Deep Brain Stimulation Lead Functional Repositioning After Spontaneous Pneumocephalus Resorption: A Clinical Case Presentation and Systematic Review
Yeimy Margarita Lebrón Sánchez, Viviana Torres, Angel Carreras, Alejandro A Jimenez Marrero, Ruben Dario Bleubar Ozoria, Lianca Rivera, Ambar Pérez-Fernández

TL;DR
A Parkinson's patient experienced electrode displacement after DBS surgery, but the electrodes spontaneously repositioned as air in the brain resolved, avoiding reoperation.
Contribution
This case and review highlight the rare occurrence of spontaneous electrode repositioning after pneumocephalus in DBS patients.
Findings
Electrode displacement occurred in 75% of cases, but only 12.5% showed spontaneous repositioning.
Spontaneous repositioning was more common with air volumes below 10 cm³.
Larger air volumes often required surgical intervention, but clear thresholds for action remain undefined.
Abstract
Deep brain stimulation (DBS) has become a critical intervention for managing advanced Parkinson's disease (PD), particularly for patients whose symptoms are no longer controlled by medication. This report details the case of a 61-year-old male with PD who experienced electrode displacement due to pneumocephalus following DBS surgery targeting the subthalamic nucleus (STN). Initial imaging revealed a significant subdural air volume causing electrode displacement. However, one month later, spontaneous pneumocephalus resorption led to the functional repositioning of the electrodes, restoring proper function and negating the need for reoperation. The accompanying systematic review analyzed 24 studies, involving 1,439 patients across 12 countries, to assess the occurrence and management in this specific scenario. Findings showed electrode displacement occurred in 75% of cases, but…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
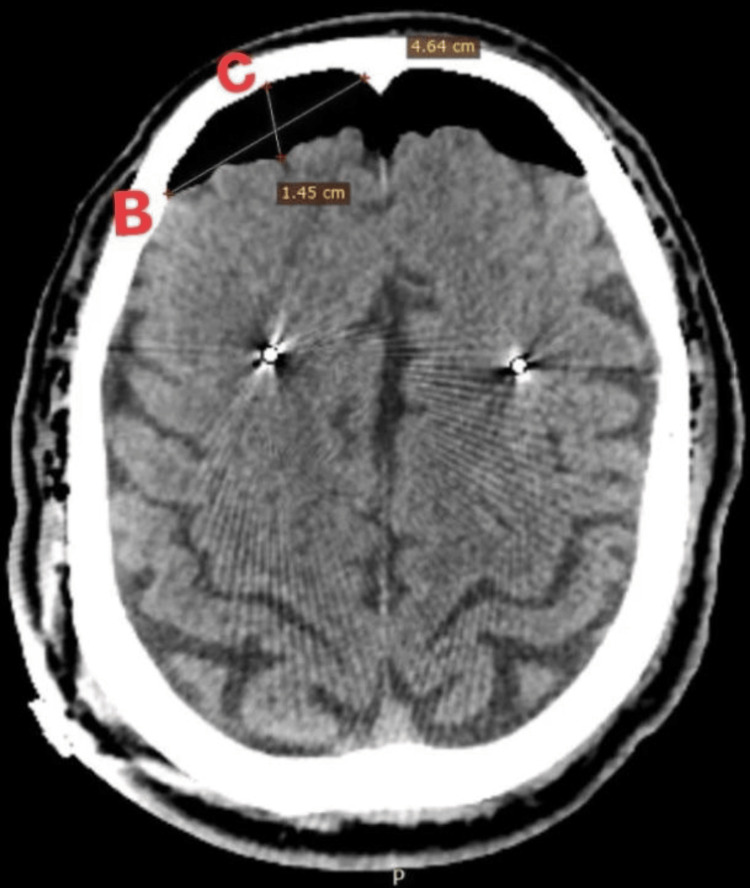 Figure 1
Figure 1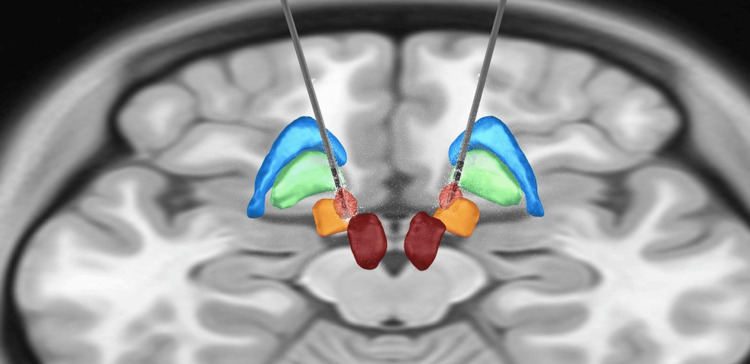 Figure 2
Figure 2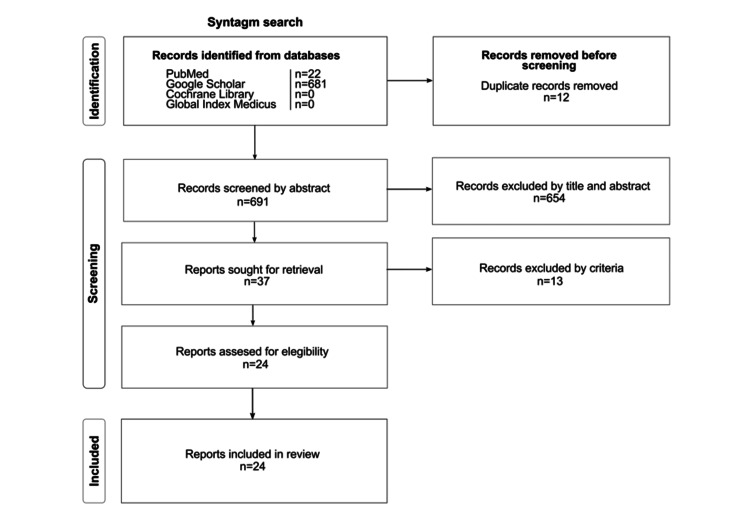 Figure 3
