Dynamics of Serum Cytokines and Chemokines in Patients With Idiopathic Multicentric Castleman Disease: From a Phase Ib Investigator-Initiated Trial of Filgotinib
Shoichi Fukui, Remi Sumiyoshi, Tomohiro Koga, Naoki Hosogaya, Sawana Narita, Shimpei Morimoto, Hiroshi Yano, Atsushi Katsube, Shingo Yano, Yasufumi Masaki, Shinichiro Tsunoda, Shuzo Sato, Kiyoshi Migita, Atsushi Kawakami

TL;DR
This study compared how two drugs affect immune signals in a rare inflammatory disease, finding that one drug had limited impact on key markers.
Contribution
Identified specific cytokines/chemokines that may explain the limited efficacy of filgotinib in iMCD treatment.
Findings
Tocilizumab improved C-reactive protein, hemoglobin, and albumin levels, while filgotinib did not.
Tocilizumab significantly altered 12 cytokines/chemokines, while filgotinib only reduced IL-18 and IL-27.
Five cytokines (FGF-2, IL-4, IL-6, TNF-β, and VEGF-A) showed significant changes with tocilizumab and differences between groups.
Abstract
Background Idiopathic multicentric Castleman disease (iMCD) is a chronic inflammatory condition for which Janus kinase (JAK) inhibition has been hypothesized to be a potential treatment. However, filgotinib, a JAK1 preferential inhibitor, did not show apparent efficacy for iMCD in a clinical trial at eight weeks. This study aimed to compare the serum cytokine and chemokine profiles of patients treated with filgotinib with those of patients treated with tocilizumab to speculate why filgotinib was not effective at eight weeks. Methods This study included five patients treated with filgotinib who participated in a phase Ib single-arm clinical trial of filgotinib for iMCD and five tocilizumab-treated patients whose data were collected retrospectively. Serum levels of 41 cytokines/chemokines before and after treatment were measured. Results The tocilizumab group showed improvement in…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
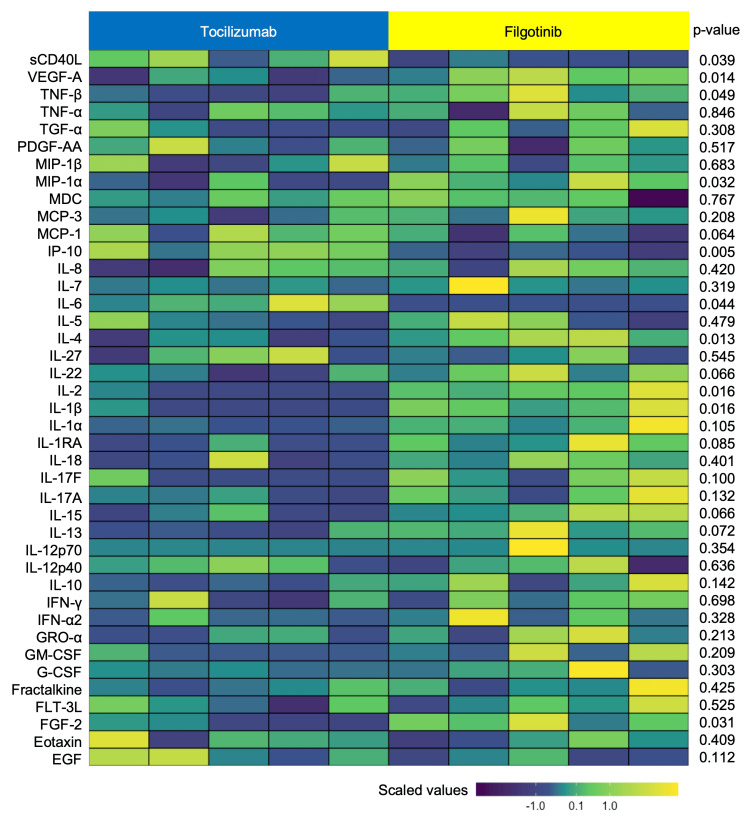 Figure 1
Figure 1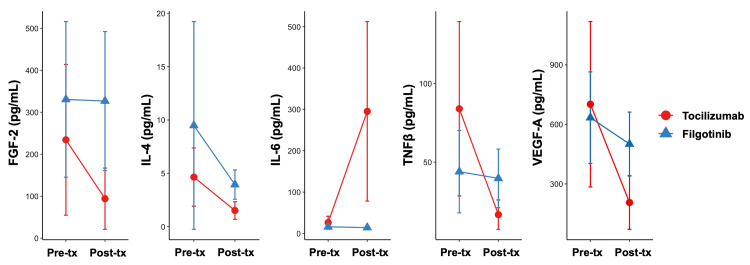 Figure 2
Figure 2| Characteristics | Tocilizumab (n=5) | Filgotinib (n=5) |
| At baseline | ||
| Age, years, median (min−max) | 62 (43-69) | 60 (37–61) |
| Sex, female, n (%) | 2 (40) | 2 (40) |
