Gas tamponade followed by laser treatment for macular retinal detachment secondary to optic pit
Leandro Chaves, Julian Costa, Thaís Bastos, Marina Albuquerque, Ingrid Scott, Rodrigo Jorge

TL;DR
This study shows that injecting gas into the eye followed by laser treatment can help treat a type of retinal detachment caused by an optic pit.
Contribution
The study introduces a new treatment approach combining gas injection and laser for optic pit-associated macular detachment.
Findings
Five out of six patients showed complete fluid resolution without recurrence.
One patient required an additional procedure for full recovery.
Visual acuity improved in all patients after the treatment.
Abstract
The study aimed to describe anatomic and visual outcomes associated with perfluoropropane intravitreal injection followed by laser treatment for macular retinal detachment secondary to optic disc pit. A single-center, retrospective study. Medical records of all patients treated at a tertiary retina referral center were evaluated between 2011 and 2018 for congenital optic disc pit-associated macular detachment with 0.3 ml 100% perfluoropropane intravitreal injection followed by retinal laser photocoagulation along the temporal optic disc margin as the initial treatment. Six patients with optic disc pit-associated macular detachment were identified, with postoperative follow-up ranging from 13 to 52 months (mean: 28 months). Spectral domain optical coherence tomography (SD-OCT) showed complete fluid resolution without recurrence in five of the six cases. Four cases showed complete…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
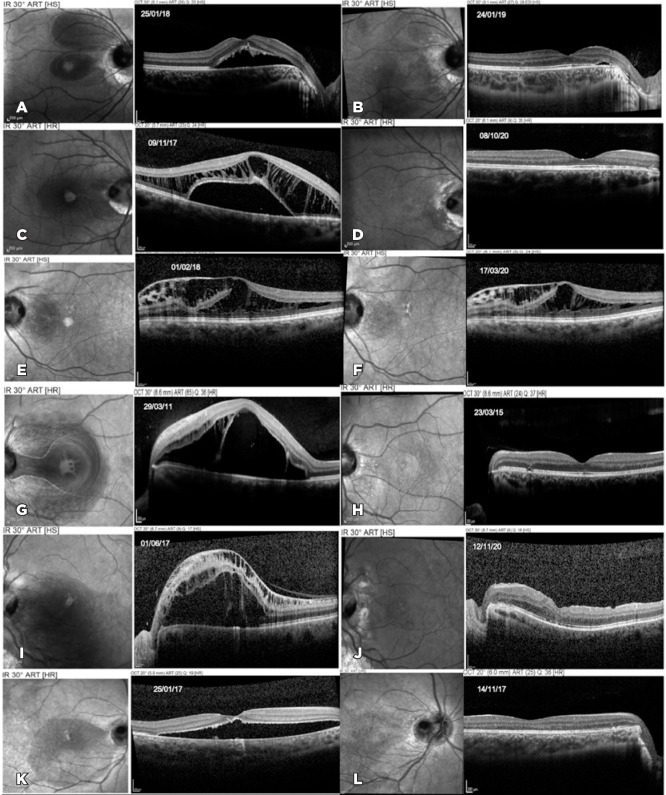 Figure 1
Figure 1| Patient # /gender/age (year)/eye | Symptons duration (month) | Fluid locaction | Retinal layers breaks | Baseline visual acuity | Final visual acuity | LASER section |
|---|---|---|---|---|---|---|
| 1 / M / 10 / RE | 10 | SRF | NO | 20/40 | 20/20 | 2 |
| 2 / F / 14 / RE | 60 | SRF + ONL | OPL+ ONL + ELM + IS/OS + ZI | 20/2.000 | 20/25 | 2 |
| 3 | 24 | NFL + GCL + INL + ONL | NO | 20/80 | 20/32 | 3 |
| 4 / M / 12 / LE | 0,26 | SRF + NFL + GCL + INL + ONL | OPL+ ONL + ELM + IS/OS + ZI | 20/200 | 20/25 | 2 |
| 5 / F / 52 / LE | 1 | SRF + GCL + ONL + INL | OPL+ ONL + ELM + IS/OS + ZI | 20/2.000 | 20/200 | 3 |
| 6 / F / 8 / RE | 1 | SRF | IS/OS + IZ | 20/30 | 20/20 | 1 |
| LASER spots number | Results | Aditional aproach | Carbonic anhydrase inhibitor use | Follow-up (month) |
|---|---|---|---|---|
| 30 | Total fluid reabsorption | NO | NO | 12 |
| 81 | Total fluid reabsorption | NO | YES, eye drops | 19 |
| 38 | Partial reabsorption | NO | YES, sistemic | 25 |
| 36 | Total fluid reabsorption | NO | YES, sistemic | 52 |
| 80 | Total fluid reabsorption | PPV + ILM peeling | YES, sistemic | 47 |
| 53 | Total fluid reabsorption | NO | NO | 13 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsRetinal and Macular Surgery · Vascular Malformations Diagnosis and Treatment · Intraocular Surgery and Lenses
INTRODUCTION
Optic disc pit was first reported in 1882 by Wiethe^(1)^. Optic disc pits (ODP) are a part of cavitary optic disc anomalies set that includes coloboma, morning glory disc, and extrapapillary cavitation^(2)^, characterized by abnormal communication between the intraocular and extraocular spaces. ODPs are extremely rare, without gender predilection, and can be congenital or acquired. The estimated congenital form incidence is 1:11,000 persons. Only 15% of these patients have a bilateral disease, and, in most cases, there is only one pit per disc, with a typical inferotemporal pit location^(3)^. The pits are oval-shaped depressions that are frequently gray but may be yellowish or black^(2,3)^.
