Spontaneous closure of a macular hole in an unusually long time after primary vitrectomy
Julio Daniel Grigera, Tomás Castro Feijóo, Alberto D. Zambrano

TL;DR
A man's macular hole spontaneously closed 36 months after initial surgery, leading to improved vision over time.
Contribution
Reports a rare case of delayed spontaneous macular hole closure after vitrectomy.
Findings
Macular hole closed spontaneously 36 months after initial surgery.
Visual acuity improved to 20/25 over 22 months post-closure.
Ellipsoid zone gap decreased over time.
Abstract
We report the case of a 68-year-old man who presented to our outpatient clinic for routine examination. Fifteen months before, he had undergone combined cataract and idiopathic full-thickness macular hole surgery in his right eye at another institution. In the present evaluation, the best-corrected visual acuity in his right eye was counting fingers. Fundus examination evidenced an idiopathic full-thickness macular hole in that eye, which was confirmed on spectral domain optical coherence tomography. A new surgery was offered, but the patient declined. Twenty-one months after his first consultation with us (36 months after the surgery), spectral domain optical coherence tomography revealed spontaneous closure of the idiopathic fullthickness macular hole, with a gap at the foveal ellipsoid zone. At the final visit, 22 months after the closure of the idiopathic full-thickness macular…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
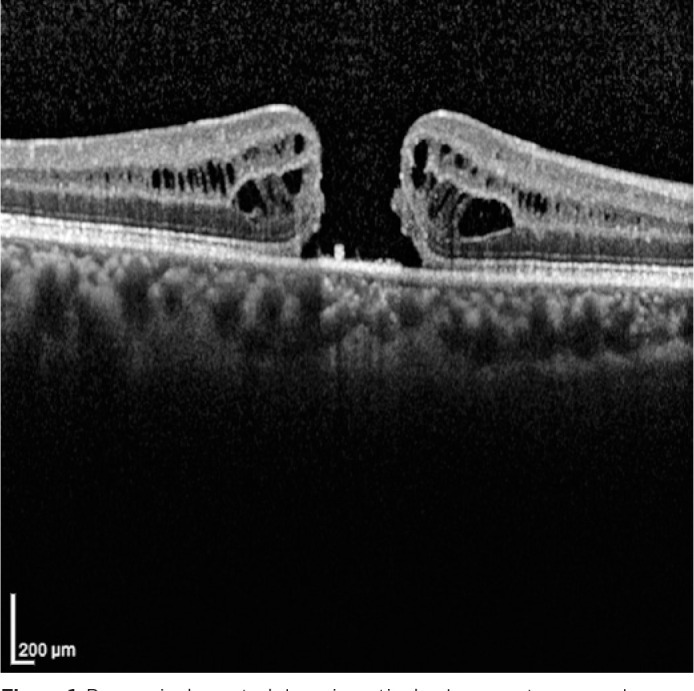 Figure 1
Figure 1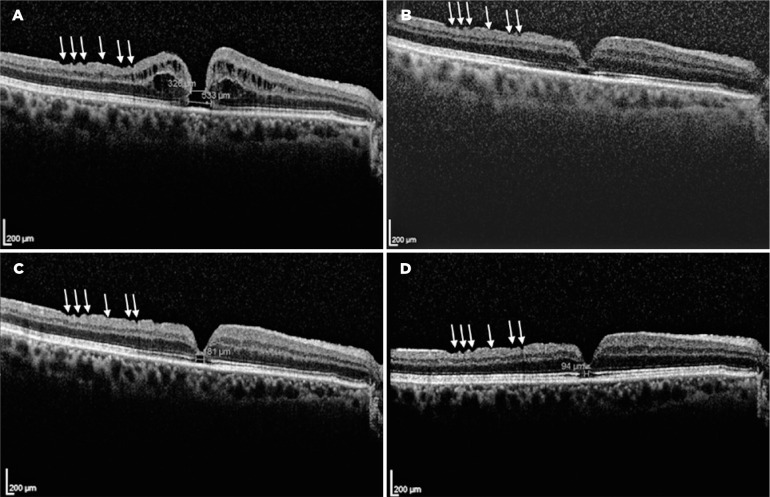 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsRetinal and Macular Surgery · Intraocular Surgery and Lenses · Glaucoma and retinal disorders
INTRODUCTION
An idiopathic full-thickness macular hole (iFTMH) is an opening of the whole retina at the fovea^(1)^. Vitrectomy with internal limiting membrane (ILM) peeling may achieve a nearly 100%-hole closure rate by the end of the first postoperative week^(2)^. We report a case of spontaneous closure of an iFTMH 36 months after the primary vitrectomy and its 22-month follow-up results.
