Late Presentation of Posterior Urethral Valve in a Four-Year-Old Child With Subtle Voiding Symptoms: A Case Report
Hany M Elkordy, Mohamed Elkordi, Greta Peciulyte

TL;DR
A four-year-old boy with mild voiding symptoms was found to have a posterior urethral valve, highlighting the need for early evaluation of subtle urinary issues in children.
Contribution
This case report highlights the late presentation of posterior urethral valve in a child with subtle symptoms and successful treatment with laser ablation.
Findings
Type I posterior urethral valve was diagnosed incidentally in a four-year-old with mild voiding difficulty.
Transurethral laser ablation successfully managed the condition.
Early diagnosis and intervention are crucial to prevent renal complications in pediatric patients.
Abstract
A four-year-old male child following an attack of acute pharyngitis was referred to the urology department as having mild voiding difficulty, where posterior urethral valve (PUV) was incidentally diagnosed. Urethrocystoscopy confirmed Type I PUV, which was successfully managed with transurethral laser ablation. This case underscores the importance of evaluating subtle pediatric urinary symptoms to prevent renal complications. Advances in imaging, surgical techniques, and monitoring strategies are critical for effective management. Early diagnosis and timely intervention remain essential to preserve renal and bladder function, emphasizing the need for vigilance in assessing pediatric urinary complaints.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
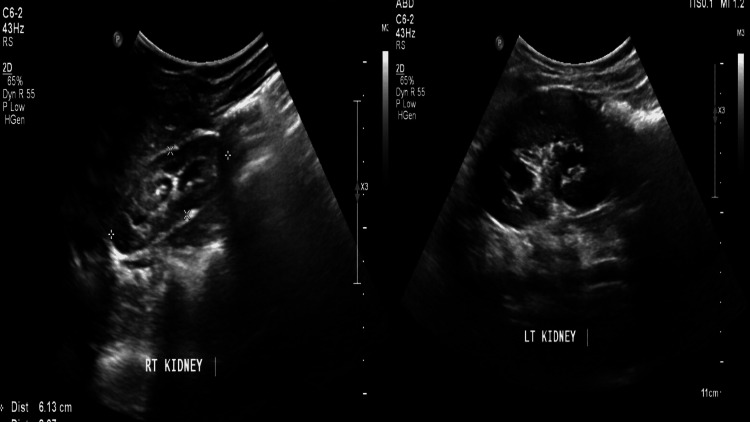 Figure 1
Figure 1 Figure 2
Figure 2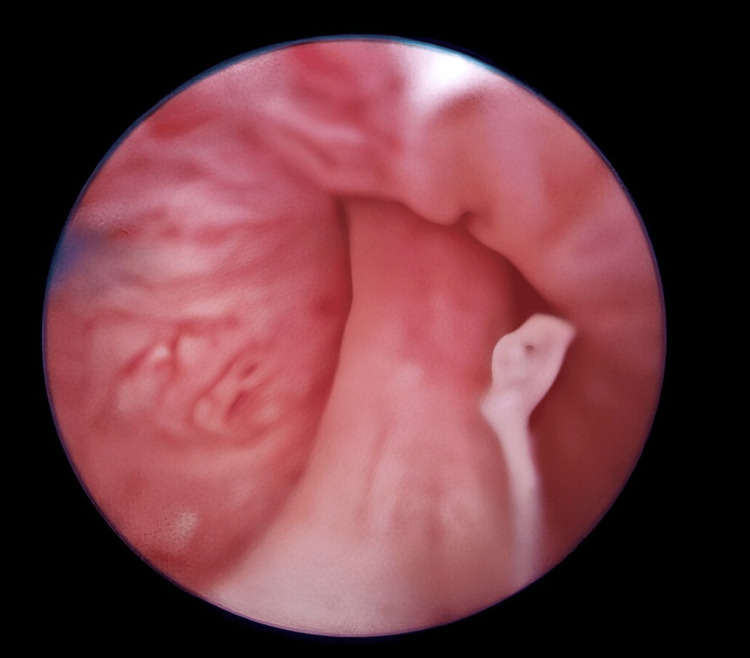 Figure 3
Figure 3 Figure 4
Figure 4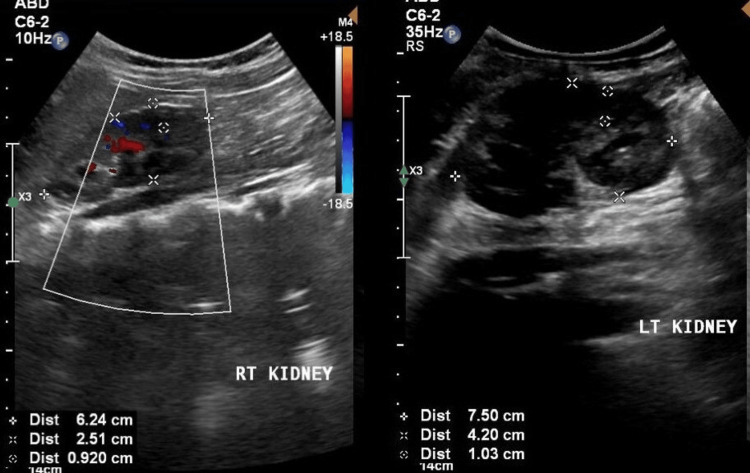 Figure 5
Figure 5Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPediatric Urology and Nephrology Studies · Urological Disorders and Treatments · Urologic and reproductive health conditions
Introduction
Posterior urethral valve (PUV) is the most common cause of congenital lower urinary tract obstruction (LUTO) in male patients, accounting for approximately 60% of cases. If left untreated, it can lead to significant renal and bladder dysfunction and may even become life-threatening. The incidence of PUV is estimated to be one in 7,000-8,000 live births [1,2].