| Height, cm, median (min−max) | 160 (152-172) | 170 (152–176) |
| Body weight, kg, median (min−max) | 55.7 (46.1-72.5) | 73.7 (50.9–75.0) |
| Treatment-naïve, n (%) | 5 (100) | 3 (60) |
| Previous treatment with immunosuppressant, n (%) | ||
| Prednisolone | 0 (0) | 2 (40) |
| Others | 0 (0) | 0 (0) |
| Concomitant use of immunosuppressant, n (%) | ||
| Prednisolone 10 mg/day | 0 (0) | 1 (20) |
| Others | 0 (0) | 0 (0) |
| Histology, n (%) | ||
| Hyaline vascular type | 0 (0) | 0 (0) |
| Plasma cell type | 5 (100) | 5 (100) |
| Mixed type | 0 (0) | 0 (0) |
| CRP, mg/dL, median (min−max) | 4.90 (3.70-7.22) | 6.73 (2.47–7.45) |
| Hemoglobin, g/dL, median (min−max) | 9.3 (8.5-11.6) | 10.1 (8.1–11.8) |
| Albumin, g/dL, median (min−max) | 2.4 (2.4-2.7) | 2.9 (2.5–3.3) |
| ECOG-PS, n (%) | ||
| 0 | 4 (80) | 2 (40) |
| 1 | 1 (20) | 3 (60) |
| CHAP score, median (min−max) | 5 (3-7) | 5 (3–6) |
| Platelet count, ×103/μL, median (min−max) | 338 (262-456) | 339 (226-556) |
| Immunoglobulin G, mg/dL, median (min−max) | 4,436 (3,733-4,996) | 5,357 (4,446-5,968) |
| At 8 weeks* or later** | ||
| CRP, mg/dL, median (min−max) | 0.01 (0.01-0.04) | 6.13 (1.88-6.82) |
| Hemoglobin, g/dL, median (min−max) | 14.1 (12.6-14.3) | 10.0 (8.0-12.4) |
| Albumin, g/dL, median (min−max) | 4.2 (4.0-4.3) | 3.1 (2.7-3.4) |
| ECOG-PS, n (%) | ||
| 0 | 5 (100) | 4 (80) |
| 1 | 0 (0) | 1 (20) |
| CHAP score, median (min−max) | 0 (0-0) | 3 (2-5) |
| Tocilizumab at baseline (n=5) | Filgotinib at baseline (n=5) | Tocilizumab after treatment (n=5) | Filgotinib at 8 weeks (n=5) | 95% CI of healthy donors (n=101) | 1)t-statistic | 1)p-value | 2)t-statistic | 2)p-value | 3)t-statistic | 3)p-value | |
| EGF | 177 (139) | 51 (26) | 160 (105) | 64 (46) | 353-451 | 0.75 | 0.494 | -1.18 | 0.304 | 1.89 | 0.112 |
| Eotaxin | 113 (57) | 95 (43) | 172 (88) | 131 (51) | 114-138 | -2.56 | 0.063 | -1.20 | 0.295 | 0.88 | 0.409 |
| FGF-2 | 234 (180) | 331 (186) | 94 (73) | 327 (166) | 32-66 | 2.86 | 0.046 | 0.11 | 0.915 | -2.87 | 0.031 |
| FLT-3L | 14 (7) | 13 (11) | 10 (5) | 12 (6) | 36-54 | 2.92 | 0.043 | 0.30 | 0.782 | -0.67 | 0.525 |
| Fractalkine | 546 (654) | 278 (334) | 143 (65) | 236 (227) | 109-145 | 1.52 | 0.204 | 0.85 | 0.445 | -0.87 | 0.425 |