Figure 3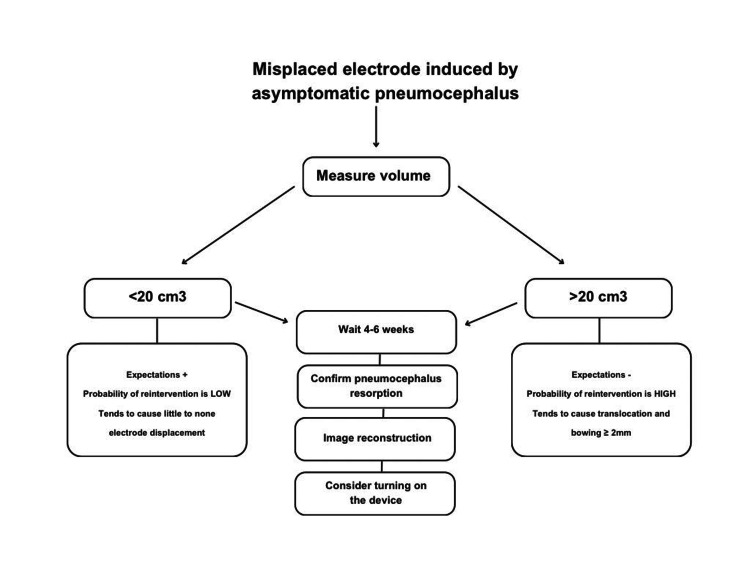 Figure 4
Figure 4| Country | n (%) |
| USA | 10 (41.7%) |
| China | 3 (12.5%) |
| Netherlands | 2 (8.3%) |
| Austria | 1 (4.1%) |
| Zurich | 1 (4.1%) |
| Japan | 1 (4.1%) |
| Spain | 1 (4.1%) |
| Turkey | 1 (4.1%) |
| Italy and USA | 1 (4.1%) |
| Sweden | 1 (4.1%) |
| South Korea | 1 (4.1%) |
| ID | Year of publication | Authors | Selection (max=4) | Comparability (max=2) | Exposure (max=3) | Total (max=9) |
| 1 | 2007 | Miyagi et al. 2007 [ | 3 | 2 | 3 | 8 |
| 2 | 2008 | Halpern et al. 2008 [ | 3 | 2 | 2 | 7 |
| 3 | 2009 | Richardson et al. 2009 [ | 3 | 2 | 3 | 8 |
| 4 | 2010 | Kim et al. 2010 [ | 3 | 1 | 3 | 7 |
| 5 | 2010 | Nazzaro et al. 2010 [ | 3 | 2 | 3 | 8 |
| 6 | 2010 | van den Munckhof et al. 2010 [ | 3 | 2 | 3 | 8 |
| 7 | 2011 | Azmi et al. 2011 [ | 3 | 2 | 3 | 8 |
| 8 | 2014 | Seijo et al. 2014 [ | 3 | 2 | 3 | 8 |
| 9 | 2015 | Sharim et al. 2015 [ | 3 | 2 | 3 | 8 |
| 9 | 2018 | Matias et al. 2018 [ | 3 | 2 | 3 | 8 |
| 10 | 2017 | Bentley et al. 2017 [ | 3 | 1 | 3 | 7 |
| 11 | 2018 | Matías et al. 2018 [ | 3 | 2 | 3 | 8 |
| 12 | 2020 | Albano et. al. 2020 [ | 3 | 1 | 3 | 7 |
| 13 | 2020 | Gong et al. 2020 [ | 3 | 2 | 3 | 8 |
| 14 | 2020 | Niederer et al. 2020 [ | 3 | 2 | 3 | 8 |
| 15 | 2021 | Göransson et al. 2021 [ | 3 | 2 | 3 | 8 |
| 16 | 2021 | Krauss et al. 2021 [ | 3 | 2 | 3 | 8 |
| 17 | 2021 | Piacentino et al. 2021 [ | 3 | 2 | 3 | 8 |
| 18 | 2021 | Taskin et al. 2021 [ | 3 | 2 | 3 | 8 |
| 19 | 2021 | van den Munckhof et al. 2021 [ | 3 | 2 | 3 | 8 |
| 20 | 2022 | Hart et al. 2022 [ | 3 | 2 | 3 | 8 |
| 21 | 2023 | Wu et al. 2023 [ | 3 | 2 | 3 | 8 |
| 22 | 2023 | Yuan et al. 2023 [ | 3 | 2 | 3 | 8 |
| 23 | 2024 | Chee et al. 2024 [ | 4 | 2 | 3 | 9 |
| 24 | 2024 | Martinez-Nunez et al. 2024 [ | * | * | * | * |
| ID | Year | n | Authors | Volume in cm3* | Is there electrode displacement outside the target? | Did the electrode spontaneously reposition itself? | Total lead deflection (mm) |
| 1 | 2007 | 18 | Miyagi et al. 2007 [ | NS | Yes | No | Mean±SD. 2.23±0.93 in Y axis and 0.39±0.68 in Z Axis. |