CASE REPORT
A 68-year-old man who had undergone combined cataract and iFTMH surgery in his right eye (OD) 15 months before at another institution presented at our outpatient clinic for routine examination. The best-corrected visual acuity (BCVA) in OD was counting fingers, with pseudophakia and normal intraocular pressure. Fundus examination evidenced an iFTMH in the right eye; the left eye showed no abnormal findings. The patient’s presurgical spectral domain optical coherence tomography (SD-OCT) study demonstrated a FTMH, but the iFTMH was not measured (Figure 1). A new SD- OCT scan revealed the persistence of the iFTMH, with 326 and 533 microns of midand base-hole diameters, respectively (Figure 2A). A new surgery was offered, but the patient declined. Thus, he was set for follow-up every 6 months.
Figure 1. Presurgical spectral domain optical coherence tomography scan showing the idiopathic full-thickness macular hole.
Figure 2. Postsurgical spectral domain optical coherence tomography scans. The idiopathic full-thickness macular hole (iFTMH) persisted for 15 months after primary vitrectomy (A). Its midand base-hole diameters were of 326 and 533 microns, respectively. The best-corrected visual acuity (BCVA) was counting fingers. iFTMH closure was verified 36 months after surgery (B). Posterior capsular opacification precluded obtaining a clear image, and the BCVA was 20/200. This improved when posterior capsulotomy was performed 12 months after (C). A 181-micron gap at the foveal ellipsoid zone was present, and the BCVA was 20/30. At the last visit, 22 months after the iFTMH closure (D), a 94-micron gap at the EZ remained. The corresponding BCVA was 20/25. The inner retinal dimples (white arrows) can be observed on the temporal side of the macular retinal nerve fiber layer.
Twenty-one months after his first consultation with us (36 months after the surgery), the BCVA in the right eye had improved to 20/200. Slit-lamp examination revealed posterior capsule opacification while fundus examination and SD-OCT revealed the spontaneous closure of the iFTMH (Figure 2B), with a gap at the foveal ellipsoid zone (EZ).
Twelve months after the verified closure of the iFTMH, posterior capsulotomy was performed, and the BCVA improved to 20/30. At the final visit, 22 months after the closure of the iFTMH, the patient’s BCVA was 20/25, and the gap at the EZ diminished its diameter from 181 microns (Figure 2C) to 94 microns (Figure 2D).
DISCUSSION
We report a case of spontaneous closure of an iFTMH 36 months after an unsuccessful primary vitrectomy. To the best of our knowledge, this is the longest time elapsed between primary vitrectomy and closure of the iFTMH reported in the literature.
Odrobina et al.^(3)^, Afrashi^(4)^, and Patel et al.^(5)^ published case reports of spontaneous delayed closure of new iFTMHs 1, 5, and 28 months after vitrectomy for vitreomacular traction, respectively. The ILM was peeled in the first case; however, in the second case, it was dissected but not removed because of alleged tight adhesions at the macula. By contrast, in the latter, ILM peeling was not even attempted.
Two case reports by Falkner-Radler et al.^(6)^ and Lee et al.^(7)^ demonstrated the late spontaneous closure of a pre-existing iFTMH 9 months after unsuccessful vitrectomy, both with ILM peeling and C_3_F_8_ gas tamponade. The closure of the latter was associated with the development of a type 1 neovascular membrane that apparently brought together the retinal tissue.
Rishi et al.^(8,9)^ reported 2 cases of spontaneous closure of traumatic macular holes 7 months after vitrectomy with ILM peeling and gas tamponade. One of the cases^(9)^ was associated with submacular hemorrhage. The authors presumed that physical approximation of the hole edges could have been facilitated by submacular blood removal. They affirmed that a dynamic process occurring at the macula long after the surgery may be responsible for the change in configuration of the macular hole. None of the cited papers explained the long time elapsed before the hole closure.
A pre-existing iFTMH was the primary reason for the surgery in our patient. We did not have access to the preoperative clinical records, but ILM peeling was assumed to be performed owing to the presence of superficial focal retinal depressions known as inner retinal dimples (Figure 2, white arrows), which are supposed to be due to diffuse loss of the Müller cell end-feet and whose presence is considered a late sign of an already peeled ILM^(10)^. The preoperative SD-OCT study result brought to us by the patient was from another clinic, and unfortunately, the iFTMH was not measured. Thus, the presurgical and postsurgical iFTMH sizes could not be compared.
