Outcomes of Primary Total Hip Arthroplasty Using Custom Femoral Stems in Patients With Secondary Hip Osteoarthritis: A Systematic Review
Kevin Ilo, Prith Hallikeri, Habillan Naathan, Bernard Van Duren, Mark Higgins, Iain McNamara, Toby Smith

TL;DR
This study reviews outcomes of custom femoral stems in hip replacements for patients with complex hip anatomy due to secondary osteoarthritis.
Contribution
The study provides a systematic review of custom femoral stem outcomes in primary THA for secondary osteoarthritis patients.
Findings
Custom femoral stems showed 6.9% reoperation and 8.25% revision rates over an average 11.6-year follow-up.
Postoperative Harris Hip Score improved by an average of 40.32 points.
Intraoperative fracture rate was 3.23%, and leg length discrepancy averaged 4.25 mm.
Abstract
This systematic review aims to evaluate the effectiveness and safety of custom femoral stems in primary total hip arthroplasty (THA) for patients with secondary osteoarthritis with abnormal hip anatomy. Following Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines, databases were systematically searched for studies published on primary THA utilizing custom femoral stems. Inclusion criteria were studies on patients with secondary osteoarthritis receiving custom stems, with outcomes including implant survival, revision rates, and functional scores. Data were extracted from eligible studies, with a focus on overall and cause-specific revision rates. A total of 689 studies were screened, 13 met the inclusion criteria, encompassing 806 patients and 951 custom THA procedures. The collective follow-up period averaged 11.6 years, with a mean age of 44.6…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
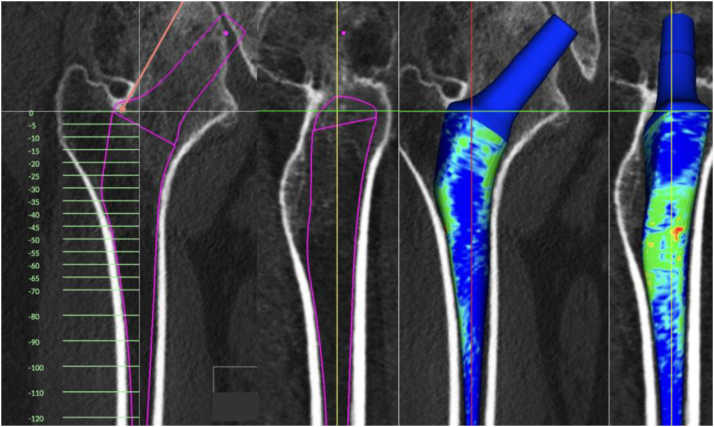 Figure 1
Figure 1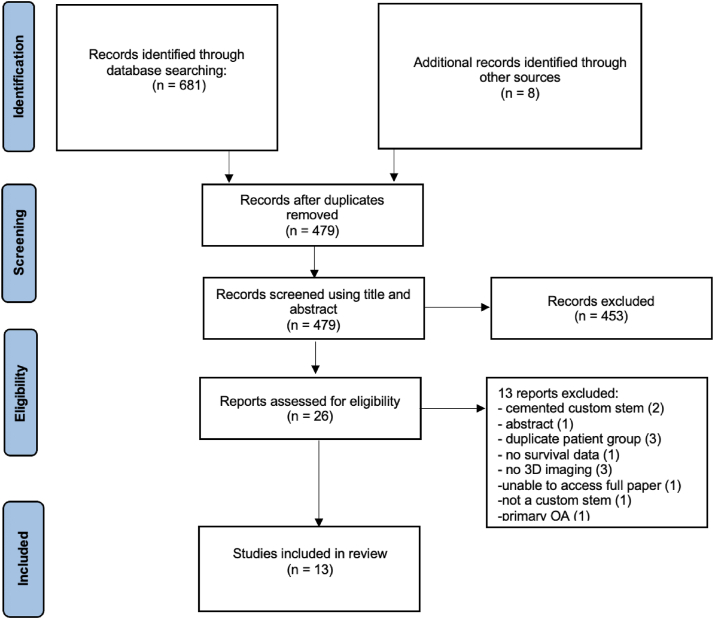 Figure 2
Figure 2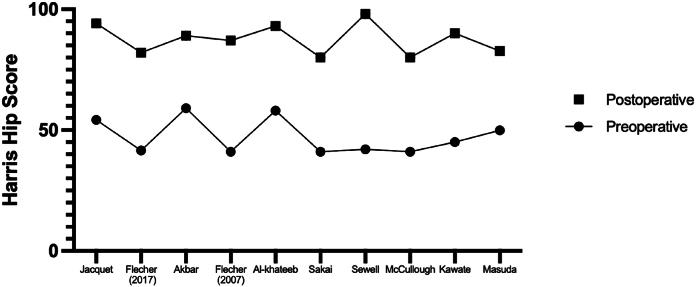 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsOrthopaedic implants and arthroplasty · Total Knee Arthroplasty Outcomes · Orthopedic Infections and Treatments
Introduction
Total hip arthroplasty (THA) is increasingly being utilized to treat younger, more active patients who have developed secondary hip osteoarthritis due to congenital or acquired conditions [1,2]. This poses new challenges in surgical practice and implant design, especially when addressing patients with complex hip anatomy [3]. Cemented femoral stems have been the preferred solution for addressing femoral abnormalities due to their versatility and flexibility during surgery to recreate a patient's normal hip biomechanics [4,5]. However, there are concerns regarding the durability of cemented fixation in younger and more active patients [6,7]. Furthermore, recent studies have highlighted an increased risk of periprosthetic fractures with certain designs of cemented femoral stems [[8], [9], [10]]. As a result, cementless and biological fixation is desirable [11]. Custom cementless femoral stems have the potential to address such issues, especially for patients with femoral deformities. Achieving primary stability is crucial for THA success, but it can be challenging with standard cementless femoral stems, especially in the presence of anatomical irregularities as the proximal femur has a wide range of anatomical variations [12]. These variations make it difficult to achieve an optimal fit-and-fill of the metaphysis with commercially available prostheses, despite the availability of various anatomical designs and sizes [13].
Custom femoral stems, designed and tailored through advanced preoperative three-dimensional (3-D) imaging techniques, are a promising solution (Fig. 1). They have shown considerable utility in treating a range of conditions, including primary osteoarthritis, osteoarthritis secondary to abnormal anatomy, and revision surgery [[14], [15], [16], [17]]. By tailoring the design to the individual's specific anatomy, custom stems ensure a more precise fit, recreating normal hip mechanics and stability, in theory improving their overall outcome [[18], [19], [20], [21]]. For patients with femoral deformity and a long-life expectancy, custom cementless femoral stems represent an encouraging alternative to standard femoral stems. This approach addresses the unique challenges posed by the patient's anatomy and age, offering a solution that aligns more closely with their physiological requirements.Figure 1. Design of a custom femoral stem utilizing computer tomography imaging for abnormal proximal femur anatomy.
Despite the potential of custom femoral stems, there is a lack of comprehensive clinical outcomes data for custom femoral stems in primary THA, especially in patients with abnormal hip anatomy. This review aims to address this need by examining the clinical outcomes associated with the use of custom femoral stems in secondary hip osteoarthritis, focusing on patients with abnormal hip anatomy and deformity and exploring their benefits and challenges in modern orthopedic practice.
Material and methods
This systematic review adheres to the guidelines outlined in the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) [22] and has been registered with PROSPERO (Registration: CRD42023488321).
Search strategy
The search strategy involved an electronic literature search conducted on November 1, 2023, encompassing Medline, Embase, Cochrane, and CINAHL databases. The search terms, including variations of "custom," "stem," and "total hip arthroplasty," were crafted to identify relevant studies (full search strategy in supplemental material). In addition to database searches, reference lists of selected articles and trial registries were scrutinized to identify further relevant studies.