| 2 | 2008 | 50 | Halpern et al. 2008 [ | NS | Yes | No | 2 mm in Y axis. |
| 3 | 2009 | 8 | Richardson et al. 2009 [ | NS | Yes | No | NS |
| 4 | 2010 | 53 | Kim et al. 2010 [ | Mean±SD (Min-Max) 11.9±16.6 (0-76) | Yes | Yes | Mean±SD 0.6±0.5 in X axis, 1.1±0.9 in Y axis, and 1.0±0.8 in Z axis. |
| 5 | 2010 | 61 | Nazzaro et al. 2010 [ | Mean±SD 0.98±1.42 | No | No | NS |
| 6 | 2010 | 14 | van den Munckhof et al. 2010 [ | Mean±SD 17±24 | Yes | No | Mean±SD. 3.3±2.5 |
| 7 | 2011 | 32 | Azmi et al. 2011 [ | Mean±SD 13.57±12.44 | Yes | No | 0.88-1.33 |
| 8 | 2014 | 233 | Seijo et al. 2014 [ | Mean 20 | Yes | No | NS |
| 9 | 2015 | 85 | Sharim et al. 2015 [ | Mean±SD 21.49±13.70 | No | No | NS |
| 10 | 2017 | 73 | Bentley et al. 2017 [ | Mean±SD (Min-Max) 21.3±13.7 (0.1-65.9) | Yes | No | Mean±SD 2.0±1.2 |
| 11 | 2018 | 20 | Matias et al. 2018 [ | Median = 0.6, Min-Max: 0-32 | No | No | NS |
| 12 | 2020 | 2 | Albano et. al. 2020 [ | Patient 1: 54.29; Patient 2: 11.8 | Yes | No | NS |
| 13 | 2020 | 130 | Gong et al. 2020 [ | Mean±SD 10.1±12.6 | Yes | Yes | Mean±SD 0.76±0.24 |
| 14 | 2020 | 33 | Niederer et al. 2020 [ | Mean±SD 8.8±5.6 | Yes | No | Mean±SD 0.55±0.49 in X axis, 0.36±0.42 in Y axis, and 0.43±0.58 in Z axis. |
| 15 | 2021 | 23 | Göransson et al. 2021 [ | Mean (Min-Max) of two groups. Left side: 0.19 (0–8.76) Right side: 0.18 (0-2.01) | Yes | No | Mean±SD 0.44±0.72 in X axis, 0.64±0.54 in Y axis, and 0.62±0.71 in Z axis. |
| 16 | 2021 | 100 | Krauss et al. 2021 [ | Mean±SD 1.3±2.8 | No | No | NS |
| 17 | 2021 | 46 | Piacentino et al. 2021 [ | Mean of two groups. Supine position: 10.55, Semi-sitting position: 7.60 | Yes | No | 3.0 mm in X axis and 2.2 mm in Y axis. |
| 18 | 2021 | 30 | Taskin et al. 2021 [ | Mean of two groups. Bone cement: 12.1, Stimloc®: 13.9 | Yes | No | NS |
| 19 | 2021 | NS | van den Munckhof et al. 2021 [ | NS | NS | NS | NS |
| 20 | 2022 | 38 | Hart et al. 2022 [ | NS | Yes | No | 0.22±0.4 with only 3 (4%) electrodes out with 2 mm from the intended target. |