| G-CSF | 38 (19) | 58 (33) | 38 (6) | 80 (79) | 2-22 | -0.03 | 0.978 | -0.94 | 0.401 | -1.18 | 0.303 |
| GM-CSF | 68 (91) | 35 (64) | 7 (15) | 44 (55) | 3-7 | 1.51 | 0.206 | -0.40 | 0.707 | -1.46 | 0.209 |
| GRO | 75 (42) | 46 (25) | 29 (10) | 49 (30) | 16-24 | 2.75 | 0.052 | -0.70 | 0.521 | -1.43 | 0.213 |
| IFNα2 | 233 (287) | 164 (256) | 39 (71) | 145 (207) | 15-49 | 1.84 | 0.139 | 0.65 | 0.549 | -1.09 | 0.328 |
| IFNγ | 204 (81) | 134 (30) | 121 (42) | 130 (24) | 2-8 | 2.71 | 0.053 | 0.43 | 0.689 | -0.41 | 0.698 |
| IL-10 | 9 (5) | 22 (27) | 5 (2) | 11 (8) | 0-8 | 1.56 | 0.194 | 1.13 | 0.323 | -1.77 | 0.142 |
| IL-12p40 | 117 (53) | 71 (35) | 64 (15) | 56 (32) | 24-36 | 1.81 | 0.145 | 2.20 | 0.093 | 0.50 | 0.636 |
| IL-12p70 | 27 (49) | 85 (177) | 2 (1) | 79 (165) | 0-0 | 1.14 | 0.317 | 1.05 | 0.354 | -1.05 | 0.354 |
| IL-13 | 200 (231) | 136 (97) | 47 (31) | 124 (71) | 45-79 | 1.69 | 0.167 | 0.93 | 0.404 | -2.22 | 0.072 |
| IL-15 | 17 (10) | 29 (16) | 14 (8) | 30 (14) | 9-17 | 1.80 | 0.147 | -0.18 | 0.863 | -2.21 | 0.066 |
| IL-17A | 30 (30) | 26 (20) | 8 (7) | 27 (22) | 3-13 | 1.88 | 0.133 | -0.55 | 0.613 | -1.82 | 0.132 |
| IL-17F | 11 (14) | 28 (23) | 6 (12) | 25 (19) | 2-16 | 3.31 | 0.030 | 0.47 | 0.661 | -1.90 | 0.100 |
| IL-18 | 21 (34) | 29 (9) | 11 (13) | 17 (6) | 15-21 | 1.02 | 0.367 | 3.49 | 0.025 | -0.91 | 0.401 |
| IL-1ra | 8 (3) | 8 (2) | 4 (1) | 8 (4) | 1-7 | 2.35 | 0.078 | 0.15 | 0.887 | -2.14 | 0.085 |
| IL-1α | 21 (19) | 34 (26) | 3 (2) | 34 (33) | 13-37 | 2.33 | 0.080 | 0.01 | 0.991 | -2.08 | 0.105 |
| IL-1β | 19 (13) | 29 (12) | 9 (4) | 28 (12) | 12-36 | 2.57 | 0.062 | 0.05 | 0.965 | -3.54 | 0.016 |
| IL-2 | 2 (2) | 3 (2) | 0 (1) | 4 (2) | 0-2 | 1.78 | 0.150 | -0.52 | 0.628 | -3.69 | 0.016 |
| IL-22 | 380 (224) | 296 (198) | 123 (95) | 289 (142) | 1-13 | 3.08 | 0.037 | 0.22 | 0.839 | -2.18 | 0.066 |
| IL-27 | 1930 (1470) | 1204 (299) | 1193 (662) | 978 (348) | 1496-1882 | 1.98 | 0.119 | 2.79 | 0.049 | 0.64 | 0.545 |
| IL-4 | 5 (3) | 9 (10) | 2 (1) | 4 (1) | 0-2 | 3.49 | 0.025 | 1.39 | 0.237 | -3.39 | 0.013 |
| IL-5 | 3 (1) | 3 (3) | 3 (2) | 3 (2) | 6-10 | 0.11 | 0.918 | -0.44 | 0.686 | -0.75 | 0.479 |
| IL-6 | 26 (15) | 16 (6) | 295 (217) | 14 (4) | 2-2 | -2.84 | 0.047 | 1.43 | 0.226 | 2.90 | 0.044 |