Macular involvement was first described in 1927 by Halbertsma^(4)^. ODPs are typically asymptomatic, although as many as 75% of affected patients develop retinal detachment or macular retinoschisis, experiencing an impaired vision, an advanced condition called optic disc pit maculopathy^(3,5)^.
ODP-associated retinal detachment pathophysiology and subretinal fluid etiology are controversial. Two studies have proposed a mechanism of subretinal fluid accumulation, such as its origin from the vitreous cavity and subarachnoid space^(2,3)^. Subretinal fluid biochemical analysis in two patients demonstrated a composition similar to that of cerebrospinal fluid^(6)^. In contrast to the theory proposed by Lincoff et al.^(7)^, which describes retinal schisis presence preceding subretinal fluid accumulation, optic coherence tomography (OCT) studies have demonstrated that retinal schisis does not always exist in patients with ODP-associated retinal detachment^(8)^.
The prognosis of untreated ODP-associated macular detachment varies. Brown et al.^(9)^ followed 20 eyes with untreated optic disc maculopathy for more than one year. The authors showed subretinal fluid persistence in 75% of these cases and last follow-up visual acuity of 20/100 or worse in 55% of cases. Sobol et al.^(10)^ followed 15 eyes with ODP-associated with macular detachment for 9 years and showed that 80% of them had a visual acuity of 20/200 or worse at the last follow-up.
There is no universally accepted effective therapy for ODP-associated macular detachment. Various treatments have been described, including intraocular gas injection only^(11)^, gas injection with laser photocoagulation along the temporal optic disc margin^(12)^, macular buckling^(13)^, pars plana vitrectomy with gas tamponade with or without laser, pars plana vitrectomy with internal limiting membrane peeling with or without a flap^(14)^, platelet-rich autologous serum infusion^(14,15)^, autologous scleral plug^(16)^, and partial inner retinal fenestration^(17)^.
Herein, we report the results of a minimally invasive and low-cost treatment with a combination of 100% perfluoropropane (C3F8) intravitreal injection followed by retinal laser photocoagulation along the temporal optic disc margin as the initial treatment for ODP-associated macular detachment.
METHODS
This study adhered to the tenets of Declaration of Helsinki and was approved by the Research Ethics Committee of Ribeirão Preto School of Medicine - University of São Paulo (CAAE: 32397720.0.0000.5440).
Medical records of patients that were treated at the Hospital das Clínicas da Faculdade de Medicina de Ribeirão Preto - Universidade de São Paulo between 2011 and 2018 for congenital ODP-associated macular detachment with 100% C3F8 intravitreal injection followed by retinal laser photocoagulation along the the temporal optic disc margin as the initial treatment for their ODP-associated macular detachment were reviewed.
Collected data included age at diagnosis, gender, laterality, duration of symptoms, visual acuity on presentation, retinal layers affected on OCT scans, need for retreatment or alternative therapy, visual acuity at last follow-up, the time course of visual acuity improvement, and follow-up duration. The initial treatment was provided by the same surgeon in an ambulatory surgical environment under aseptic conditions and with topical anesthesia. After paracentesis of the anterior chamber, 0.3 ml 100% C3F8 was injected intravitreally, and the patient was instructed to maintain face-down positioning for seven days. Retinal photocoagulation with green diode laser was performed along the temporal optic disc margin three days after C3F8 injection using the following parameters: 50-100 µm spot size with an exposure duration of 50-100 milliseconds and sufficient intensity to achieve visible marks. All patients were treated with 360-degree peripheral retinal laser photocoagulation before C3F8 injection for a theorical retinal detachment prophylaxis.