Eligibility criteria
Inclusion criteria comprised studies reporting clinical outcomes of custom femoral stems designed from preoperative 3-D imaging in secondary hip osteoarthritis. Studies where the majority of the population group (>50%) was diagnosed with primary osteoarthritis were excluded. The exclusion criteria also encompassed non-English studies, those published before 2000, revision THA studies, custom femoral stems not made with 3-D imaging, cemented stems, narrative reviews, expert opinions, and case reports.
The titles and abstracts of all references from the search results were screened for inclusion by 2 independent reviewers (KI, PH). These authors then reviewed the full text of the studies, and disagreements between the 2 reviewers were resolved through review and consensus with a third reviewer (HN).
Data extraction
Three reviewers (KI, PH, HN) independently reviewed each study and extracted relevant review data. This included year of publication, population characteristics, indication for surgery, type of stem, surgical approach, follow-up duration, type of acetabulum component, and patient demographics. Outcomes including revision rates, reoperation rates, postoperative leg length discrepancies, survival rates of the femoral stem and both components, and preoperative and postoperative patient-reported outcomes were also collected.
Outcomes
The primary outcome was reoperation events. Secondary outcomes included revision and survival, intraoperative complications, postoperative complications, leg-length discrepancy, patient-reported outcome measures, and health resource use/cost-effectiveness analysis data.
Critical appraisal
The quality of each study was evaluated using the Joanna Briggs Institute Checklist, an appraisal tool for case series which is an approved method to assess the methodological quality of these studies [23]. This checklist consists of 10 questions, and a point was scored for each, giving a maximum of 10 points. Assessments were performed by one reviewer (KI) and independently verified by 2 other reviewers (HN and PH).
Data synthesis
Outcomes from the studies were recorded. Arithmetic and weighted means were calculated. Data extraction tables were reviewed for study heterogeneity. Where there was substantial heterogeneity in study design, population characteristics, and surgical procedure, a narrative analysis was performed. Continuous data were assessed using a mean difference and presented with 95% confidence intervals (CIs). Dichotomous data were assessed with relative risk and presented with 95% CI. All data were analyzed using Prism 10 (Prism 10, GraphPad Software, San Diego, CA).
Results
Search results
A total of 689 studies were identified, and of these, 202 were duplicates (Fig. 2). A further 41 studies were removed as they were carried out prior to the year 2000 and not in English. The remaining 438 studies were screened using title and abstract. This resulted in the inclusion of 51 studies for full-text screening. Out of these, 13 studies met the inclusion criteria in the systematic review. All 13 studies reported on the clinical outcomes of primary THA using custom stems designed from 3-D imaging in patients with secondary hip osteoarthritis. One study (Jacquet et al.) reported on 2 series of patients [24]. All included studies were case series [17,[24], [25], [26], [27], [28], [29], [30], [31], [32], [33], [34], [35]].Figure 2PRISMA flow diagram.