| IL-7 | 12 (3) | 47 (78) | 8 (5) | 33 (49) | 6-24 | 2.27 | 0.086 | 1.09 | 0.336 | -1.13 | 0.319 |
| IL-8 | 169 (262) | 13 (2) | 11 (5) | 14 (4) | 86-184 | 1.33 | 0.256 | -0.48 | 0.657 | -0.85 | 0.420 |
| IP-10 | 189 (100) | 105 (62) | 248 (82) | 68 (38) | 124-158 | -1.72 | 0.161 | 2.03 | 0.112 | 4.42 | 0.005 |
| MCP-1 | 268 (95) | 295 (127) | 510 (172) | 280 (167) | 567-661 | -3.35 | 0.029 | 0.53 | 0.627 | 2.15 | 0.064 |
| MCP-3 | 115 (50) | 58 (18) | 37 (11) | 54 (24) | 14-22 | 4.24 | 0.013 | 1.46 | 0.218 | -1.42 | 0.208 |
| MDC | 375 (58) | 384 (120) | 381 (39) | 362 (128) | 691-815 | -0.19 | 0.860 | 2.17 | 0.096 | 0.31 | 0.767 |
| MIP-1α | 38 (16) | 36 (9) | 24 (7) | 38 (9) | 31-41 | 1.80 | 0.147 | -0.47 | 0.661 | -2.63 | 0.032 |
| MIP-1β | 51 (20) | 38 (11) | 40 (18) | 36 (7) | 47-61 | 0.89 | 0.426 | 0.42 | 0.699 | 0.43 | 0.683 |
| PDGF-AA | 13479 (5020) | 7649 (3578) | 9433 (3821) | 7809 (3757) | 4754-5588 | 4.46 | 0.011 | -0.37 | 0.732 | 0.68 | 0.517 |
| TGFα | 11 (3) | 13 (11) | 6 (5) | 11 (8) | 5-9 | 3.20 | 0.033 | 0.96 | 0.390 | -1.11 | 0.308 |
| TNFα | 65 (36) | 53 (20) | 41 (11) | 43 (23) | 14-18 | 1.50 | 0.207 | 2.31 | 0.082 | -0.20 | 0.846 |
| TNFβ | 84 (56) | 44 (26) | 17 (9) | 40 (19) | 5-9 | 2.98 | 0.041 | 0.91 | 0.414 | -2.47 | 0.049 |
| VEGF-A | 701 (417) | 634 (231) | 206 (135) | 501 (161) | 279-371 | 3.61 | 0.023 | 2.04 | 0.111 | -3.13 | 0.014 |
| sCD40L | 6050 (1989) | 1607 (991) | 6473 (3474) | 1824 (741) | 2223-2959 | -0.25 | 0.815 | -0.41 | 0.701 | 2.93 | 0.039 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsViral-associated cancers and disorders · Lymphoma Diagnosis and Treatment · Chronic Lymphocytic Leukemia Research
Introduction
Idiopathic multicentric Castleman disease (iMCD) is a rare disease characterized by systemic lymphadenopathy with constitutional symptoms (fever, night sweats, weight loss, and fatigue) [1]. Research has shown that elevated interleukin-6 (IL-6) levels correlate with clinical symptoms, leading to the development of the IL-6 inhibitors, tocilizumab [2] and siltuximab [3] for iMCD. These treatments are effective for iMCD; however, some patients experience intractable disease. Although various chemotherapeutic agents have been tried for refractory cases [4], evidence supporting their use remains minimal.