Green diode laser retinal photocoagulation along the temporal optic disc rim was repeated in five patients 30-70 days after the first procedure. The laser was repeated once the surgeon observed no improvement of the intraretinal and/or subretinal fluid on OCT follow-up. The mean number of laser sessions was 2.2, with a mean number of spots being 53. The laser was repeated at the same spot when the laser burn performed in a previous section was not clearly visible or in an additional row temporal to the previous section to stimulate a healthier retinal pigment epithelium (RPE) to generate a more efficacious chorioretinal adhesion than the previous one.
RESULTS
Six patients with ODP-associated macular detachment during the study period were identified (Table 1), and all these ODP were congenital. Three patients were males, and one had bilateral involvement but consented to treatment only for his left eye. The age at diagnosis ranged from 5 to 52 years, with a mean age of 24.3 years (standard deviation (SD): 20.76). Duration of symptoms ranged from eight days to five years. Mean best-corrected visual acuity (BCVA) at four meters was 20/200 or worse in three cases and 20/40 or better in two.
Table 1: Clinical characteristics of 6 patients with optic disc pit maculopathy, OCT finding, and outcomes
Table 1: Clinical characteristics of 6 patients with optic disc pit maculopathy, OCT finding, and outcomes.
Spectral domain optical coherence tomography (SD-OCT) (Spectralis OCT^®^, Heidelberg Engineering, Heidelberg, Germany) revealed optic disc defect and macular subretinal fluid in all patients. Four patients had intraretinal fluid involving primarily the outer nuclear layer. In three cases, there was fluid in the inner and outer retina. Retinal layer discontinuity was observed in four eyes, all of them involving the inner segment/outer segment (IS/OS) layer, interdigitation zone, and RPE. Involvement of the outer plexiform and outer nuclear layers and the external limiting membrane was observed in three cases (Table 1).
Postoperatively, OCT demonstrated complete fluid resolution in five patients, without recurrence during follow-up (Figure 1). Total reabsorption was documented after 12 months, 13 months, 25 months, and 6.5 months in patients number 1, 2, 4, and 6, respectively. Patient number 5 failed to demonstrate fluid reabsorption on OCT and underwent pars plana vitrectomy, achieving complete fluid resolution 41 months after the initial treatment. Patient number 3 failed to demonstrate progressive fluid reabsorption and refused any additional treatment.
Figure 1. Patients number 1-6: Optical coherence tomography (OCT) before and after treatment. OCT images showing improvement of macular fluid in all six patients. All patients were treated with 0.3 ml 100% C3F8 intravitreal injection followed by retinal photocoagulation along the temporal optic disc margin. Patient 1 (A, B); 2 (C, D), 4 (G, H), and 6 (K, L) showed anatomic improvement and complete resolution of macular fluid after this treatment. Patient 5 (I, J) had fluid recurrence and needed an additional procedure (inner limiting membrane peeling under brilliant blue dye visualization, pedicle flap inversion at the temporal optic disc margin). There was complete resolution of the fluid after this treatment. Patient 3 (E, F) showed a slight improvement of the intraretinal fluid. However, he refused additional treatments and the fluid persisted.
Patient number 5 demonstrated transient anatomical improvement but had subretinal/intraretinal fluid recurrence and underwent 25-gauge pars plana vitrectomy, inner limiting membrane peeling under visualization with brilliant blue dye, inversion of pedicle flap at the temporal optic disc margin, and 15% C3F8 intravitreal injection 5 months after the initial procedure (gas injection followed by photocoagulation).
Four patients received carbonic anhydrase inhibitors during the postoperative period: orally in three cases, (250 mg-1 g per day) and topically (every 8 hours) in the fourth case. The duration of medication use ranged from 30 days to 30 months.
BCVA improved, at least in one line, in all patients. Median BCVA was 20/80 before surgery and improved significantly to 20/32 at last follow-up after intravitreal gas plus laser. Four patients had BCVA of 20/40 or better. The median follow-up duration was 28 months (range: 12-52 months).
