range: 30-92). The average Vit D level was 28.46±17.35 ng/mL (range: 6.8-99.8 ng/mL). Notably, Vit D deficiency manifested in 69 patients, with 15 exhibiting severe deficiency. Abnormal MPI findings were identified in 57% of the patients. Comprehensive demographic, clinical, and MPI parameters are meticulously detailed in table 1.
When comparing mean Vit D levels between patients with normal and abnormal MPI (30.44±18.66 vs. 26.97±16.21, respectively), no statistically significant difference emerged (P=0.237). Furthermore, there was no significant association between abnormal MPI and Vit D categorizations using cutoffs at 10, 20, and 30 ng/mL (P=0.184, P=0.422, P=0.417, respectively).
Table 2 provides an overview of patient characteristics based on SSS categorization. Those with severe ischemia (SSS>13) exhibited significantly higher age (P=0.018), SRS (P<0.001), and SDS (P<0.001). Notably, the Vit D level was significantly lower in this group (P=0.047) (figure 1). Chi Square test established a significant association between severe Vit D deficiency and severe ischemia (P<0.001).
The simple box plot shows Vit D level in patients with categorized Summed Stress Score.
Spearman rho correlation analysis demonstrated a significant correlation between Vit D levels and SSS and SRS (P=0.026, r=-0.157; P=0.028, r=-0.155, respectively), but there was no significant correlation between Vit D levels and SDS (P=0.170, r=-0.097). Further insights into the association between categorized Vit D levels and MPI parameters are elucidated in table 3. SSS was significantly elevated in patients with severe Vit D deficiency (P=0.026) (figure 2).
The simple box plot shows Summed Stress Score levels in patients with categorized Vit D levels.
HTN, diabetes, obesity, hyperlipidemia, and smoking did not present a significant association with severe Vit D deficiency (P=0.19, P=0.92, P=0.43, P=0.43, P=0.84, respectively).
Discussion
In our study, we found no significant association between Vit D levels and the prevalence of CAD. However, there was a significant association between lower Vit D levels and severe ischemia (SSS>13). Additionally, severe Vit D deficiency (<10 ng/mL) was associated with increased CAD severity. Although a few clinical studies on the association of Vit D and coronary atherosclerosis and CAD via imaging techniques have been performed, the results of these studies have been controversial. Moradi and others performed a cohort study in a group of 180 Iranian patients to assess the effect of Vit D levels on coronary artery computed tomography angiography (CTA). Their study showed that coronary artery calcium score and Vit D level were inversely related. Nevertheless, there were some limitations, such as heterogeneity of groups in terms of cardiovascular risk factors and incomplete collection of all risk factors. ^ 16 ^ Verdoia and others performed a cross-sectional study in a sample of 1484 patients undergoing coronary angiography in Italy. Vit D deficiency, especially severe Vit D deficiency, was related to a higher prevalence of CAD and CAD severity. ^ 15 ^ Alsancak and others conducted a cross-sectional study including 746 patients who underwent coronary angiography. They divided patients into two groups: Vit D<20 ng/mL (n=602) and Vit D20 ng/mL (n=144). There was no significant difference in Gensini scores (severity of CAD) between the two groups. ^ 17 ^ In another cross-sectional study that was performed by Dhibar and others in a group of 315 Indian patients, Vit D deficiency was prevalent among CAD patients, but there was no association between the deficiency and the angiographic severity of CAD according to the stenosis percentage, in addition to the number of involved vessels. ^ 18 ^ In a stronger study with 1131 patients, authors showed that Vit D levels and coronary artery calcium score had no association with CAD severity. However, the low number of obstructive diseases (>70% stenosis) in CTA was expressed as its limitation in obtaining adequate statistical power. ^ 19 ^ Batsi and others assessed the association of Vit D level with the prevalence of myocardial ischemia during a cross-sectional study in 113 patients undergoing SPECT MPI. The results of their study showed that the prevalence of ischemia was significantly higher in patients with lower Vit D levels. There was also a negative association between Vit D level and SSS and SRS. ^ 13 ^ Manson and others conducted a randomized placebo-controlled clinical trial in the US including 25871 patients with about 5 years of follow-up. Patients in the intervention group were given a daily dose of 2000 IU of Vitamin D and 1 g of omega-3 fatty acids to help prevent cancer and cardiovascular disease in men aged 50 and above and women aged 55 and above. There was