Characteristics of people with bipolar disorder I with and without auditory verbal hallucinations
Aster Javier, Natalia Jaworska, Jess Fiedorowicz, Vincent Magnotta, Jenny G. Richards, Ercole John Barsotti, John A. Wemmie

TL;DR
People with bipolar disorder I who experience auditory hallucinations have more severe symptoms and face greater socioeconomic challenges.
Contribution
This study is one of the first to explore the impact of auditory verbal hallucinations in bipolar disorder I.
Findings
Individuals with AVHs had higher manic and positive symptom scores.
Those with AVHs reported lower socioeconomic status and higher unemployment rates.
The presence of AVHs may indicate more severe illness and long-term hardship.
Abstract
Approximately half of people with bipolar disorder type I (BD-I) report the presence of psychotic symptoms at least at some point during their illness. Previous data suggest that more than 20% of people with BD-I report the presence of auditory verbal hallucinations (AVHs), or “voice-hearing” in particular. While work in other disorders with psychotic features (e.g., schizophrenia) indicates that the presence vs. absence of AVHs is associated with poorer clinical outcomes, little is known about their effects on clinical and socioeconomic features in BD-I. We investigated whether people with BD-I (N = 119) with AVHs (n = 36) and without AVHs (n = 83) in their lifetime differ in terms of demographic features and clinical measures. Relations with AVHs and other positive symptoms were explored. People with BD-I and AVHs vs. without AVHs had higher manic and positive symptom scores (i.e.,…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
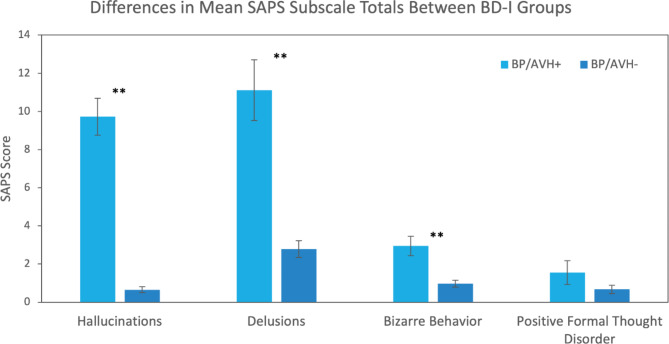 Figure 1
Figure 1- —http://dx.doi.org/10.13039/100000025National Institute of Mental Health
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsBipolar Disorder and Treatment · Schizophrenia research and treatment · Electroconvulsive Therapy Studies
Background
Bipolar disorder type I (BD-I) is a debilitating mood disorder characterized by episodes of mania (i.e., periods of abnormally elevated and irritable mood) and depression. However, psychotic symptoms, such as hallucinations and delusions, can also occur in BD-I, with at least one lifetime occurrence being reported in up to 57–70% of people with BD-I (Aminoff et al. 2022; Upthegrove et al. 2015). Studies have shown that a history of psychotic symptoms in BD-I is associated with increased cognitive and functional impairment, as well as a greater number of hospitalizations (Glahn et al. 2007; Levy et al. 2013; Simonsen et al. 2011; Strakowski et al. 2000).
Though generally understudied in the context of BD, previous work indicates that approximately 20% of people with BD-I report experiencing auditory verbal hallucinations (AVH), one of the most common types of hallucinations, at least once during their illness course (Morgan et al. 2005; Toh et al. 2015). AVHs can occur in any state of BD-I, but have been found to be more present during manic and mixed-manic episodes (Smith et al. 2017). Work in other disorders with psychotic features, such as schizophrenia, indicates that AVHs are associated with poorer clinical outcomes, as well as greater cognitive and functional impairments (Hugdahl et al. 2013; Jenkins et al. 2018; Kelleher et al. 2013; Toh et al. 2015). Studies in people with schizophrenia have also reported that AVHs correlated with increased severity of other hallucination types; this might contribute to functional impairment (Eve Lewandowski et al. 2009; Mueser et al. 1990). AVHs in people with BD-I have been associated with reduced illness insigh; that is, decreased awareness of symptoms, openness to feedback about illness, and self-reflectiveness (Baethge et al., 2005; Kumari et al. 2013). Decreased insight has been linked with medication non-adherence, reduced cognitive performance, and daily and occupational functioning impairments (Sajatovic et al. 2011; Wels et al. 2023). Conversely, increased illness insight has been linked with better coping and adaptation in BD-I patients (Tohumcu and Çuhadar 2024). Compared to people with schizophrenia, the impact of AVHs in the context of BD-I in terms of sociodemographic features and clinical profiles has been unexplored. Such insight might be important in laying the groundwork for more tailored and ultimately more effective treatment approaches for distinct subgroups of people with BD-I.