Study characteristics
The included studies exhibited a mean follow-up duration of 11.6 years (95% CI: 9.48-13.74). The collective patient pool across the studies comprised 806 individuals and 951 custom femoral THAs (Table 1). The mean number of custom femoral stems included in each study was 67.9 (95% CI: 36.1-99.8). The mean age of patients who received a custom femoral stem was 44.6 years (95% CI: 38.4-50.9) with a mean BMI (4 studies included the mean BMI) of 25.4 kg/m^2^ (95% CI: 23.7-27.0). The indications for THA in each study are summarized in Table 1. There were no studies that compared patients with secondary hip osteoarthritis to patients with primary hip osteoarthritis. There were also no studies that compared custom femoral stems to off-the-shelf stems.Table 1. Characteristics of included studies.StudyNo. of patientsNo. of hipsIndicationApproachMean age (range)Male no. (%)Mean BMI (range)Jacquet et al.2020 [24]212233Primary OA 17.6%,Secondary OA 49.4%AVN 33%DDH 37.8%,Post-traumatic 11.6%Anterolateral39.6 (20-50)106 (50%)25 (16-48)2126DDH (Crowe 3 and 4)Anterolateral45 (17-73)13 (61.9%)27.2 (16-52)Flecher et al.2018 [25]2323Hip fusionWatson Jones49 (28-69)13 (56.6%)25 (19-33)Pakos et al.2015 [35]6786DDHPosterolateralMedian 487 (10.50%)Median 26.81Akbar et al.2009 [26]6172Dysplasia 34.7%Hip dislocation 11.1%AVN 11.1%OA 2.8%Post-traumatic 16.7%Perthes 11.1%RA 9.7%SUFE 2.8%Anterolateral35 (22-40)33 (54%)26 (18-41)Flecher et al.2007 [27]7997Congenital hip dislocation Crowe 1 = 38.1%Crowe 2 = 28.9%Crowe 3 = 13.4%Crowe 4 = 19.6%Watson Jones48 (17-72)5 (6.3%)Not statedAl-Khateeb et al.2014 [28]1415PerthesAnterolateral or posterior32.8 (23-55)6 (42.9%)Not statedKoulouvaris et al.2008 [29]3848Congenital dislocation of hipPosterolateral47 (22-69)Not statedNot statedBenum et al.2010 [33]8383Primary OA 19%Dysplasia 57%Perthes 12%RA 6Post-traumatic 1%AVN 2%Other 2%Direct lateral46 (20-60)36 (43.4%)Not statedSakai et al.2006 [17]7799Congenital hip dysplasiaCrowe 1 = 47.5%Crowe 2 = 41.4%Crowe 3 = 11.1&Posterolateral54 (40-73)7 (9.1%)23.6 (17.3-30.6)Sewell et al.2011 [30]2540Skeletal dysplasiaAnterolateral or Posterior,37.5 (18-61)15 (60%)Not statedMcCullough et al.2006 [31]2542Inflammatory polyarthropathyNot stated21 (11-35)7 (28%)Not statedKawate et al.2009 [34]5355Dysplastic hipsPosterolateral60 (40-73)5 (9.4%)Not statedMasuda et al.2016 [32]2832Dysplastic hips with previous osteotomyPosterolateral62 (29-77)2 (7.1%)Not statedAVN, avascular necrosis; DDH, developmental dysplasia of hip; OA, osteoarthritis; RA, rheumatoid arthritis; SUFE, slipped upper femoral epiphysis.
Design of custom stems
Of the 13 included studies of custom femoral stems, there were 6 different manufacturers, and in one study, the manufacturer was not stated (Supplementary Material). All custom stems were designed from computer tomography imaging. They were all uncemented, and 11 studies specified a coating with hydroxyapatite; however, not always stating whether fully or partially. In addition, 10 studies mentioned the material of the femoral stem (titanium alloy), while others did not provide specific material details. The lengths of the custom femoral stems were stated in 4 studies.