no significant difference between the incidence of invasive cancer or cardiovascular events in the Vit D and placebo groups. ^ 20 ^ Scragg and others performed a randomized placebo-controlled clinical trial in New Zealand including 5108 patients with about 4 years of follow-up. Patients in the intervention group were supplemented with 100000 IU Vit D monthly. High-dose Vit D supplementation did not reduce cardiovascular disease incidence. ^ 21 ^ In a systematic review and meta-analysis by Barbarawi and others, 21 clinical trials were included. The clinical trials assessed the effect of more than one year of Vit D supplementation on the incidence of CAD and all-cause mortality. There was no significant effect on any of the mentioned outcomes. ^ 22 ^ Kahwati and others performed a systematic review and meta-analysis on randomized controlled trials about Vit D supplementation. Among community-based studies, although treatment reduced mortality, the result was not statistically significant. For assessing the effect of treatment with Vit D only two trials including patients with low Vit D levels were evaluated. There was no significant effect on the incidence of cardiovascular events. ^ 23 ^
The controversy between different observational studies, and also between observational and trial studies, might be due to the difference in Vit D cutoffs. Another reason might be that not all clinical trials have assessed the effect of Vit D supplementation regarding the basal Vit D status. Additionally, most studies have assessed its effect on the incidence of CAD and not the CAD severity. Another point might be that they had not assessed the effect of severe Vit D deficiency on the incidence and severity of CAD. An additional probable reason may be the reverse causation. The most common cause of Vit D is lack of exposure to sunlight. Lack of exposure to sunlight may be due to physical inactivity, a sedentary lifestyle, incapacitation, and so on. ^ 24 ^ Physical inactivity is also associated with obesity, HTN, diabetes, and other CVD risk factors. ^ 25 ^ Therefore, a higher prevalence of CAD among patients with Vit D deficiency may simply be due to confounding co-morbidities rather than a cause-and-effect relationship between Vit D and CAD. It is plausible that patients with CVD do not get enough sun exposure due to physical inactivity, which causes Vit D deficiency. In other words, CVD caused Vit D deficiency, not Vit D deficiency caused CVD. Limitations of our study include its cross-sectional design, a relatively small sample size, and a lack of assessment of seasonal changes in Vit D levels.
Conclusion
Our study suggests an association between severe Vit D deficiency and severe myocardial ischemia (SSS>13) and non-categorized SSS levels. Further research with larger samples and comprehensive assessments is needed to elucidate the intricate association between Vit D, CAD, and its severity.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Bauersachs R Zeymer U Briere JB Marre C Bowrin K Huelsebeck M Burden of Coronary Artery Disease and Peripheral Artery Disease: A Literature Review Cardiovasc Ther 201920198295054[ PMC Free Article ]10.1155/2019/829505432099582 PMC 7024142 · doi ↗ · pubmed ↗
- 2Nowbar AN Gitto M Howard JP Francis DP Al-Lamee R Mortality From Ischemic Heart Disease Circ Cardiovasc Qual Outcomes 201912 e 005375[ PMC Free Article ]10.1161/CIRCOUTCOMES.118.00537531163980 PMC 6613716 · doi ↗ · pubmed ↗
- 3Karr S Epidemiology and management of hyperlipidemia Am J Manag Care 201723 S 139S 4828978219 · pubmed ↗
- 4Chen KW Chen CW Yuan KC Wang IT Hung FM Wang A Yetal Prevalence of Vitamin D Deficiency and Associated Factors in Critically Ill Patients: A Multicenter Observational Study Front Nutr 20218768804[ PMC Free Article ]10.3389/fnut.2021.76880434966771 PMC 8710763 · doi ↗ · pubmed ↗
- 5Queiroz DJM Silva AS Diniz ADS Carvalho AT Araujo E Neves JP Retal Vitamin D insufficiency/deficiency and its association with cardiometabolic risk factors in Brazilian adolescents Nutr Hosp 201936142810.20960/nh.188430836756 · doi ↗ · pubmed ↗
- 6Rojas LZ Quintero-Lesmes DC Gamboa-Delgado EM Guio E Serrano NC Prevalence of vitamin D status and its association with overweight or obesity in a population of Colombian children and adolescents J Nutr Sci 20209 e 55[ PMC Free Article ]10.1017/jns.2020.4733354326 PMC 7737171 · doi ↗ · pubmed ↗
- 7Berridge MJ Vitamin D deficiency and diabetes Biochem J 201747413213210.1042/BCJ 2017004228341729 · doi ↗ · pubmed ↗
- 8Roy A Lakshmy R Tarik M Tandon N Reddy KS Prabhakaran D Independent association of severe vitamin D deficiency as a risk of acute myocardial infarction in Indians Indian Heart J 2015672732[ PMC Free Article ]10.1016/j.ihj.2015.02.00225820047 PMC 4382524 · doi ↗ · pubmed ↗