Progressive Unilateral Proptosis and [ 18 F]FDG-Avid Lesions Connoting Aggressive Disease in Radioiodine-Refractory Differentiated Thyroid Carcinoma
Yeshwanth Edamadaka, Rahul V. Parghane, Sandip Basu

TL;DR
A patient with thyroid cancer that no longer responds to radioiodine developed aggressive disease shown by FDG scans and worsening symptoms.
Contribution
Demonstrates the aggressive nature of FDG-avid lesions in radioiodine-refractory thyroid cancer through a clinical case.
Findings
The patient developed orbital metastasis after radioiodine therapy, presenting as sudden unilateral proptosis.
FDG-PET/CT showed more FDG-avid lesions than radioiodine-avid lesions, indicating aggressive disease progression.
Despite targeted therapies, the disease progressed, highlighting the poor prognosis of FDG-avid RAIR-DTC.
Abstract
Radioiodine-refractory differentiated thyroid carcinoma (RAIR-DTC) have poor prognosis as compared with radioiodine concentrating thyroid carcinoma. We present a case of follicular thyroid carcinoma presenting as a disseminated disease initially, underwent thyroid surgery and radioiodine (RAI) therapy. Following RAI, the patient developed a sudden-onset unilateral proptosis, finally diagnosed as orbital metastasis. [ 18 F]-Fluorodeoxyglucose (FDG)-positron emission tomography-computed tomography identified FDG-avid metastatic lesions more numerous than the RAI-avid lesions. The patient was treated with local and systemic targeted therapy, but despite these treatments, he developed progressive disease indicating aggressive nature of the disease consistent with [ 18 F]FDG-avid RAIR-DTC.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
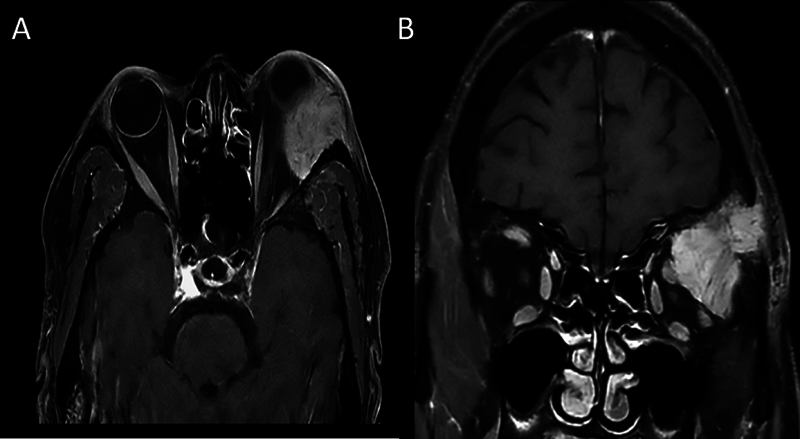 Fig. 1
Fig. 1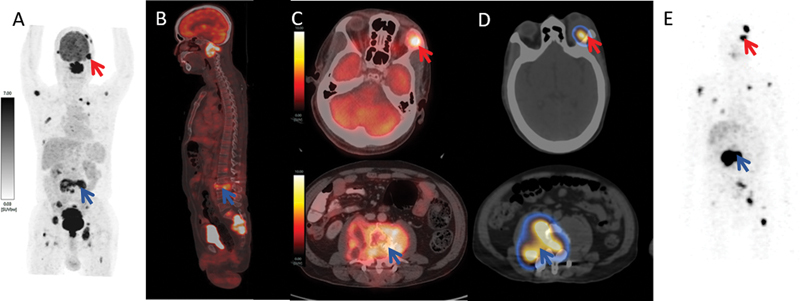 Fig. 2
Fig. 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsThyroid Cancer Diagnosis and Treatment · Medical Imaging Techniques and Applications · Radiomics and Machine Learning in Medical Imaging
Introduction
Differentiated thyroid carcinoma (DTC) is the most common type of endocrine malignant tumor. The standard of care is surgery followed by radioactive iodine (RAI) therapy in most cases of DTC. Recently, the American Thyroid Association guideline introduced the term radioiodine-refractory DTC (RAIR-DTC), which have poor prognosis with limited therapeutic options. 1 We present a patient of follicular thyroid carcinoma diagnosed from lumbar vertebral metastasis, presenting as disseminated disease initially, and treated with surgery and RAI therapy. Following RAI, he developed sudden-onset unilateral proptosis finally diagnosed as orbital metastasis from DTC.