According to Hugh Young's classification, PUV is categorized into three types, with only Type I and Type III considered obstructive. Type I, the most common form (90%-95% of cases), involves membranous folds extending from the verumontanum to the posterior urethra. Type II, which is rare, involves folds extending from the bladder neck to the verumontanum. Type III presents as a distal membranous diaphragm at the posterior urethra.
Recent studies have highlighted genetic predispositions linked to PUV, including associations with TBX5 and PTK7 genes, emphasizing the potential role of genome-wide association studies (GWAS) in understanding its pathogenesis [3]. Advances in prenatal ultrasonography have significantly improved the detection rates of LUTO, allowing for earlier diagnosis and intervention [4,5]. For postnatal assessment of PUV, a voiding cystourethrogram (VCUG) is recommended, including lateral views of the urethra during the voiding phase without a catheter in situ [6].
Management strategies for PUV range from prenatal interventions in specialized centers to postnatal approaches, including bladder drainage, vesicostomy, endoscopic valve ablation, and clean intermittent catheterization, and in severe cases, higher urinary diversion procedures may be needed [5,7].
Case presentation
A four-year-old boy was referred to the urology clinic with mild voiding symptoms, including a weak urine stream and straining to void, which had started two weeks prior to presentation. This followed an episode of acute pharyngitis. The parents reported that he had rarely experienced similar symptoms in the past and had otherwise maintained full bladder control. He had no prior significant medical or surgical history. Physical examination revealed normal external genitalia and unremarkable abdominal findings.
Laboratory findings revealed a serum creatinine level of 0.55 mg/dL, blood urea of 36 mg/dL, and normal complete blood count and electrolyte profile. Urine analysis and culture showed no bacterial growth. Ultrasound exam of the kidneys, ureters, and bladder (US-KUB) demonstrated mild-to-moderate bilateral hydronephrosis, thickened bladder wall, and dilated distal ureters, suggesting infravesical obstruction or reflux (Figure 1).
Ultrasound exam of the kidneys, ureters, and bladder (US-KUB) demonstrated mild-to-moderate bilateral hydronephrosis.
A VCUG revealed a dilated posterior urethra without evidence of vesicoureteral reflux, consistent with a PUV initial diagnosis (Figure 2).
A voiding cystourethrogram (VCUG) revealed a dilated posterior urethra without evidence of vesicoureteral reflux, consistent with a posterior urethral valve initial diagnosis.
After obtaining informed consent, we proceeded with diagnostic urethrocystoscopy under general anesthesia, and it confirmed Type I PUV, which was subsequently treated with laser ablation (Figure 3).
Urethrocystoscopy confirmed the diagnosis of Type I posterior urethral valve (PUV). A successful laser ablation was performed.
Endoscopic laser ablation of the PUV was performed successfully at the five and seven o’clock positions using a Holmium YAG laser at a setting of 1 J to 15-20 Hz. Cystoscopy revealed mild urinary bladder trabeculations. Both ureteric orifices were identified with no visible mass or diverticulum. The child was catheterized with Foley’s catheter for only 24 hours. Postcatheter removal, the child voided freely without complications. Follow-up results nine months later revealed normal renal function tests; VCUG showed resolution of the previously noted posterior urethral dilatation with no apparent urethral filling defects (Figure 4).
A voiding cystourethrogram (VCUG) showed resolution of the previously noted posterior urethral dilatation.
US-KUB demonstrated improvement in backpressure changes, although mild hydronephrosis persisted (Figure 5).
Ultrasound exam of the kidneys, ureters, and bladder (US-KUB) demonstrated improvement in backpressure changes, although mild hydronephrosis persisted.
Long-term follow-up was advised to monitor renal function and bladder compliance, along with close surveillance for urinary tract infections (UTIs), particularly given emerging evidence linking persistent bladder dysfunction to adverse outcomes.