This study aimed to assess whether BD-I patients with vs. without a history of AVH differ in terms of demographic (i.e., age, assigned sex at birth, race, ethnicity) and clinical features (e.g., depressive, manic, and positive symptoms). Most novel, we also assessed occupational and daily functioning, operationalized by years of education, subjective socioeconomic status (SES), employment/disability/student status, and housing situation to assess the influence of AVH presence in people with BD. We expected that patients with AVHs would exhibit more pronounced indications of functional impairments, such as increased unemployment and disability status, and lower levels of education and subjective SES. We also explored if AVH severity was related to the severity of other hallucination types in people with BD-I and AVHs. Though this has been studied in schizophrenia, positive symptoms do not present the same way in BD-I (Baethge et al., 2005; Mancuso et al. 2015), as such, exploring such relations in people with BD-I addresses this research gap.
Methods
Participants
A total of N = 119 people with BD-I, aged 18–68 years (39.3, S.D.=13.5), were recruited as part of the Bipolar Disorder Research Program of Excellence at the University of Iowa; participants were either outpatients affiliated with the University Health Centre or recruited from the community. To ensure eligibility and confirm diagnosis, research personnel administered the Structured Clinical Interview for DSM-5 (SCID-5) (First et al. 2015), followed by an unstructured clinical interview by a psychiatrist. The majority (64.7%; N = 77) were female sex assigned at birth. Participants were divided into two groups based on the first item of the Scale for the Assessment of Positive Symptoms (SAPS) (Andreasen 1984): those who experienced AVH in their lifetime (BP/AVH+, SAPS score ≥ 1; N = 36) and those who did not (BP/AVH-, SAPS score = 0; N = 83). Group (i.e., BP/AVH + vs. BP/AVH-) features are presented in Table 1.
Measures
The SAPS is a 34-item scale that measures positive psychotic symptoms (Andreasen 1984). It is divided into 4 subscales measuring hallucinations (items 1–6), delusions (8–19), bizarre behavior (21–24), and positive formal thought disorder (26–33). Each item is rated from 0 (absent) to 5 (severe). There are also global items (self-reported overall ratings for each subscale), but these were not included in the total/composite SAPS score or any subscale totals. Reliability tests showed excellent internal consistency of the overall SAPS scale (Cronbach’s alpha = 0.91) in our sample (N = 119).
The Montgomery Åsberg Depression Rating Scale (MADRS) is a 10-item scale that measures the presence of depression symptoms in the last week (Davidson et al. 1986). Each item is rated from 0 (none) to 6 (severe). Reliability tests showed good internal consistency (Cronbach’s alpha = 0.83) in our sample (N = 119).
The Young Mania Rating Scale (YMRS) is an 11-item scale that measures the presence of manic symptoms in the past 48 h (Young et al. 1978). Items 1–5, 7, 10, 11 are rated from 0 (none) to 4 (severe), while items 6, 8, 9 are rated 0 (none) to 8 (severe). Reliability tests showed acceptable internal consistency (Cronbach’s alpha = 0.78) in our sample (N = 119).
Subjective SES was obtained using a “ladder rung” item that asked participants to select where they believe they rank socioeconomically (Adler and Stewart 2007). The bottom rung corresponds to a score of 1 (lowest SES), while the highest rung corresponds to a score of 10 (highest SES).