Recent research has focused on Janus kinases (JAKs), which regulate downstream of cytokine receptors, including IL-6 [5]. JAKs contribute to the signal transducer and activator of transcription 3 activation in iMCD pathogenesis [6], suggesting that JAK-STAT signaling inhibition is a potential treatment approach. This rationale led to a phase Ib investigator-led clinical trial of filgotinib for iMCD that was conducted at five facilities across Japan in 2024. Filgotinib, which has been approved for use in rheumatoid arthritis (RA) [7] and ulcerative colitis [8], is a JAK1 preferential inhibitor that suppresses downstream signals of IL-6, and it was anticipated that filgotinib would also be effective in iMCD. However, the treatment response at eight weeks was not promising because C-reactive protein (CRP), hemoglobin, and albumin levels showed no changes [9]. Further research is needed to understand why filgotinib did not show apparent efficacy for the future development of treatments for iMCD.
In this study, we aimed to elucidate the changes in serum cytokines and chemokines in patients treated with filgotinib by comparing them with those in patients treated with tocilizumab, the standard treatment for iMCD. This study was an exploratory post-hoc analysis using preserved sera from a clinical trial, and sera collected separately from the clinical trial. We anticipated that understanding the dynamics of multiple cytokines and chemokines would provide speculation on the cause of the lack of apparent efficacy of filgotinib in iMCD.
Materials and methods
Study design and patients
This study used sera from iMCD patients who participated in a single-arm trial of filgotinib (200 mg daily) registered in the Japan Registry of Clinical Trials (https://jrct.niph.go.jp/) as jRCT2071230108 (approved by the Nagasaki University Hospital Institutional Review Board, approval no. 123-002). The study was conducted from December 2023 to June 2024. In addition, sera from patients treated with tocilizumab were collected to be compared to those from patients treated with filgotinib. Patients in the tocilizumab group were diagnosed with iMCD at Nagasaki University Hospital between September 2018 and October 2023. Sera at baseline and eight weeks (filgotinib) or later (tocilizumab, median 28 months (minimum 11 - maximum 73 months)) were used. Clinical information of patients treated with tocilizumab, referring to clinical records, was collected retrospectively.
Criteria
All patients were diagnosed with iMCD according to the diagnostic criteria issued by Japan's Ministry of Health, Labour and Welfare, i.e., “Designated intractable diseases that became effective on April 1, 2018 (notice no. 331).” Patients with a total score on the CHAP (C-reactive protein (CRP), Hemoglobin, Albumin, + Performance Status (PS, Eastern Cooperative Oncology Group (ECOG))) [10] that was ≥2 points in total with hemoglobin or albumin ≥1 point and CRP ≥1 point at baseline. Patients with iMCD-TAFRO (thrombocytopenia, anasarca, fever, reticulin fibrosis, renal insufficiency, and organomegaly clinical subtype) as defined by the validated international definition [11] were excluded.
Outcomes
Endpoints were as follows at eight weeks of treatment (filgotinib) or later (tocilizumab): (1) the patient's CHAP score [10], (2) CRP (mg/dL), (3) hemoglobin (g/dL), (4) albumin (g/dL), and (5) the ECOG-PS.
Multiple cytokines/chemokines measurements
The sera of the patients were analyzed using the Milliplex^®^ MAP Human Cytokine/Chemokine Magnetic Bead Panel-Premixed 41 Plex panel (Merck Millipore, Billerica, MA, USA) and MAGPIX® with xPONENT^®^ software (Luminex Corp., Austin, TX, USA). The levels of 41 cytokines/chemokines were measured as follows: epidermal growth factor (EGF), CCL11/eotaxin, basic fibroblast growth factor (FGF-2/bFGF), FMS-like tyrosine kinase 3 ligand (FLT-3 L), fractalkine, granulocyte colony-stimulating factor (G-CSF), granulocyte-macrophage colony-stimulating factor (GM-CSF), chemokine (C-X-C motif) ligand 1 (CXCL1/GRO-α), interferon (IFN)-α2, IFN-γ, interleukin (IL)-10, IL-12p40, IL-12p70, IL-13, IL-15, IL-17A, IL-17F, IL-18, IL-1 receptor antagonist (IL-1RA), IL-1α, IL-1β, IL-2, IL-22, IL-27, IL-4, IL-5, IL-6, IL-7, IL-8, C-X-C motif chemokine ligand 10 (CXCL10/IP-10), monocyte chemoattractant protein-1 (MCP-1/CCL2), MCP-3, macrophage-derived chemokine (MDC), CCL3/macrophage inflammatory protein (MIP)-1α, CCL4/MIP-1β, platelet-derived growth factor (PDGF)-AA, transforming growth factor (TGF)-α, tumor necrosis factor (TNF)-α, TNF-β, vascular endothelial growth factor (VEGF)-A, and soluble CD40 ligand (sCD40L).