DISCUSSION
Using laser alone to treat OPD-associated macular detachment was first reported in 1969 by Gass^(18)^, who used xenon laser to create chorioretinal adhesion at the temporal optic disc margin in an attempt to minimize fluid movement from the pit to the subretinal space in two patients. In 1972, Mustonen and Varonen used argon laser in three patients with the same objective and observed slow subretinal fluid reabsorption^(19)^. Sandali et al. reported a success rate of 30% using laser alone^(20)^. The use of gas was evaluated by Lincoff et al. only in 1998 in three cases. Despite an initial visual acuity improvement, macular fluid recurrence was seen in two cases within 3 months and in the third case during the fifth year of follow-up^(21)^. In our patients, we used intravitreal C3F8 in addition to the laser, in a similar way to previously published studies^(12,20,22-24)^. With proper positioning, the gas bubble exerts pressure on the inner retinal surface and induces passive subretinal fluid migration through the RPE and choroid. Consequently, it reduces the distance between the retinal layers, thus, facilitating photocoagulation and subsequent adhesion between the outer retinal layers and RPE^(2,12,22)^.
Our patients and results are comparable to the published data. Two-thirds of our patients were younger than 14 years, and the mean age of 24.3 years was comparable to Lei et al. (25.8 years) and Elmohamady et al. (22 years)^(22,24)^. Our success rate was 88.3%, which is comparable to previous studies as well, where Sandali et al. reported a success rate of 72%^(20)^; Lei et al. reported a success rate of 75%^(22)^, and Elmohamady et al. reported a success rate of 82%^(24)^.
The duration between C3F8 injection and retinal photocoagulation along the temporal optic disc margin in our patients was three days, in contrast to the study by Lei et al.^(22)^, who applied laser one or two weeks after gas injection, and the study by Elmohamady et al.^(24)^, who applied laser two or three weeks after gas injection. We prefer a shorter period of face-down positioning, which is more convenient for the patient. Another difference in our technique compared to that of Lei et al.^(22)^ was the C3F8 concentration, which was 100% in the present study and 66% in the former. We prefer a higher C3F8 concentration since that usually generates a larger bubble exerting a higher pressure over a greater retinal area; this, in turn, may be associated with more efficient intraretinal and subretinal fluid drainage. Elmohamady et al. had used 0.6 ml of 100% sulfur hexafluoride (SF_6_)^(24)^.
All patients were treated with 360-degree peripheral retinal laser photocoagulation prior to intravitreal C3F8 injection for rhegmatogenous retinal detachment prophylaxis. Although ODP is not related to a higher risk of rhegmatogenous retinal detachment or peripheral retinal abnormalities, we believe that posterior hyaloid detachment, expansion, movements, and mechanical forces triggered by the intraocular gas may generate traction on the peripheral retina, with the risk of retinal tear and detachment, as reported by the DRCR Retina Network^(25)^, where intravitreal perfluoropropane was used for vitreomacular traction with and without macular hole. The prophylaxis might not have been necessary since other similar case series that used gas injection without pars plana vitrectomy to treat optic disc pit maculopathy did not describe rhegmatogenous retinal detachment nor peripheral breaks during the follow-up^(12,20,22,24)^. Fortunately, none of these complications were identified during the follow-up in our study, and no patient developed epiretinal membrane.
An important characteristic of the treatment strategy reported in this study is slow intra- and subretinal fluid resolution. The fastest total reabsorption was observed 6.5 months after the treatment. Visual acuity started to improve concomitantly with the beginning of fluid reabsorption identified on OCT. We believe that careful follow-up of patients who are improving is preferable to administering multiple treatments. In contrast, visual acuity worsening associated with increased intraretinal or subretinal fluid on OCT is an indication for additional treatment, as was the case for patient number 5 (who was treated with pars plana vitrectomy).
Visual acuity improved in all patients in our study. There was no significant association between discontinuity of the retinal layers on OCT or duration of symptoms and visual prognosis.