Survival rates, revisions, and reoperations
Eleven studies (N = 780) presented reoperation rates (Table 2). At a mean follow-up of 11.6 years, the overall mean reoperation rate was 6.9% (95% CI: 3.24-10.13). The range of reoperation rates in the studies was 0%-16%. The overall weighted mean reoperation rate was 5.6%.Table 2. Rates and reasons for revision and reoperations in included studies.StudyFollow-up period in years (range)Revisions (%)Reason for revisionReoperations (%)Reason for reoperationJacquet et al.2020 [24]20 (14-27)23 (9.9%)Cup-7 for AL-6 for PE wearBoth implants-3 for AL-7 for infection12 (5.2%)4 infections3 symptomatic HO1 PP femur fracture1 liner dislocation1 painful trochanteric wire 1 GT fracture non-union1 dislocation16 (10-22)6 (23.1%)Cup-2 for dislocation-1 for ALStem-for PP fracture-2 for AL1 (3.8%)1 PP femur fractureFlecher et al.2018 [25]15 (9-22)1 (4.35%)Stem-1 for AL2 (8.7%)1 infection1 head fracturePakos et al.2015 [35]10.68 (9.30%)Cup-3 for AL-1 for PE liner wearStem-2 for ALBoth implants-2 for infection3 (3.5%)2 dislocations1 HOAkbar et al.2009 [26]14 (10-16)3 (4.17%)Cup-3 for ALNot statedNot statedFlecher et al.2007 [27]10.25 (83-182)6 (6.2%)Cup-2 for AL-2 for dislocationStem-1 for stem fractureBoth implants-1 for infection1 (1.0%)1 dislocationAl-Khateeb et al.2014 [28]10.1 (5-15)3 (21%)Cup-3 for AL2 (13.3%)1 symptomatic HO 1 infectionKoulouvaris et al.2008 [29]6 (4-8)3 (6.25)Cup-1 for mechanical failureBoth implants-2 for infection2 (4.2%)1 dislocation1 symptomatic HOBenum et al.2010 [33]102 (2.41%)Stem-2 for PP fracture7 (8.4%)1 PP femur fracture4 PE wear 2 painSakai et al.2006 [17]9.251 (1.01%)Stem-1 for ALNot stated-Not statedSewell et al.2011 [30]10.1 (4.3-18.2)4 (10%)Cup-2 for ALStem-1 for infectionBoth implants-1 for AL4 (16%)1 dislocation2 intraoperative fracture1 infectionMcCullough et al.2006 [31]11.2 (8-13)4 (9.5%)Cup-2 for ALStem-2 for AL6 (14.3%)1 stem subsidence4 exchange PE line1 PP fractureKawate et al.2009 [34]7 (5-11)001 (1.8%)1 dislocationMasuda et al.2016 [32]13 (10-19)--3 (9.38%)3 dislocationAL, aseptic loosening; GT, greater trochanter; HO, heterotopic ossification; PE, polyethylene; PP, periprosthetic.
Eleven studies (N = 780) presented their revision rates (Table 2). At a mean follow-up of 11.5 years, the overall mean revision rate for custom femoral THA prostheses was 8.25% (95% CI: 4.02-12.47). The range of revision rates in the studies was 0%-23.10%. The overall weighted mean revision rate was 7.0%.
Kaplan–Meier survival was reported in 11 studies (Table 3). Stem survival with aseptic loosening as an endpoint was reported in 11 studies (N = 869). Eight studies (N = 488) [[26], [27], [28], [29],[32], [33], [34], [35]] reported this as 100% with a follow-up ranging from 6 to 14 years. Three studies (n = 381) [17,24,25] reported survival of 87.5%-99%, with a follow-up ranging from 9.3 to 20 years.Table 3. Kaplan–Meir survival data for included studies.StudyStem revision for aseptic looseningRevision of any component for any reasonFollow-up yearsKM survival (95% CI)Follow-up yearsKM survival (95% CI)Jacquet et al.2020 [24]2096.8% (95.1-98.5)2077.7% (72.4-84)1587.5% (76.5-99.1)1572.60%Flecher et al.2018 [25]1595.6% (92.4-98.8)Not statedNot statedPakos et al.2015 [35]10100%1095.4%%Akbar et al.2009 [26]14100%1486% (64-95)Flecher et al.2007 [27]13100%1389.5% (89.2-89.8)Al-Khateeb et al.2014 [28]10.1100%10.179%Koulouvaris et al.2008 [29]6100%Not statedNot statedBenum et al.2010 [33]10100%Not statedNot statedSakai et al.2006 [17]9.399% (0.97-1)9.399% (0.97-1)Sewell et al.2011 [30]Not statedNot statedNot statedNot statedMcCullough et al.2006 [31]Not statedNot stated1271.4%Kawate et al.2009 [34]7100%Not statedNot statedMasuda et al.2016 [32]13100%Not statedNot statedCI, confidence interval; KM, Kaplan–Meir.
