Subfoveal perfluorocarbon liquid removal by peeling of internal limiting membrane, without retinotomy
Fernanda Silvestre, Gabriela Silvestre, Rodrigo Pessoa Cavalcanti Lira

TL;DR
A 43-year-old woman had subfoveal perfluorocarbon liquid removed without retinotomy by peeling the internal limiting membrane.
Contribution
A novel method for removing subfoveal perfluorocarbon liquid without retinotomy is described.
Findings
Subfoveal perfluorocarbon liquid can be removed using internal limiting membrane peeling.
The procedure avoided retinotomy and preserved retinal structure.
The method offers a potential alternative for treating subretinal retention.
Abstract
Perfluorocarbon liquid has been widely used during vitreoretinal operations. Subretinal retention is a rare intraoperative complication, but even small quantities can damage the macular structure and function, and no standard treatment has been established. We encountered a 43-year-old woman who presented a retained subfoveal bubble after a vitreoretinal operation due to primary rhegmatogenous retinal detachment. Herein, we describe the procedure we used to remove the perfluorocarbon liquid without retinotomy using internal limiting membrane peeling.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
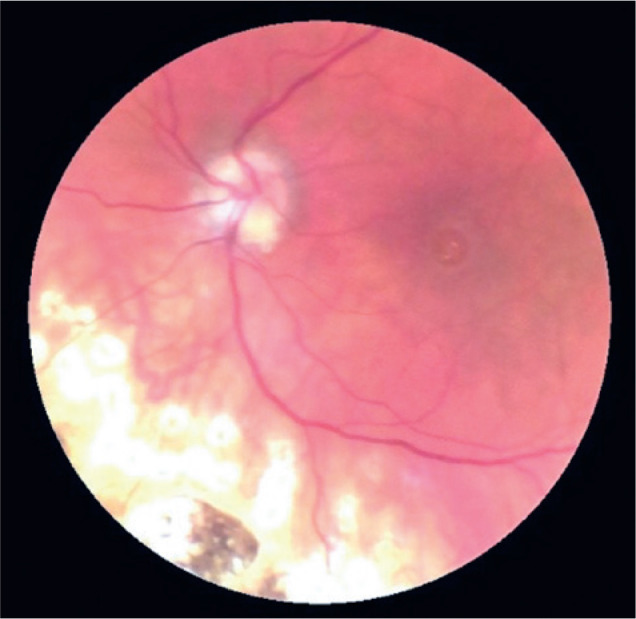 Figure 1
Figure 1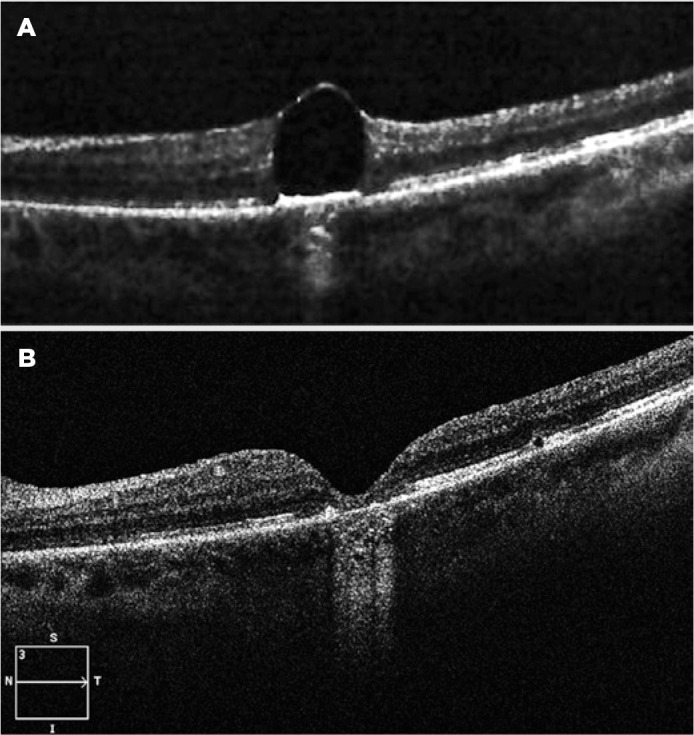 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsRetinal and Macular Surgery · Retinopathy of Prematurity Studies · Retinal Diseases and Treatments
INTRODUCTION
Perfluorocarbon liquid (PFCL) has been widely used during vitreoretinal operations^(1)^. Subretinal PFCL retention is a rare intraoperative complication, but even small quantities can damage the macula^(2)^. Visual acuity may improve following removal or displacement of subfoveal PFCL^(2)^. No standard method to treat this complication has been established. Subfoveal PFCL can be aspirated directly by retinotomy using a small gauge needle at the edge of^(3)^ or above^(4)^ the PFCL bubble. Other options include displacing the PFCL to the outside of the subfoveal space, followed by removal^(5)^ or displacement without removal^(6)^. Herein, we removed the subfoveal PFCL without retinotomy using only internal limiting membrane (ILM) peeling.