Retrospective symptom burden for each participant was estimated by percentage of time (self-reported) spent in depressed, manic, and euthymic mood states over the past decade (maximum 100%).
Statistics
Statistical analyses were performed using SPSS for Mac v. 28.0 (SPSS, Chicago, Illinois, USA); significance levels were p = 0.05, unless stated otherwise. A two-tailed student t-test was run to compare groups (i.e., BP/AVH + vs. BP/AVH-) on age. One-sided t-tests were applied for total years of education and subjective SES as the AVH group was expected to report lower levels. Two-sided Pearson Chi Square statistics were used to compare groups on housing (homeless/shelter, living with family, owns a house, or renting an apartment/dormitory), assigned sex at birth, race, and ethnicity. To further explore our directional hypothesis (AVH group would exhibit more functional impairments), a Fisher’s exact test (one-sided) was used to compare groups on disability status (persons with or without disabilities), employment (full/part time employment or unemployed), and student status (enrolled in school or not).
Separate one-way analyses of variance (ANOVAs) were used to compare groups on SAPS, MADRS, and YMRS total scores. A multivariate ANOVA (MANOVA) was also used to compare groups on the four SAPS subscales. For the AVH group, exploratory Pearson’s correlations (with bias-corrected and accelerated bootstrapping) were performed to examine relations between the SAPS AVH item and each of the following SAPS items: tactile/somatosensory hallucinations, visual, and olfactory hallucinations. Finally, Mann-Whitney U tests were performed to compare the two groups on the self-reported and retrospectively estimated percentage of time spent in depressed, manic, and euthymic mood states over the past decade.
Results
Demographics
Table 1 displays the means for various demographic factors in the BP/AVH + and BP/AVH- groups. The groups did not differ in terms of age (t(1,117) = 0.66, p = 0.51), assigned sex at birth (χ^2^ = 0.92, p = 0.34), race (χ^2^ = 1.81, p = 0.77), ethnicity (χ^2^ = 4.71, p = 0.09), or housing situation (χ^2^ = 0.85, p = 0.84). The AVH group tended to have fewer years of education than the group without AVHs (t(1,117)=-1.35, p = 0.09). The BP/AVH + group had a lower subjective SES (t(1,116)=-1.58, p = 0.05) and a greater tendency for being unemployed (χ^2^ = 2.87, p = 0.068) compared to the BP/AVH- group. Fisher’s exact tests revealed that the AVH group was not more likely to declare disability status (χ^2^ = 0.76, p = 0.26) or be out of school (χ^2^ = 0.43, p = 0.37) compared to the group without AVHs; the inclusion of total SAPS scores (minus hallucinatory item score) as a covariate on these outcomes is presented in Supplementary Table 1.
Table 1. Demographic factors and clinical scores for people with bipolar disorder type I (BD-I) with (BP/AVH+) and without (BP/AVH-) auditory verbal hallucinations (AVH)ParameterBP/AVH+ (N = 36)BP/AVH- (N = 83)Significance(N = 119)Age (Years)M = 40.6 (SD = 13.5)M = 38.8 (SD = 13.9)t(1,117) = 0.66p = 0.51Total Years of EducationM = 14.5 (SD = 2.0)M = 15.0 (SD = 2.2)t(1,117)=-1.231-tailed p = 0.11Subjective SESM = 4.8 (SD = 2.0)M = 5.4 (1.9)t(1,116)=-1.581-tailed p = 0.05Assigned Sex at BirthFemale = 21 (58.4%)Male = 