| 21 | 2022 | 255 | Wu et al. 2022 [ | Mean±SD of two groups. Elevated-head positioning group: 16.76±15.23, Supine positioning group: 3.25±8.78 | NS | No | NS |
| 22 | 2023 | 88 | Yuan et al. 2023 [ | uPVP* median of two groups. Cannula Puncture Group: 0.15% Cross-Incision: 0.50% | Yes | No | Mean±SD 0.29±0.44 in X axis, 0.62±0.39 in Y axis and not significant in Z axis. |
| 23 | 2024 | 46 | Chee et al. 2024 [ | Mean±SD. 4.49±6.05 | Yes, but less than 1mm. | No | NS |
| 24 | 2024 | 1 | Martinez-Nunez et al. 2024 [ | NS | Yes, intentionally during the surgery. | Yes | 1.4 medial and 1.4 posterior. |
| Clinical results | n (%) |
| Target | |
| STN | 16 (66.7%) |
| STN / GPi | 2 (8.3%) |
| GPi / STN / VIM | 1 (4.2%) |
| GPi / VIM | 1 (4.2%) |
| VIM / STN | 1 (4.2%) |
| GPi | 1 (4.2%) |
| Not specified | 2 (8.3%) |
| Electrode displacement | |
| Yes | 18 (75.0%) |
| No | 4 (16.7%) |
| Not specified | 2 (8.3%) |
| Spontaneous repositioning of the electrode | |
| Yes | 3 (12.5%) |
| No | 20 (83.3%) |
| Not specified | 1 (4.2%) |
| Time before re operation | |
| Provided | 6 (25.0%) |
| Not specified | 18 (75.0%) |
| Volume category | |
| Les than 10 cm³ | 7 (30.4%) |
| 10-20 cm³ | 7 (30.4%) |
| More than 20 cm³ | 3 (13.0%) |
| Not specified | 7 (30.4%) |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsNeurological disorders and treatments · Parkinson's Disease Mechanisms and Treatments · Botulinum Toxin and Related Neurological Disorders
Introduction
Parkinson's disease (PD) is a neurodegenerative disorder that affects approximately 1-3% of the population over the age of 60, significantly reducing their quality of life [1,2]. As the disease advances, patients often experience debilitating motor and non-motor symptoms, which can severely impair daily functioning and independence. While pharmacological treatments, primarily dopaminergic therapies, are effective in managing symptoms during the early stages, their efficacy diminishes over time, leading to fluctuations and complications.