For personal reasons, our patient chose not to undergo another surgery. Although prospective studies are lacking, the current retrospective evidence holds that 71% to 84% of iFTMHs close with a secondary procedure. This may be achieved with different techniques, but the available evidence does not show superiority of one procedure over the others^(11)^.
Sokol et al.^(12)^ presented a multicenter, retrospective observational case series of 14 patients who underwent successful off-label topical treatment with steroids, nonsteroidal anti-inflammatory drugs, and carbonic anhydrase inhibitors for closure of iFTMHs. They suggested that this treatment could trigger both decreased inflammation and increased fluid absorption through the retinal pigment epithelium, thereby closing the hole.
However, the possibility that treated iFTMHs could have closed spontaneously without treatment must be considered. This study has no arm for comparison or data on treated patients whose holes did not close. Hence, further investigation is needed.
When the iFTMH closed spontaneously and the BCVA improved to 20/200, capsular opacification from the original combined procedure precluded further visual improvement for 12 months, until capsulotomy was performed. The facts that EZ gradually regenerated up to a 94-micron gap and that BCVA improved to 20/25 at the last follow-up visit are consistent with the evidence of long-term postoperative vision improvement associated with the restoration of the morphological features of the outer retinal layers^(13)^.
Bringmann et al.^(14)^ previously hypothesized that the mechanism of spontaneous iFTMH closure is likely mediated by an annular contraction of the horizontal Müller cell side processes in the foveal outer plexiform layer (OPL) and the Müller cell structures that envelop the photoreceptor cells at the external limiting membrane. These movements result in a centripetal shift of the foveal walls and the closure of the hole at the level of the OPL/inner part of the outer nuclear layer (ONL). After the closure of the hole, the EZ regenerates, possibly due to a centripetal displacement of the photoreceptor cells around the EZ defect and/or an outgrowth of the newly formed photoreceptor segments from the photoreceptor cell somata in the central ONL.
In conclusion, we report the unusual occurrence of delayed spontaneous closure of an iFTMH. Through the 22-month follow-up after the iFTMH closure, anatomical and functional improvements were detected. When the patient rejects a secondary procedure, it could be acceptable to assess the macula with serial OCTs scans considering the possibility of spontaneous delayed closure and anatomical regeneration of the EZ.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Ho AC Guyer DR Fine SL. Macular hole Surv Ophthalmol 199842393416954857010.1016/s 0039-6257(97)00132-x · doi ↗ · pubmed ↗
- 2Chow DR Chaudhary KM. Optical coherence tomographybased positioning regimen for macular hole surgery Retina 20153558999072560263210.1097/IAE.0000000000000410 · doi ↗ · pubmed ↗
- 3Odrobina D Laudańska-Olszewska I Gozdek P Maroszyński M Amon M. Macular hole formation and spontaneous closure after vitrectomy for vitreomacular traction documented in spectral-domain optical coherence tomography BMC Ophthalmol 201414172455216110.1186/1471-2415-14-17PMC 3931271 · doi ↗ · pubmed ↗
- 4Afrashi F Öztas Z NalçacıS. Late closure of a stage III idiopathic macular hole after pars plana vitrectomy Turk J Ophthalmol 20154562742762780024810.4274/tjo.33603 PMC 5082268 · doi ↗ · pubmed ↗
- 5Patel R Gopalakrishnan M Rajesh B Giridhar A. Postvitrectomy macular hole undergoing delayed closure after 28 months Indian J Ophthalmol 20176598828842890583910.4103/ijo.IJO_426_17PMC 5621278 · doi ↗ · pubmed ↗
- 6Falkner-Radler CI Gabriel M Binder S. Spontaneous closure of an idiopathic macular hole 9 months after unsuccessful vitreoretinal surgery Retin Cases Brief Rep 2014831571602537242710.1097/ICB.0000000000000030 · doi ↗ · pubmed ↗
- 7Lee J Nguyen VQ Doss MK Eller AW. Spontaneous closure of a chronic full thickness macular hole after failed surgery Am J Ophthalmol Case Rep 20181359613058207310.1016/j.ajoc.2018.12.006PMC 6292999 · doi ↗ · pubmed ↗
- 8Rishi P Kothari A. Delayed, spontaneous conversion of type 2 closure to type 1 closure following surgery for traumatic and idiopathic macular holes Retin Cases Brief Rep 2009321771792539106810.1097/ICB.0b 013e 3181607 a 39 · doi ↗ · pubmed ↗