15 (41.6%)Female = 56 (67.5%)Male = 27 (32.5%)χ^2^ = 0.92p =* 0.34RaceNative American = 0 (0%)Asian = 0 (0%)Black/African American = 2 (5.6%)Multiracial = 1 (2.7%)White = 33 (91.7%)Native American = 2 (2.4%)Asian = 2 (2.4%)Black/African American = 4 (4.8%)Multiracial = 2 (2.4%)White = 73 (88.0%)χ^2^ = 1.81p = 0.77EthnicityHispanic/Latino = 3 (8.3%)Other Ethnicity = 31 (86.1%)Unknown = 2 (5.6%)Hispanic/Latino = 8 (9.6%)Other Ethnicity = 75 (90.4%)Unknown = 0 (0%)χ^2^ = 4.71p = 0.09Housing SituationHomeless/shelter = 1 (2.8%)Living with family = 5 (13.9%)House owner = 14 (38.9%)Renting = 16 (44.4%)Homeless/shelter = 1 (1.2%)Living with family = 15 (18.1%)House owner = 28 (33.7%)Renting = 39 (47.0%)χ^2^ = 0.85p = 0.84Disability StatusDisability = 10 (27.8%)Without disability = 26 (72.2%)Disability = 17 (20.5%)Without disability = 66 (79.5%)χ^2^ = 0.76p = 0.26 (1-sided)Employment StatusEmployed (full/part time) = 17 (47.2%)Unemployed = 19 (52.8%)Employed (full/part time) = 53 (63.9%)Unemployed = 30 (36.1%)χ^2^ = 2.87p = 0.068 (1-sided)Student Status (full/part time)Student = 4 (11.1%)Not in school = 32 (88.9%)Student = 13 (15.7%)Not in school = 70 (84.3%)χ^2^ = 0.43p = 0.37 (1-sided)SAPS totalM = 25.3 (SD = 16.0)M = 5.2 (SD = 6.2)F(1,117) = 98.28p < 0.001MADRS totalM = 14.8 (SD = 7.9)M = 14.0 (SD = 9.7)F(1,117) = 0.16p = 0.69YMRS totalM = 10.1 (SD = 8.6)M = 5.2 (SD = 5.5)F(1,117) = 13.78p < 0.001% time (past decade): DepressedM = 38.8 (SD = 22.9)M = 38.4 (SD = 26.2)Z=-0.20p = 0.84% time (past decade): ManicM = 23.0 (SD = 16.9)M = 16.8 (SD = 16.0)Z=-2.13p = 0.03*% time (past decade): EuthymicM = 38.2 (SD = 26.7)M = 44.9 (SD = 29.8)Z=-1.01p = 0.31**p* ≦ 0.05, **p < 0.001. Note. SES: Socioeconomic Status; SAPS: Scale for the Assessment of Positive Symptoms; MADRS: Montgomery Åsberg Depression Rating Scale; YMRS: Young Mania Rating Scale
Clinical measures
In terms of clinical scales (Table 1), SAPS (F(1,117) = 98.28, p < 0.001, _partial_η^2^ = 0.46) and YMRS (F(1,117) = 13.78, p < 0.001, _partial_η^2^ = 0.11) total scores were elevated in the BP/AVH + vs. BP/AVH- group. However, AVH presence was not found to influence MADRS total scores (F(1,117) = 0.16, p = 0.69, _partial_η^2^ = 0.001; see Supplementary Table 1 for the effect of including total SAPS score [minus hallucinatory item] as a covariate).
A MANOVA for the four SAPS subscales (hallucinations, delusions, bizarre behavior, positive formal thought disorder) was conducted between the groups; the multivariate model was significant (Pillai’s Trace = 0.61, F(4,114) = 47.97, p < 0.001, _partial_η^2^ = 0.63). Follow-up univariate analyses yielded a difference between groups on hallucinations (F(1,117) = 192.44, p < 0.001, _partial_η^2^ = 0.62), delusions (F(1,117) = 43.92, p < 0.001, _partial_η^2^ = 0.27), and bizarre behavior (F(1,117) = 17.64, p < 0.001, _partial_η^2^ = 0.13) subscales (Fig. 1). No group difference existed on the positive formal thought disorder subscale (F(1,117) = 2.10, p = 0.15, _partial_η^2^ = 0.02).
Finally, the BP/AVH + group (M = 23.0%) reported significantly more time spent in manic episodes over the past decade compared to the BP/AVH- group (M = 16.8%) (Z=-2.13, p = 0.03). These differences were not evident for depressed (Z=-0.20, p = 0.84) or euthymic (Z=-1.01, p = 0.31) states.