In this context, deep brain stimulation (DBS) has emerged as a promising intervention for patients with advanced PD who are no longer adequately managed with medication alone [1-3]. DBS involves the implantation of electrodes in specific brain regions, which deliver electrical impulses to modulate neural activity and alleviate motor symptoms. This technique has been shown to substantially improve motor function and quality of life for appropriately selected patients.
Despite its benefits, DBS is a complex procedure with risks and possible complications related to the device, the procedure, electrical stimulation, and current spread. These complications may include intracerebral hematomas, intracranial hemorrhages, ischemic stroke, seizures, dyskinesias, dysarthria, mood changes, Horner's syndrome, as well as issues with the hardware such as migration, erosion, or rupture of the electrodes. Notably, the development of pneumocephalus - characterized by the accumulation of air within the skull following craniotomy - can also occur [4-6].
Pneumocephalus can lead to neurological symptoms, and, in the context of DBS, it may displace implanted electrodes, compromising the treatment’s effectiveness. Managing a pneumocephalus-induced electrode displacement requires careful evaluation and sometimes reoperation to restore optimal function.
This article presents a clinical case involving a 61-year-old male patient with PD treated with DBS of the subthalamic nucleus (STN). Twelve hours after surgery for DBS placement, a follow-up computed tomography (CT) scan revealed the presence of pneumocephalus with the subsequent electrode displacement, leading to the decision for reoperation. One month later, a magnetic resonance imaging (MRI) scan with DBS protocols in preparation for the new surgery demonstrated complete resorption of the pneumocephalus and proper alignment of the electrodes with the previously planned coordinates. Following this, the device was activated, and the patient exhibited very good control of his PD symptoms.
In light of this case, we proposed this systematic review to provide valuable insights into managing DBS electrode displacement due to pneumocephalus. Specifically, it will address two critical questions that could influence decision-making in this scenario: 1) how often does the position of DBS electrodes in the STN spontaneously correct after the appearance and resorption of pneumocephalus? and 2) what are the guidelines for managing DBS electrode displacement after the occurrence of pneumocephalus? By exploring these questions, we aim to enhance clinical decision-making and optimize patient outcomes in DBS procedures.
This article was previously presented at the XLI Latin American Congress of Neurosurgery (CLAN) 2024 on October 22, 2024, titled Review of DBS Complications.
Case presentation
We present the case of a 61-year-old male with an 11-year history of Parkinson's disease, classified as Hoehn and Yahr stage III. The patient exhibited severe global bradykinesia, handwriting impairment, freezing of gait, and rigidity, along with significant motor and non-motor fluctuations despite treatment with levodopa/carbidopa, pramipexole, amantadine, and clonazepam. The total Levodopa Equivalent Daily Dose (LEDD) was 1000 mg/day. Neurological examination revealed mild hypophonia, hypomimia, and moderate to severe bradykinesia with a slight resting tremor. Given the patient's severe motor fluctuations and satisfactory response to levodopa (61% improvement), we recommended bilateral DBS in the subthalamic nucleus to manage his symptoms.
The DBS implantation surgery was performed while the patient was awake and guided by microelectrode recording (MER), adhering closely to the planned coordinates throughout the procedure. Following the surgery, a follow-up CT scan revealed significant pneumocephalus. Subdural air volume was 25.11 cm³ (Figure 1), estimated in brain CT according to the following formula: A x B x C / 2 [7]. The mean distance between initial and delayed DBS lead tip position was <2 mm. At the time, the patient's clinical condition remained stable and without neurological deficits.
Early post-operative CT scan without contrast, showing subdural pneumocephalus of 25.11 cm³A: the number of air pockets noted x section thickness, B: widest diameter in axial section, C: widest diameter perpendicular to B.
Given these findings, the decision was made to reoperate. One month later, a new MRI performed in preparation for reintervention showed complete reabsorption of the pneumocephalus and realignment of the electrodes with the planned coordinates. Following this, stimulation was initiated and the patient’s parameters were adjusted to optimize therapeutic effects, resulting in better control of his symptoms. This improvement led to the decision to cancel the planned second surgery.