Intraoperative fractures and leg-length discrepancy
Intraoperative fracture rates were reported in 11 studies (N = 595) with a mean rate of 3.23% (95% CI: 1.35-5.11). The overall weighted mean was 3.19%. All cases of intraoperative fractures were treated with cabling, except one which required no intervention.
Leg-length discrepancies postoperatively were reported in 5 studies with a mean discrepancy of 4.25 mm (95% CI: 1.57-6.93). The overall weighted mean was 3.08 mm.
Postoperative patient-reported outcomes
All studies included patient-reported outcomes. Ten studies reported their outcomes using Harris Hip Score (HHS; Figure 3) [36], 4 studies presented Merle D’Aubigne scores [37], and one study presented Hospital for Special Surgery system scores [38]. There were insufficient data to permit meta-analysis with studies not reporting inter-quartile range or standard deviation values for specific timepoints. The mean preoperative HHS was 47.26 (range 41-59), and postoperative HHS was 87.58 (range 80-98). The mean improvement in HHS was 40.32 (30-56). The mean preoperative Merle D’Aubigne score was 9 (range 7.6-10), and postoperatively the mean score was 16.63 (range 15.9-17). The one study presenting the hospital for special surgery system score showed an improvement from a median 14 preoperatively to a median 30 postoperatively.Figure 3. Graph illustrating mean preoperative and postoperative Harris Hip Scores.
Quality of evidence
The Joanna Briggs Institute score, reflecting the quality of evidence, indicated a mean score of 6.08 points out of a maximum of 10, with a range of 3 to 9 points (Table 4). Consistently reported strengths in the literature included clearly reported follow-up results of cases (N = 12; 92.3% studies), clear criteria for inclusion in the case series (N = 11; 84.6% studies), and clear reporting of the study participants’ demographics (N = 12; 92.3% studies). Repeated limitations in the evidence included insufficient methods used for identification of the condition for all participants included (N = 11; 84.6% studies) and the condition was not measured in a standard and reliable way for all participants included (N = 9; 69.2% studies)Table 4. Illustrating Joanna Briggs Institute (JBI) Checklist Score and study type.StudyJBI checklist scoreJacquet et al.2020 [24]6 (non-comparative, retrospective)Flecher et al.2018 [25]4 (non-comparative, retrospective)Flecher et al.2018 [25]7 (non-comparative, retrospective)Pakos et al.2015 [35]8 (non-comparative, prospective)Akbar et al.2009 [26]8 (non-comparative)Flecher et al.2007 [27]7 (non-comparative, retrospective)Al-Khateeb et al.2014 [28]9 (non-comparative, prospective)Koulouvaris et al.2008 [29]0 (non-comparative, prospective)Benum et al.2010 [33]8 (non-comparative, prospective)Sakai et al.2006 [17]7 (non-comparative, retrospective)Sewell et al.2011 [30]5 (non-comparative)McCullough et al.2006 [31]7 (non-comparative)Kawate et al.2009 [34]3 (non-comparative, retrospective)
Discussion
Custom femoral stems offer tailored solutions for deformed proximal femurs, optimizing fixation for unique anatomical challenges. However, their use has limitations, requiring a balanced consideration of benefits against potential challenges in clinical practice. The findings of this systematic review indicate the impressive performance of custom femoral stems in complex patient groups, where achieving durable fixation in abnormal proximal femoral bone is a concern [39,40]. These custom stems demonstrate excellent survival rates against aseptic loosening, with figures ranging from 87.5% to 100% over follow-up periods of 6-20 years. Multiple studies have emphasized that custom femoral stems excel in achieving enhanced metaphyseal fit and fill, a critical factor in boosting both rotational and axial stability [18,41]. The integration of computer-aided design and manufacturing technologies in crafting these stems has been instrumental in achieving this [42,43]. This approach not only preserves bone mass but also optimizes load distribution across the hip joint, characteristics vital for femoral stems, particularly in complex clinical scenarios [42,44]. While the overall survival rate for all components (considering any cause) is somewhat lower, it remains promising in a challenging patient demographic. Notably, most revisions were related to acetabular issues such as loosening and wear, underscoring known challenges with acetabular fixation and durability in these patients [45,46]. The relatively fewer revisions pertaining solely to the femoral component are reassuring.