Fig. 1. Differences Between People with Bipolar Disorder Type I (BD-I) with (BP/AVH+) and without (BP/AVH-) Auditory Verbal Hallucinations (AVH) on the Scale for the Assessment of Positive Symptoms (SAPS) Subscales: Hallucinations, Delusions, Bizarre Behavior, and Positive Formal Thought Disorder. ** p < 0.001
Exploratory correlations
For the BP/AVH + group, there was no significant correlations found between the SAPS AVH and tactile hallucination items (r = 0.004, p = 0.63, 95% BCa CI [-0.40, 0.35]). This was also the case for the correlation between the AVH and the olfactory hallucination (r = 0.07, p = 0.67, 95% BCa CI [-0.26, 0.39]) and visual hallucination items (r = 0.18, p = 0.28, 95% BCa CI [-0.15, 0.48]).
Discussion
This study aimed to compare demographic and clinical characteristics between BD-I people with vs. without AVHs. We expected that the AVH group would exhibit more functional impairments in terms of socioeconomic (e.g., unemployment, disability status) and clinical features. In addition, we sought to examine the relations between the SAPS AVH item and other types of hallucinations for the BP/AVH + group as this has previously been under-explored and would provide some insight into the relations between hallucinatory features.
Our BP/AVH + sample made up 30.3% (n = 36) of the entire cohort (N = 119), which is consistent (though somewhat higher) with past literature that found the proportion of people with BD-I and AVHs was around 20% (Morgan et al. 2005; Toh et al. 2015). While we found that the groups did not differ on most demographic factors, people with BD-I and AVHs reported lower subjective SES and a tendency for lower employment rates compared to those without AVHs. The AVH group also had elevated positive (delusions, bizarre behavior, other kinds of hallucinations) and manic symptoms; no differences in depressive symptoms existed. In addition, the AVH group had higher YMRS scores and retrospectively reported significantly more time spent in manic states over the past decade compared to the non-AVH group. Finally, no correlations were found between the SAPS AVH item and any of the hallucination items for the BP/AVH + group.
People with BD-I and AVHs were found to have lower subjective SES and a tendency for lower employment rates than those without AVHs, which aligns with our hypotheses. However, while we expected the AVH group to exhibit functional impairments as assessed by years of education, disability status, housing situation, and student status, there was no significant difference found between groups. Previous research on people with AVHs (general population and those with schizophrenia only) found several indications of functional impairment in addition to lower SES and unemployment (Kr Akvik et al. 2015; Varese et al. 2011). Others have noted that people with BD and schizophrenia with AVHs vs. without AVHs exhibited greater working memory impairments (Gupta et al. 2018; Jenkins et al. 2018), and abnormalities in neural networks related to attention, emotion processing, speech production/processing, and memory (Kühn and Gallinat 2012; Qiu et al. 2020). By extension, such cognitive and emotional impairments could translate to daily functional impairments. A meta-analysis (Depp et al. 2012) reported significant relations between cognitive abilities (i.e., verbal learning, working and visual learning memory) and daily functioning (measured by clinician and self-report ratings, functional milestones, and performance-based tasks) in BD-I patients. Studies have also reported correlations between cognitive function and social and occupational functioning in both symptomatic and euthymic BD-I patients (Baune and Malhi 2015). Our data suggest functional impairments in people with BD-I and AVHs as operationalized by lower self-reported SES and a tendency for decreased employment rates, speaking perhaps to lower socioeconomic productivity in this cohort. Granted, other positive symptoms/greater illness severity likely accounted for some of this variance (see Supplementary Table 1); larger epidemiological studies are required to home in on the specific contributions of AVHs on clinical and socioeconomic features of this feature in BD.