Lead-DBS [8,9] was used for 3D visualization of the final position of the electrodes and their relationship with the STN. Preoperative MRI and the latest CT scan were fused to establish the final electrode locations after air resorption. Additionally, a volume of tissue activated (VTA) model was constructed based on the stimulation parameters used, corroborating stimulus to the sensorimotor region of the STN, which correlates with the observed motor improvement (Figure 2).
3D reconstruction model of final DBS-lead position and VTADBS-lead: deep brain stimulation lead. VTA: volume of tissue activated (indicated in light red).Figure created by the authors using Lead-DBS (MATLAB) [9]
Ethical considerations
Informed consent was obtained from the patient to present his results to the scientific community following confidentiality principles and measures to safeguard the patient's physical and emotional well-being. This process adhered to the guidelines outlined in the Declaration of Helsinki regarding medical research involving human subjects [10].
Discussion
Literature search
This systematic review followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines [11]. We aimed to evaluate the management of DBS electrode displacement due to pneumocephalus in patients with Parkinson's disease.
A comprehensive literature search was performed. The search terms included a combination of keywords (syntax search): ((electrode) OR (lead)) AND ((pneumocephalus) AND (DBS) AND (Parkinson)) in the PubMed, Google Scholar, Cochrane Library, and Global Index Medicus databases. Studies that did not meet the research objectives, theses, monographs, books, animal studies, and studies not published in English or Spanish were excluded. These searches were conducted without date restrictions.
Methodological quality assessment
The quality of the selected articles was evaluated using the Newcastle-Ottawa Scale (NOS), which has shown reliability and validity for structured and standardized assessment of the quality of cohort and case-control studies based on content, design, and usability [12]. This scale consists of eight items, divided into three dimensions (comparison, selection, study type), where each study can receive a maximum of nine points or "stars." High-quality studies can score 7-9 stars, moderate quality 4-6 stars, and low quality 0-3 stars.
Data extraction, management, and analysis
From the collected literature, a clear set of data items were stablished to answer the review questions. These items were recorded in a spreadsheet and evaluated by three independent reviewers, using easy coding rules and response options to ensure consistent responses among them and prevent potential sources of bias or systematic errors. Criteria for unifying responses in fields such as median pneumocephalus volume and total lead deflection for each study were discussed academically with the other authors to reach consensus, and frequent comparisons were made to limit errors in interpreting the data items.
For each article, the following were identified: year of publication, number of patients included, country, language, target/planning, pneumocephalus volume, total lead deflection, reintervention (yes/no), waiting time before reintervention, spontaneous repositioning (yes/no), severity of the patient's disease before and after surgery as assessed by the Unified Parkinson's Disease Rating Scale (UPDRS) [13], and patient symptoms before and after DBS.
A descriptive statistical analysis [14] was performed on the variables identified in the articles, presenting their absolute frequencies (number of cases) and relative frequencies (percentages), calculated using the JASP 0.18.1 software [15].
Systematic review results
Study Characteristics
The systematic search procedure yielded 24 articles through the phases of identification, screening, and inclusion using syntax-based search (Figure 3).
Search strategy according to the scheme proposed in the PRISMA 2020 guidelines. PRISMA: Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
A total of 24 articles were selected, comprising one case report and 23 cohort studies, all written in English, considering a total of 1439 patients who received DBS for the treatment of Parkinson's disease in 12 countries (Table 1). Of these, eight studies (33.3%) were conducted in Europe, 10 in North America (41.6%), and six (25.0%) in Asia.
Methodological Quality and Publication Frequency
All cohort studies demonstrated excellent methodological quality according to the NOS (7-9 stars); one study received 9 stars (4.3%), 17 studies (73.9%) received 8 stars, and five studies (21.7%) received 7 stars (Table 2). This scale is not defined for case reports.
Regarding the frequency of publication per year, 24 publications were found between 2007 and 2024. Of these, 11 (45.8%) appeared sporadically before 2020 (0.84 publications per year), but between 2020 and 2024, 54.2% of the publications were found, with a frequency of 2.1 publications per year.