Custom femoral stems are designed to achieve optimal fit and fill in the metaphyseal region. This is particularly significant in patients with atypical proximal femoral anatomy, who may also present with abnormal bone quality. Such scenarios inherently raise the possibility of intraoperative challenges, including the risk of fractures and potential discrepancies in limb length, should the custom femoral stem not fit as intended [25,47]. Encouragingly, the incidence of intraoperative fractures in custom stems has been reported to be low, even falling below the reported rate of up to 5% for cementless stems in primary THA [[48], [49], [50]]. This is a noteworthy achievement, considering the complexity of cases involving custom stems. Furthermore, the rates of postoperative leg-length discrepancy with custom stems have also been low. When contrasted with the average discrepancies reported in the literature, which range from 3 to 17 mm, the precision achieved with custom stems is commendable [51]. This suggests that with meticulous surgical planning and technique, the risks typically associated with custom stem implantation, such as intraoperative fractures and leg-length discrepancies, can be effectively mitigated while adequately replicating center of rotation of the femoral head, thereby avoiding impingement and reproducing the original foot progression angle [52,53]. These findings underscore the importance of careful preoperative assessment and planning in ensuring successful outcomes with custom femoral stems in THA.
Custom femoral stem manufacturing has evolved over the past 3 decades, shifting from intraoperative silicone mold crafting to preoperative design using radiographs and 3-D imaging. Manufacturers differ in their approach; some modify off-the-shelf models, while others use detailed imaging for a precise anatomical fit. These stems vary in dimensions, shapes, and materials, reflecting diverse manufacturing practices and necessitating treating each stem as a unique, patient-specific implant. This variability challenges standard classification and comparison, as noted in a previous systematic review [54]. Custom stems, designed based on individual patient anatomy and surgeon preferences, offer unique surgical solutions but face challenges like higher costs and extensive preoperative planning [55,56]. Advancements in technologies such as computer-aided design and manufacturing and 3-D printing are revolutionizing the manufacturing of custom stems, by making the process more efficient and cost-effective. Although the initial cost of these advanced manufacturing techniques might be higher, this could be offset by reduced risk of revision. These techniques offer enhanced precision and customization, which enable surgeons to provide more tailored and patient-specific solutions, particularly in complex cases where standard implants may not be adequate. As we continue to embrace these innovations, the future of hip replacement surgery looks to offer more personalized treatment options in order to significantly improve patient outcomes and satisfaction.
This review highlights that existing research lacks direct comparative studies between custom and standard femoral stems in secondary hip osteoarthritis, limiting understanding of custom designs' benefits in complex scenarios. The decision to utilize a custom femoral stem requires deep knowledge of patient anatomy, standard implant limitations, and custom design benefits and challenges. Expertise in preoperative planning and intraoperative techniques is crucial to reduce complications. Current comparative studies show no significant differences, indicating a need for more robust comparative research involving larger cohorts [18,20,21,[57], [58], [59]]. Future studies should include long-term follow-ups to assess custom stems' performance, durability, and effectiveness in mimicking natural biomechanics.