Discussion
PUV remains a significant cause of morbidity in the pediatric population. While early presentations are common, late presentations with subtle symptoms pose critical diagnostic challenges and carry important implications for patient outcomes. Delayed diagnosis of PUV often results in progressive renal damage, bladder dysfunction, and a higher risk of long-term complications, including chronic kidney disease, hypertension, and, in some cases, the need for renal replacement therapy. These consequences highlight the importance of timely recognition and intervention [2].
Strategies for earlier detection must prioritize comprehensive antenatal and postnatal care. Prenatal ultrasonography remains a cornerstone of early detection, especially when findings such as oligohydramnios, bladder distension, or bilateral hydronephrosis are observed. Any degree of antenatal hydronephrosis, even when mild, warrants thorough postnatal follow-up. Postnatal ultrasonography within the first week of life is essential for evaluating the urinary tract in at-risk neonates. In cases of suspected obstruction, VCUG remains the gold standard for diagnosis, while urethrocystoscopy serves to confirm the diagnosis and guide treatment planning [8,9].
Educational initiatives targeted at primary care providers and pediatricians are crucial to raising awareness of the subtle presentations of PUV. Persistent lower urinary tract symptoms, even in the absence of overt findings, should prompt detailed evaluation. In resource-limited settings, improving access to diagnostic modalities, including VCUG and postnatal ultrasonography, is vital to ensuring earlier detection and better outcomes.
The primary treatment for PUV is endoscopic valve ablation, which has proven highly effective in relieving obstruction and preserving renal function. Advancements in surgical techniques, such as the use of cold knife, diathermy, Thulium, or Holmium YAG lasers, have further enhanced outcomes. In this case, Holmium YAG laser ablation was utilized, demonstrating high efficacy with minimal complications [7,9]. Management does not end with valve ablation; addressing residual bladder dysfunction is equally critical. Adjunctive therapies such as alpha-adrenergic blockers and clean intermittent catheterization are increasingly recognized as essential components of long-term care, particularly for patients with ongoing voiding dysfunction. Early and aggressive management of bladder dysfunction following valve ablation is critical to minimizing secondary complications and optimizing renal outcomes.
In conclusion, addressing the challenges of late presentation through earlier detection and comprehensive management is essential to mitigate the morbidity associated with PUV. By improving awareness, access to diagnostic tools, and the timely implementation of appropriate treatment, the burden of late-diagnosed PUV and its complications can be substantially reduced, ultimately enhancing patient outcomes.
Conclusions
Subtle urinary symptoms in children should prompt thorough evaluation for the possibility of PUVs. Early and timely intervention is crucial to prevent long-term renal and bladder complications. Laser ablation has emerged as a highly effective and minimally invasive treatment modality, offering excellent outcomes with minimal complication rates. Long-term follow-up remains essential to monitor renal function, bladder dynamics, and overall growth and development, ensuring optimal outcomes.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Posterior urethral valve World J Pediatr Nasir AA Ameh EA Abdur-Rahman LO Adeniran JO Abraham MK 205216720112182298810.1007/s 12519-011-0289-1 · doi ↗ · pubmed ↗
- 2Posterior urethral valves: overview of urologic management from the antenatal period to adulthood Curr Treat Options Pediatr Davis MF Zack J Weiss DA 4112025
- 3Diverse ancestry whole-genome sequencing association study identifies TBX 5 and PTK 7 as susceptibility genes for posterior urethral valves Elife Chan MM Sadeghi-Alavijeh O Lopes FM 11202210.7554/e Life.74777 PMC 951240136124557 · doi ↗ · pubmed ↗
- 4Posterior urethral morphology on initial voiding cystourethrogram correlates to early renal outcomes in infants with posterior urethral valves J Pediatr Urol Wu CQ Blum ES Patil D Smith EA 8138191820223584045610.1016/j.jpurol.2022.06.002 · doi ↗ · pubmed ↗
- 5Posterior urethral valve clinical assessment and outcome Asian Pac J Health Sci Kunal P Kumar S Priyanka Priyanka Ulla A 586562019
- 6Smeulders N, Makin E, Desai D, Duffy PG, Healy C, Cuckow PM et al. The predictive value of a repeat micturating cystourethrogram for remnant leaflets after primary endoscopic ablation of posterior urethral valves. J Pediatr Urol 2011; 7: 203-8J Pediatr Urol Yadav R Goel A 115820122053758910.1016/j.jpurol.2010.04.011 · doi ↗ · pubmed ↗
- 7Consensus on the management of posterior urethral valves from antenatal period to puberty J Indian Assoc Pediatr Surg Sharma S Joshi M Gupta DK 4142420193068688110.4103/jiaps.JIAPS_148_18PMC 6322183 · doi ↗ · pubmed ↗
- 8Long-term outcomes of kidney and bladder function in patients with a posterior urethral valve Medicine (Baltimore) Kim SJ Jung J Lee C Park S Song SH Won HS Kim KS 097201810.1097/MD.0000000000011033 PMC 599949929879071 · doi ↗ · pubmed ↗