The cohort studies on which this review is based demonstrated excellent methodological quality according to the NOS criteria. One study (4.3%) achieved the maximum score of 9 stars due to its high level of rigor in participant selection, group comparability, and outcome measurement [36]. Most studies (73.9%) received 8 stars because none included a selection of an unexposed cohort, a criterion that involves comparing outcomes with a group of DBS patients who did not develop pneumocephalus. Five studies (21.7%) received 7 stars, indicating good methodological quality, with minor comparability or patient follow-up deficiencies. The Newcastle-Ottawa Scale is not designed to evaluate case reports, as it only applies to studies lacking a comparative design, such as case studies, thus limiting its utility in such contexts.
Surgical Outcomes
Regarding the volume of the pneumocephalus, it was reported in 14 out of 19 studies (73.7%), of which 13 reported volumes ranging between 0.18 and 54.29 cm³. One study conducted in China presented unilateral pneumocephalus volume percent (uPVP), which refers to the percentage of the affected cerebral hemisphere's volume concerning the total volume (Table 3).
In this systematic review, the subthalamic nucleus was the most frequently reported target, as it is the most commonly operated site in these procedures (Table 4).
Electrode displacement was often observed among patients undergoing this surgery. Spontaneous repositioning of the DBS electrode associated with pneumocephalus resorption was reported in three out of the 24 papers reviewed, with a total lead deflection <2mm in all three axles, the most reported volume of pneumocephalus ranging between 10 and 20 cm³.
Takeaways
This report highlights the complexities and potential complications associated with DBS for PD, particularly regarding pneumocephalus and electrode displacement.
In our case, initial post-operative imaging revealed a concerning pneumocephalus volume, prompting a decision for reoperation. However, a follow-up MRI a month later showed complete reabsorption of the pneumocephalus and realignment of the electrodes, suggesting that not all instances of electrode displacement require immediate surgical correction. Despite these insights, there remains a notable gap in the literature regarding standardized protocols for managing DBS electrode displacement due to pneumocephalus.
The systematic review revealed inconsistencies in reported practices and outcomes, indicating a need for more clarity on when surgical intervention is warranted. Based on the review, we highlight the following key findings:
Pneumocephalus and Electrode Displacement
Most studies suggest that smaller volumes of pneumocephalus (less than 10 cm³) are typically associated with spontaneous resorption and electrode repositioning. In contrast, larger volumes (greater than 20 cm³) tend to result in persistent electrode displacement, often requiring surgical intervention. This highlights the importance of controlling intracranial air volume postoperatively, as each additional cubic centimeter of intracranial air is associated with approximately 0.024 mm of DBS electrode translocation [28].
Challenges Posed by Pneumocephalus in DBS
Pneumocephalus significantly impacts the stability and effectiveness of DBS, with several studies demonstrating a direct correlation between larger pneumocephalus volumes and increased electrode displacement in the early postoperative period [19,22,32]. These findings underscore the importance of preventing the accumulation of intracranial air as a strategy to avoid electrode displacement and related complications.
Postoperative Monitoring and Electrode Localization
Ongoing monitoring of electrode migration in the weeks after surgery is crucial. Van den Munckhof et al. [33] recommend regular postoperative assessments with extended follow-up, particularly for patients with large volumes of subdural air. Additionally, studies such as that by Kim et al. suggest performing brain CT scans at least one month after surgery to more accurately assess electrode localization. While immediate postoperative imaging is crucial for confirming initial electrode placement, recent studies suggest that delayed follow-up imaging may offer a more precise assessment of final electrode position, especially in cases of significant cortical displacement [26].
Discrepancies in the Relationship Between Pneumocephalus and Electrode Displacement
Despite the general association between pneumocephalus and electrode displacement, some recent research has questioned the clinical significance of this relationship. In a study by Chee et al. [36], pneumocephalus volumes up to 22.0 cm³ did not result in significant brain displacement compared to patients without pneumocephalus. The mean magnitude of displacement was less than 1.0 mm, regardless of intracranial air volume. These findings suggest that while pneumocephalus is often associated with electrode displacement, its clinical impact may not be significant in all cases, and other factors may contribute to electrode migration.