Limitations
Our review is not without limitations. The potential for publication bias, the heterogeneity of the included studies, and the variability in methodologies, follow-up periods, and patient demographics across studies may affect the generalizability of our conclusions. Furthermore, there is variability in the design and manufacturing of custom femoral stems that cannot be controlled and may result in a difference of outcomes. Data for each included study were not available, so a meta-analysis of the postoperative patient-reported outcomes could not be performed.
Conclusions
In conclusion, custom femoral stems in primary THA for secondary hip osteoarthritis offer a potentially accurate and reliable solution that can significantly improve patient outcomes. However, their use requires careful consideration of the individual patient’s anatomy, surgical expertise, and the challenges associated with a custom implant design and manufacturing. Future research should aim to directly compare results and cost-effectiveness of custom and standard femoral stems and provide more robust evidence to guide clinical practice. As orthopedic surgery continues to evolve, the quest for optimal solutions in complex primary THA will undoubtedly fuel ongoing research and innovation.
Conflicts of interest
The authors declare there are no conflicts of interest.
For full disclosure statements refer to https://doi.org/10.1016/j.artd.2024.101504.
CRediT authorship contribution statement
Kevin Ilo: Writing – review & editing, Writing – original draft, Formal analysis, Conceptualization. Prith Hallikeri: Writing – original draft, Data curation. Habillan Naathan: Data curation. Bernard Van Duren: Writing – review & editing, Writing – original draft, Formal analysis. Mark Higgins: Writing – review & editing. Iain McNamara: Writing – review & editing. Toby Smith: Writing – review & editing, Writing – original draft, Formal analysis, Conceptualization.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Mc Auley J.P.Szuszczewicz E.S.Young A.Engh C.A.Sr.Total hip arthroplasty in patients 50 years and younger Clin Orthop Relat Res 200411912510.1097/00003086-200401000-0001915043102 · doi ↗ · pubmed ↗
- 2Adelani M.A.Keeney J.A.Palisch A.Fowler S.A.Clohisy J.C.Has total hip arthroplasty in patients 30 years or younger improved? A systematic review Clin Orthop Relat Res 4712013259526012356436310.1007/s 11999-013-2975-x PMC 3705054 · doi ↗ · pubmed ↗
- 3Boisgard S.Descamps S.Bouillet B.Complex primary total hip arthroplasty Orthop Traumatol Surg Res 991 Suppl 2013 S 34S 422337596010.1016/j.otsr.2012.11.008 · doi ↗ · pubmed ↗
- 4Morley J.R.Barker R.Howell J.R.Cemented total hip replacement Bentley G.European surgical orthopaedics and traumatology: the EFORT textbook 2014 Springer Berlin Heidelberg Berlin, Heidelberg 23972422
- 5Murray D.W.Cemented femoral fixation: the North Atlantic divide Bone Joint J 95-B 11 Suppl A 201351522418735210.1302/0301-620X.95B 11.32976 · doi ↗ · pubmed ↗
- 6Wyatt M.Hooper G.Frampton C.Rothwell A.Survival outcomes of cemented compared to uncemented stems in primary total hip replacement World J Orthop 520145915962540508710.5312/wjo.v 5.i 5.591PMC 4133466 · doi ↗ · pubmed ↗
- 7Bloch B.V.White J.J.E.Matar H.E.Berber R.Manktelow A.R.J.Should patient age thresholds dictate fixation strategy in total hip arthroplasty?Bone Joint J 104-B 20222062113509458010.1302/0301-620X.104B 2.BJJ-2021-1199.R 1 · doi ↗ · pubmed ↗
- 8Jain S.Lamb J.Townsend O.Scott C.E.H.Kendrick B.Middleton R.Risk factors influencing fracture characteristics in postoperative periprosthetic femoral fractures around cemented stems in total hip arthroplasty : a multicentre observational cohort study on 584 fractures Bone Jt Open 220214664753423345510.1302/2633-1462.27.BJO-2021-0027.R 1PMC 8325979 · doi ↗ · pubmed ↗