The AVH group exhibited increased positive symptoms – specifically, hallucinations (AVHs as well as other types), delusions, and bizarre behavior – in comparison to the non-AVH group. These results align with previous research in people with schizophrenia (Chang et al. 2015; Chen et al. 2015; Larøi et al. 2012; Wang et al. 2021) and BD (Smith et al. 2017; Toh et al. 2015). Collectively, this suggests that the presence of AVHs corresponds to the worsening of other psychotic symptoms. Past studies have shown that positive symptoms are correlated with each other; further, greater positive symptoms (especially hallucinations and delusions) predicted higher rates of illness recurrence, relapse, hospital admissions, and suicide attempts in BD (Smith et al. 2017; Wilson and Sponheim 2014), underscoring the need for more proactive and intensive treatment approaches for this population. The only positive symptom that the groups did not significantly differ on was positive formal thought disorder. Past studies have shown that this symptom is more severe in people with schizophrenia compared to people with BD-I (Yalincetin et al. 2017), which could explain our results.
AVH presence was accompanied by elevated manic symptoms, as well as more time spent in manic episodes over the past decade (retrospective, self-report). Several studies have also reported that AVHs were more associated with manic and mixed-manic episodes in people with BD (Baethge et al. 2005b; Smith et al. 2017). This may indicate a connection between the co-occurrence of mania and psychotic features in BD-I. Indeed, significant overlap has been observed between manic and positive symptoms, which corroborates the proposition of psychosis as a spectrum disorder that includes BD-I (Craddock et al. 2009; Dunayevich et al. 2000; Simonsen et al. 2011). These findings suggest that people with BD-I and AVHs (as well as other positive symptoms) experience exacerbated, more chronic manic symptoms, which can lead to lower quality of life and poorer clinical outcomes. This highlights the need for specialized early detection and treatment strategies that address psychosis and mania in concert.
No differences existed between groups on depressive symptom severity. Psychotic features in BD, such as AVHs, can manifest during manic and depressive (and mixed) episodes (Chakrabarti and Singh 2022). Some have reported that AVHs in people with BD-I are less associated with depressive vs. manic episodes, while others report the opposite (Hammersley et al. 2010; Smith et al. 2017; Toh et al. 2015). AVH severity in patients with schizophrenia was associated with more severe depressive symptoms and lower social functioning (Abdelraof et al. 2023; Wang et al. 2019). It is feasible that AVHs have less influence/interaction with depression features and depression severity in BD-I; however, this needs to be assessed with larger samples.
Finally, our exploratory analyses indicated that there were no significant correlations between AVH severity and the severity of other hallucination types for the BP/AVH + group. While there is limited precedent literature on this, our findings are inconsistent with previous work noting correlations between AVHs and other types of hallucinations (visual, tactile/somatosensory, and olfactory) in people with schizophrenia (Eve Lewandowski et al. 2009; Mueser et al. 1990). It is feasible that the relatively modest severity of AVHs in our sample might contribute to the lack of notable relations with other hallucinatory features.
While novel, several limitations of the above work must be acknowledged. First, only a small percentage (~ 11%; n = 13) of the cohort identified as a racial minority, which may impact generalizability. Second, the smaller sample of people with BD-I and AVHs (vs. without) may result in less precise power estimates. Future studies with larger and more diverse samples are warranted to fully investigate the clinical and socioeconomic effects of AVHs in people with BD-I. Further, the retrospective symptom burden data was collected using self-report methods rather than direct measurements; these might be impacted by both recall bias and insight into symptoms, and limits reliability. While only used to supplement findings from clinical rating analyses, we acknowledge this method has not been validated. Nevertheless, the retrospective data on mania corroborate and expand upon the YMRS symptom data by offering a glimpse into long-term manic profiles. Also, we acknowledge that the use of subjective SES might be a limitation. Income was not collected as part of the study, but this measure might not have accurately captured SES in our cohort. This study was conducted in the metro area of Iowa, a university/college town with ~ 30,000–40,000 students (out of a population of ~ 75,000). These students might report a low income because of part-time employment or no employment during school; thus, years of education might better reflect their objective SES. Nevertheless, objective measures of SES should be utilized in future studies.