Clinical and Temporal Considerations
A practical scale proposed by Gong et al. [27] to assess DBS surgery outcomes reported that in one out of 130 patients (0.8%), electrodes spontaneously realigned with their intended target one week after pneumocephalus caused a posterior bending of the lead. Martinez-Nunez (2024) [37] also described a case in which pneumocephalus was detected during surgery, and a cannula was left in place to guide electrode repositioning. Although the frequency of publications on this issue has increased from 0.8 articles per year between 2007 and 2018 to an average of 2.5 articles between 2020 and 2023 [1,34], such cases remain relatively rare.
Reoperation Decision-Making
The decision to reoperate is typically driven by the lack of clinical improvement or the progression of symptoms attributed to pneumocephalus [26]. This symptom-based approach highlights the importance of close monitoring in the immediate postoperative period, with reoperation indicated if neurological symptoms worsen or if complications arise. On the other hand, electrode migration can be evaluated over up to one year [32]. However, there is no consensus on the optimal time for reassessment, with studies suggesting time frames ranging from a few days to one year for potential reoperation. This approach disparity underscores the need for clearer, more standardized guidelines for clinical decision-making in electrode displacement cases, considering both clinical progression and electrode stability.
Proposed Management Algorithm or Decision-Making Protocol
Given the lack of standardized protocols, we propose a management algorithm to guide decision-making in DBS electrode displacement caused by pneumocephalus.
The protocol outlined in Figure 4 suggests a clinical approach for managing electrode displacement following DBS surgery, particularly due to pneumocephalus.
Decision-making protocol for electrode displacement management following deep brain stimulation surgery.
Conclusions
Spontaneous DBS lead repositioning after pneumocephalus resorption is rare and depends on factors like intracranial air (ICA) volume. This review highlights a lack of evidence to guide decision-making in these cases, particularly in Latin America. Clinicians must balance clinical signs with imaging findings, as not all electrode displacements require surgery. Further research is needed to develop clear, region-specific protocols to guide management and follow-up, tailored to individual patient needs.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Deep brain stimulation in Parkinson disease: a meta-analysis of the long-term neuropsychological outcomes Neuropsychol Rev Bucur M Papagno C 3073463320233531858710.1007/s 11065-022-09540-9PMC 10148791 · doi ↗ · pubmed ↗
- 2Deep brain stimulation of the subthalamic nucleus in Parkinson's disease: from history to the interaction with the monoaminergic systems Prog Neurobiol Faggiani E Benazzouz A 13915615120172741211010.1016/j.pneurobio.2016.07.003 · doi ↗ · pubmed ↗
- 3The related factors and effect of electrode displacement on motor outcome of subthalamic nuclei deep brain stimulation in Parkinson’s disease J Clin Med Yuan T Chen Y Zhu G Zhang J 12202310.3390/jcm 12247561 PMC 1074411538137630 · doi ↗ · pubmed ↗
- 4Risks of common complications in deep brain stimulation surgery: management and avoidance J Neurosurg Fenoy AJ Simpson RK Jr 13213912020142423665710.3171/2013.10.JNS 131225 · doi ↗ · pubmed ↗
- 5Surgical adverse events of deep brain stimulation in the subthalamic nucleus of patients with Parkinson's disease. The learning curve and the pitfalls Acta Neurochir (Wien) Seijo F Alvarez de Eulate Beramendi S Santamarta Liébana E Lozano Aragoneses B Saiz Ayala A Fernández de León R Alvarez Vega MA 1505151215620142475272410.1007/s 00701-014-2082-0 · doi ↗ · pubmed ↗
- 6Rare complications during deep brain stimulation surgery for Parkinson’s disease J Neuroanaesth Crit Care Vanamoorthy P Tomar A Prabhakar H Rath GP 15015212018
- 7Intracerebral hemorrhage volume measurement Stroke Broderick JP Brott TG Grotta JC 10812519948165684 · pubmed ↗
- 8Deep brain stimulation: imaging on a group level Neuroimage Treu S Strange B Oxenford S Neumann WJ Kühn A Li N Horn A 11701821920203250569810.1016/j.neuroimage.2020.117018 · doi ↗ · pubmed ↗