Progressive fluid reabsorption and the closure of communication between the subretinal and intraretinal spaces with the optic pit occurred in 5 of the 6 cases. Four of them showed anatomic improvement after intravitreal gas injection, face-down positioning, and laser photocoagulation. One of them needed an additional procedure (pars plana vitrectomy, inner limiting membrane peeling under brilliant blue dye visualization, and pedicled flap inversion at the temporal optic disc margin). This patient was the oldest from the study (a 52-year-old woman) and probably had greater vitreous gel liquefaction. We propose two potential explanations for first treatment failure. 1) Even with face-down positioning, there is not enough time for retinal compaction; therefore, the laser may not have a healing effect on all retinal layers. The liquefied vitreous gel may infiltrate the intra- and subretinal space more easily as soon as the patient abandons face-down positioning even for short time intervals. 2) A lower healing capacity of older patients. For this reason, pars plana vitrectomy may be necessary in older patients. During vitrectomy, inner limiting membrane peeling is performed, and a pedicle internal limiting membrane flap is prepared and positioned over the pit in an attempt to prevent fluid entry from the vitreous body into the sub- or intraretinal space. Further, vitrectomy permits the placement of a more voluminous C3F8 bubble, which probably leads to a more effective and long-lasting tamponade of the temporal optic disc margin. This provides a longer healing time after retinal photocoagulation, which may be performed intra- or postoperatively. Some patients with ODP-associated macular detachment are treated only by vitrectomy, without using flaps or endolaser. Those who recommend this technique believe that removal of the hyaloid and prediscal membranes may create a communication between the subarachnoid space and the vitreous cavity, preventing the fluid from that space from migrating toward the retinal tissue.
Carbonic anhydrase inhibitor use varied among patients according to an individualized approach and respecting the tolerance and contraindications for each case. The rationale for this prescription is stimulating the mechanism of fluid pumping outside the subretinal space by RPE cells. Although literature data suggest a theoretical benefit of the carbonic anhydrase inhibitor use in this condition^(26-28)^, the current small case series do not permit an assessment of the potential carbonic anhydrase inhibitors impact on OPD-associated macular detachment.
Clinical examination of patient number 4 showed a possible optic disc pit in the right eye (contralateral eye), which was confirmed on OCT (Figure 1). Cases of optic disc pit not associated with maculopathy should not be treated prophylactically with laser along the temporal optic disc margin. The natural history of this disease may not involve maculopathy development, and the risk of injury to the papillomacular bundle does not justify this approach^(2)^.
The present study is limited by the small sample size, its retrospective nature, and lack of a control group. The postoperative treatment was not uniform, and two-thirds of the patients received anhydrase carbonic medications by different routes and during different periods. Low ODP-associated maculopathy incidence and multiple therapeutic options existence represent challenges in conducting comparative studies.
The procedure described herein represents a low-cost alternative therapeutic approach to manage ODP-associated macular detachment and is associated with outcomes similar to those obtained with the surgical procedures mentioned earlier^(20)^. It may be of particular interest in countries with limited public health resources and a lack of universal access to vitreoretinal surgeries.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Wiethe T A case of optic nerve deformity Archiv für Augenheilkunde 1882111419
- 2Jain N Johnson MW Pathogenesis and treatment of maculopathy associated with cavitary optic disc anomalies Am J Ophthalmol 201415834234352493298810.1016/j.ajo.2014.06.001 · doi ↗ · pubmed ↗
- 3Georgalas I Ladas I Georgopoulos G Petrou P Optic disc pit: a review Graefes Arch Clin Exp Ophthalmol 20112498111311222163803010.1007/s 00417-011-1698-5 · doi ↗ · pubmed ↗
- 4Halbertsma KT Crater-like hole and coloboma of the disc associated with changes at the macula Br J Ophthalmol 192711111171816858910.1136/bjo.11.1.11PMC 511893 · doi ↗ · pubmed ↗
- 5Steel DHW Suleman J Murphy DC Song A Dodds S Rees J Optic disc pit maculopathy: A Two-Year Nationwide Prospective Population-based Study Ophthalmology 201812511175717642988733110.1016/j.ophtha.2018.05.009 · doi ↗ · pubmed ↗
- 6Türkçüoğlu P Taskapan C The origin of subretinal fluid in optic disc pit maculopathy Ophthalmic Surg Lasers Imaging Retina 20164732942982698580610.3928/23258160-20160229-15 · doi ↗ · pubmed ↗
- 7Lincoff H Lopez R Kreissig I Yannuzzi L Cox M Burton T Retinoschisis associated with optic nerve pits Arch Ophthalmol 198810616167333770810.1001/archopht.1988.01060130067030 · doi ↗ · pubmed ↗
- 8Tzu JH Flynn HW Jr Berrocal AM Smiddy WE Murray TG Fisher YL Clinical manifestations of optic pit maculopathy as demonstrated by spectral domain optical coherence tomography Clin Ophthalmol [Internet]2013 citd 2020 Jul 277167172 Available from: Clinical manifestations of optic pit maculopathy as demonstrated by spectral domain optical coherence tomography (nih.gov)2335577210.2147/OPTH.S 37157 PMC 3552479 · doi ↗ · pubmed ↗