Finally, after completing data collection and analyses, it was discovered that portion of people with BD and AVH- (N = 30) were asked about their hallucinatory status in the past month (vs. lifetime, as was asked for the remainder of participants [N = 53]). As such, it is feasible that these people were miscoded (i.e., a portion of the N = 30 might have been lifetime hallucinators). To address this possibility, sensitivity analyses were carried out by excluding these N = 30 people from our AVH- group. Our results did not change substantially; the exception was that disability status was no longer significant while SES reached significance (likely due to power issues). This sensitivity analyses, coupled with the fact that the inclusion of the N = 30 people with BD and AVH- in the past month (vs. lifetime) biases analyses to the null hypotheses, and that -based on previous work- only a minority would be miscoded, suggests that our data, as presented, are robust.
In summary, AVHs in people with BD-I were found to be associated with functional impairments manifesting as unemployment and subjective socioeconomic hardship, as well as more severe positive (specifically other types of hallucinations, delusions, and bizarre behavior) and manic symptoms. While this research contributes to the growing body of research characterizing people with BD-I and AVHs, larger-scale studies with more in-depth investigation into demographic, socioeconomic, cognitive, clinical, and neural features are needed. Such insight might inform more tailored treatment approaches for this clinical population, thus improving functional outcomes and quality of life.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Supplementary Material 1
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Adler NE, Stewart J. (2007). The Mac Arthur Scale of Subjective Social Status. Mac Arthur Research Network on SES and Health at UCSF.
- 2Aminoff SR, Onyeka IN, Ødegaard M, Simonsen C, Lagerberg TV, Andreassen OA, Romm KL, Melle I. (2022). Lifetime and point prevalence of psychotic symptoms in adults with bipolar disorders: a systematic review and meta-analysis. In Psychological Medicine (Vol. 52, Issue 13). 10.1017/S 003329172200201 X 10.1017/S 003329172200201 XPMC 964751736016504 · doi ↗ · pubmed ↗
- 3Andreasen NC. (1984). Scale for the Assessment of positive symptoms (SAPS). Br J Psychiatry Suppl, 0(7).
- 4Chang X, Xi Y-B, Cui L-B, Wang H-N, Sun J-B, Zhu Y-Q, Huang P, Collin G, Liu K, Xi M, Tan Q-R, Miao D-M, Yin H. (2015). Distinct inter-hemispheric dysconnectivity in schizophrenia patients with and without auditory verbal hallucinations OPEN. 10.1038/srep 1121810.1038/srep 11218 PMC 445922026053998 · doi ↗ · pubmed ↗
- 5Davidson J, Turnbull CD, Strickland R, Miller R, Graves K. The Montgomery-Åsberg Depression Scale: reliability and validity. Acta Psychiatrica Scandinavica. 1986;73(5). 10.1111/j.1600-0447.1986.tb 02723.x.10.1111/j.1600-0447.1986.tb 02723.x 3751660 · doi ↗ · pubmed ↗
- 6Eve Lewandowski K, Balci Camsari G, Lewandowski KE, De Paola J, Camsari GB, Cohen BM, Öngür D. (2009). Tactile, olfactory, and gustatory hallucinations in psychotic disorders: a descriptive study cognition across the psychosis spectrum view project Cognitive Remediation View project Tactile, olfactory, and gustatory hallucinations in psychotic disorders: a descriptive study. 38(5). 10.47102/annals-acadmedsg.V 38N 5p 383
- 7Glahn DC, Bearden CE, Barguil M, Barrett J, Reichenberg A, Bowden CL, Soares JC, Velligan DI. The neurocognitive signature of psychotic bipolar disorder. Biol Psychiatry. 2007;62(8). 10.1016/j.biopsych.2007.02.001.10.1016/j.biopsych.2007.02.00117543288 · doi ↗ · pubmed ↗
- 8Jenkins LM, Bodapati AS, Sharma RP, Rosen C. Working memory predicts presence of auditory verbal hallucinations in schizophrenia and bipolar disorder with psychosis. J Clin Exp Neuropsychol. 2018;40(1). 10.1080/13803395.2017.1321106.10.1080/13803395.2017.132110628562181 · doi ↗ · pubmed ↗