CASE REPORT
A 43-year-old woman was seen in August 2017 with a suspected macular hole in her left eye (LE). Two months before that, her vision in that eye had deteriorated due to macula-off retinal detachment with an inferior retinal tear. Vitrectomy, PFCL injection, endolaser, and fluid-gas exchange had been performed in another institute. Her medical history included systemic arterial hypertension, bilateral optic disc drusen, bilateral LASIK surgery in 2011 (myopia of 6 diopters in both eyes), bilateral cataract surgery with insertion of intraocular lenses in 2013, YAG laser capsulotomy in 2014, and posterior vitreous detachment in 2016. The best-corrected visual acuity of the LE was 0.05, with metamorphopsia and central scotoma in the Amsler grid. Biomicroscopy, color vision test, and tonometry were all normal. We identified photocoagulation marks up to the lower border of the eye, slight pallor of the papilla, and a macular pseudo-hole due to a retained subfoveal PFCL bubble by ophthalmoscopy (Figure 1), although Watzke-Allen and laser aiming beam tests were positive. Optical coherence tomography (OCT) confirmed the diagnosis (Figure 2A).
Figure 1. Photograph showing the fundus of the left eye with a macular pseudo-hole due to a retained subfoveal PFCL bubble.
Figure 2. Preoperative and postoperative optical coherence tomography (OCT) demonstrating the removal of the subfoveal perfluorocarbon liquid (PFCL). A) Retained subfoveal PFCL bubble. B) Thinning, gliosis, and disruption of the external retinal layers in the foveal region on postoperative OCT.
The patient was scheduled to undergo a 25-gauge pars plana vitrectomy (Alcon Constellation Vision System, Fort Worth, Texas, USA). The surgeon stained the retinal surface with brilliant blue (Opht-Blue, Ophthalmos Rohto, São Paulo, Brazil), and removed the ILM in the foveal and temporal juxtafoveal region using forceps (Grieshaber^®^ asymmetrical forceps, Forth Worth, Texas, USA). The subfoveal PFCL bubble migrated spontaneously to the vitreous cavity through the foveal area where the ILM had been removed. The surgeon then aspirated the PFCL using a 41-gauge cannula (DORC, Zuidland, The Netherlands), and performed fluid-air exchange with 15% sulphur hexafluoride (SF_6_) gas tamponade. The patient was instructed to remain face down for a week. Six months following the operation, the patient’s visual acuity was 0.2, without metamorphopsia or central scotoma. Postoperative fundoscopy and OCT showed no macular holes; however, thinning, gliosis, and disruption of the external retinal layers in the foveal region were apparent (Figure 2B).
DISCUSSION
We describe the case of a patient with retained subfoveal PFCL treated surgically by ILM removal without retinotomy. Her visual acuity improved; however, the visual prognosis was limited by characteristics associated with the previous retinal detachment surgery, and the location, size, and duration of the subfoveal PFCL. Moreover, we cannot rule out the possibility of an iatrogenic lesion during the removal^(2)^. However, real-time intraoperative OCT could render this surgical technique safer.
Direct surgical aspirations through a foveal or juxtafoveal retinotomy at the edge of the PFCL bubble have already been attempted, with varying results^(3,4)^. However, this procedure can cause sight-threatening complications, including macular holes, submacular hemorrhages, enlargement of the juxtafoveal retinotomy, or damage to the macular photoreceptor or retinal pigment epithelia. Because of these potential complications, a temporary retinal detachment was developed as a means of dis placing the retained subfoveal PFCLs^(5,6)^.
Our technique provides several advantages. The ILM covering the PFCL bubble is removed, leaving virtually no lesions or additional tissue losses; moreover, no macular retinal detachment or any additional damage to perifoveal photoreceptors are needed. Finally, this method is relatively simple to perform, requiring no special subretinal instruments.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Chang S Ozmert E Zimmermann NJ. Intraoperative perfluorocarbon liquids in the management of proliferative vitreoretinopathy Am J Ophthalmol 19881066668674319564610.1016/0002-9394(88)90698-8 · doi ↗ · pubmed ↗
- 2Liu W Gao M Liang X. Management of subfoveal perfluorocarbon liquid: a review Ophthalmologica 20182401172966935510.1159/000488118 · doi ↗ · pubmed ↗
- 3Joondeph BC. Controlled aspiration of subfoveal perfluorocarbon liquid using a novel microcannula Retina 20113159919932148733210.1097/IAE.0b 013e 3182150565 · doi ↗ · pubmed ↗
- 4De CillàS Alkabes M Radice P Carini E Mateo C. Direct transretinal removal of subfoveal perfluorocarbon liquid: the role and timing of internal limiting membrane peeling Eur J Ophthalmol 20172722492522812773610.5301/ejo.5000934 · doi ↗ · pubmed ↗
- 5Sierra-Rodríguez MA López-López JM Jiménez-Prada de Miguel S Subfoveal perfluorocarbon liquid. Removal after three months Arch Soc Esp Oftalmol 201691125965982700592010.1016/j.oftal.2016.02.004 · doi ↗ · pubmed ↗
- 6Le Tien V Pierre-Kahn V Azan F Renard G Chauvaud D. Displacement of retained subfoveal perfluorocarbon liquid after vitreoretinal surgery Arch Ophthalmol 20081261981011819522510.1001/archophthalmol.2007.2 · doi ↗ · pubmed ↗