Case History
A 57-year-old male patient presented with chronic lower back pain which on magnetic resonance imaging (MRI) evaluation revealed multiple lytic skeletal lesions in the spine with L3 vertebral collapse. Histopathological analysis from L3 lesion showed metastatic disease from follicular thyroid carcinoma with immunohistochemistry positive for TTF-1, thyroglobulin, PAX8, and K i -67 index of 15%. The patient underwent total thyroidectomy followed by high-dose RAI therapy. Post-RAI follow-up (8 months after RAI), he developed a sudden-onset swelling in the left orbital region ( Fig. 1A ). He was evaluated with MRI which revealed an ill-defined lobulated lesion in the lateral aspect of the orbit abutting the superior and lateral rectus muscles with temporal bone with invasion and no intracranial extension noted ( Fig. 1B and C ).
Clinical patient image showing unilateral proptosis in the left eye with epiphora ( A ). Axial T1 postcontrast magnetic resonance imaging (MRI) showing an ill-defined lobulated lesion in the lateral aspect of the orbit in extraconal space displacing the globe anteriorly ( B ). Coronal T1 postcontrast MRI showing the lesion abutting the superior and lateral rectus muscles with temporal bone invasion ( C ).
He underwent [18F]-fluorodeoxyglucose (FDG)-positron emission tomography-computed tomography (PET/CT), which showed increased uptake in left orbital lesion, multiple skeletal lesions, and lung lesions ( Fig. 2A–C ). Whole-body (WB) radioiodine ( ^131^ I) single-photon emission CT/ CT, showed radioiodine uptake in the metastatic left orbital lesion and multiple skeletal lesions ( Fig. 2D and E ). The patient received a palliative external beam radiotherapy (EBRT) to the orbit lesion and lumbar vertebral lesions and was given tablet lenvatinib 14 mg once daily. He tolerated the treatment well initially, but presented with spastic paresis 3 months after EBRT and developed symptoms of weight loss and increase in orbital swelling with declining performance, which was treated as supportive treatment.
[18F]-Fluorodeoxyglucose (FDG)-positron emission tomography-computed tomography (PET/CT), maximum intensity projection (MIP) image ( A ) and sagittal fused image ( B ) demonstrating hypermetabolic multiple lytic skeletal lesions at the calvarium, left orbit (red arrow), C2 vertebra, multiple ribs, L3 vertebra (blue arrow), multiple pelvic bone, and sacrum with intraspinal extension (blue arrow). Axial fused images ( C ) showing [18F]FDG-avid (maximum standardized uptake value [SUVmax] 11.50) left lateral extraconal orbital metastasis (red arrow) and [18F]FDG-avid (SUVmax 14.50) L3 vertebral metastasis with compression fracture and associated soft tissue component (blue arrow). 131 I fused axial single-photon emission computed tomography (SPECT)/computed tomography (CT) images ( D ) and whole-body MIP SPECT/CT image ( E ) showing 131 I uptake in left lateral extraconal orbital metastasis, L3 vertebral lesion, and other skeletal lesions, but on comparison with [18F]FDG-PET/CT scan, 131 I scan showed lack of concentration in cervical and sacral metastatic lesions suggestive of dedifferentiation and aggressive disease.
Discussion
The recent consensus statement by the American Head and Neck Society, Endocrine Surgery Section, and International Thyroid Oncology Group has defined advanced thyroid carcinoma according to four categories including surgical, biochemical, molecular, and at discretion of clinician when features portend aggressive tumor behavior. In the literature, various studies indicated that patients of RAIR-DTC had the worst outcome with a median 10-year survival rate of 10%. 2 Before considering systemic treatments in patients with advanced thyroid carcinoma, local therapies are typically offered to symptomatic disease. The targeted therapy in RAIR-DTC is recommended in cases with a rapidly progressive tumor, symptomatic disease, and tumors in a threatening location. 3 The multikinase inhibitors for advanced thyroid carcinoma include sorafenib and lenvatinib as initial targeted therapy, while cabozantinib received approval as second-line therapy without any biomarker selection. 4 The use of targeted therapy in RAIR-DTC should be made by a multidisciplinary team while weighing risks versus benefits and close surveillance for any treatment-related side effects and disease progression. 5 Thyroid carcinoma rarely metastasizes to orbit with only 3% from thyroid origin. 6 They often present with symptoms of diplopia, ocular pain, and vision loss coupled with globe displacement and palpable masses. 7 [ ^18^ F]FDG-PET/CT is of considerable value in characterizing patients with advanced thyroid carcinoma presenting with suspected orbital metastases and further evaluating global WB disease burden. 8 For the treatment of symptomatic orbital metastasis in DTC, local EBRT is useful with overall response rates between 75 and 100%, a median local control rate of 11 months after EBRT. 9 We herein presented a rare case of progressive orbital metastasis in RAIR-DTC, demonstrating more [18F]FDG-avid lesions than radioiodine-avid disease and received local therapy as well as systemic targeted therapy, but eventually the patient developed progressive disease within a short period of time connoting aggressive nature of disease in RAIR-DTC.
Conclusion
[18F]FDG-PET/CT plays a crucial role in identifying dedifferentiated lesions, evaluating global metastatic burden, and as a prognostic biomarker in RAIR-DTC. FDG-avidity in RAIR-DTC can signify a poor prognosis and outcome despite local therapy and systemic targeted therapy. Unilateral proptosis in known case of thyroid carcinoma should raise a suspicion of metastasis and need urgent investigation for diagnosing this rare site metastasis in DTC.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Lim H Devesa S S Sosa J A Check D Kitahara C M Trends in thyroid cancer incidence and mortality in the United States, 1974–2013 JAMA 2017317131338134828362912 10.1001/jama.2017.2719 PMC 8216772 · doi ↗ · pubmed ↗
- 2Durante C Haddy N Baudin E Long-term outcome of 444 patients with distant metastases from papillary and follicular thyroid carcinoma: benefits and limits of radioiodine therapy J Clin Endocrinol Metab 200691082892289916684830 10.1210/jc.2005-2838 · doi ↗ · pubmed ↗
- 3Haugen B R Alexander E K Bible K C 2015 American Thyroid Association Management guidelines for adult patients with thyroid nodules and differentiated thyroid cancer: the American Thyroid Association Guidelines Task Force on Thyroid Nodules and Differentiated Thyroid Cancer Thyroid 20162601113326462967 10.1089/thy.2015.0020 PMC 4739132 · doi ↗ · pubmed ↗
- 4Shonka D C Jr Ho A Chintakuntlawar A V American Head and Neck Society Endocrine Surgery Section and International Thyroid Oncology Group consensus statement on mutational testing in thyroid cancer: defining advanced thyroid cancer and its targeted treatment Head Neck 202244061277130035274388 10.1002/hed.27025 PMC 9332138 · doi ↗ · pubmed ↗
- 5Agosto Salgado S Kaye E R Sargi Z Chung C H Papaleontiou M Management of advanced thyroid cancer: overview, advances, and opportunities Am Soc Clin Oncol Educ Book 202343 e 38970837186883 10.1200/EDBK_389708 · doi ↗ · pubmed ↗
- 6Palmisciano P Ferini G Ogasawara C Orbital metastases: a systematic review of clinical characteristics, management strategies, and treatment outcomes Cancers (Basel)202114019435008259 10.3390/cancers 14010094 PMC 8750198 · doi ↗ · pubmed ↗
- 7Valenzuela A A Archibald C W Fleming B Orbital metastasis: clinical features, management and outcome Orbit 200928(2-3):15315919839900 10.1080/01676830902897470 · doi ↗ · pubmed ↗
- 8Kalemaki M S Karantanas A H Exarchos DPET/CT and PET/MRI in ophthalmic oncology (Review)Int J Oncol 2020560241742931939615 10.3892/ijo.2020.4955 PMC 6959466 · doi ↗ · pubmed ↗