Healthy donors
Sera from healthy donors - residents of the town of Saza in Nagasaki prefecture - who underwent specific health checkups in 2016 were used for the 41 Plex panel as the controls to calculate the normal limits with 95% confidence interval (approved by the Ethics Committee of the Nagasaki University Graduate School of Biomedical Sciences, project registration number: 14051404). All healthy donors had no past or present medical history of inflammatory disease (n=101 (59 women), mean age 58 (standard deviation: 10) years).
Ethics
This study complied with the Declaration of Helsinki and was approved by the Nagasaki University Hospital Institutional Review Board (approval no. 24120503). An opt-out approach was used to obtain patient consent for the study.
Statistical analyses
Categorical and continuous variables are described as frequencies and means with standard deviations unless otherwise specified. Associations between variables were assessed using the student's t-test for continuous variables. The paired t-test was used to assess differences in serum cytokine and chemokine levels at baseline and after treatment. All hypothesis tests were conducted at a significance level of 0.05. The selective process of null hypotheses or multiplicity of the tests was not considered because of the exploratory objective of the analyses [12]. All statistical analyses were performed using R ver. 4.3.2 (R Foundation for Statistical Computing, Vienna, Austria).
Results
Patient characteristics at baseline
Table 1 presents the baseline characteristics. The median patient age was 62 and 60 years in the tocilizumab and filgotinib groups, respectively. The lymph node histology at diagnosis was plasma cell type, and neither the hyaline-vascular type nor the mixed type was observed in either group. All patients were diagnosed with idiopathic plasmacytic lymphadenopathy (IPL) based on the criteria for IPL [13], which was modified from the original criteria by Mori et al. [14]. The median CRP levels were 4.90 mg/dL and 6.73 mg/dL, respectively. The median CHAP (CRP, Hemoglobin, Albumin, + PS (ECOG)) score at baseline was five in both groups.
Outcomes at eight weeks or later
All five patients in the filgotinib group completed eight weeks of treatment with no discontinuation. The median CRP levels after treatment were 0.01 mg/dL (tocilizumab) and 6.13 mg/dL (filgotinib), respectively. The median hemoglobin level and albumin level after treatment were 14.1 g/dL and 10.0 g/dL, and 4.2 g/dL and 3.1 g/dL, respectively. The median CHAP scores were 0 and 3, respectively.
Comparison of cytokines and chemokines between the two groups
Table 2 shows the serum levels of cytokines and chemokines in both groups.
The tocilizumab group showed a significant decrease in the serum levels of FGF-2, FLT-3L, IL-17F, IL-22, IL-4, MCP-3, PDGF-AA, TGF-α, TNF-β, and VEGF-A, and a significant increase in the serum levels of IL-6 and MCP-1 from baseline to after treatment. The filgotinib group showed a significant decrease in serum levels of IL-18 and IL-27 from baseline to after treatment. Figure 1 shows the differences in serum cytokines and chemokines after treatment between the two groups on a heat map. Significant differences were observed in the serum levels of FGF-2, IL-1β, IL-2, IL-4, IL-6, IP-10, MIP-1α, TNF-β, VEGF-A, and sCD40L between the tocilizumab and filgotinib groups after treatment.
Heat map of serum cytokines and chemokines after treatment of the tocilizumab group and the filgotinib groupThe p-values were calculated using the student’s t-test to compare cytokines and chemokines between the two groups. Colors represent scaled values of cytokines and chemokines.
Serum cytokines and chemokines that were significantly different between at baseline and after treatment in the tocilizumab group and significantly different between tocilizumab and filgotinib after treatment included FGF-2, IL-4, IL-6, TNF-β, and VEGF-A (Figure 2). All cytokines were lower in the tocilizumab group than in the filgotinib group after treatment, except for IL-6.
Cytokines with significant differences between the two groupsPre-tx: pre-treatment, Post-tx: post-treatment
Discussion
This exploratory study showed significant differences in the serum levels of FGF-2, IL-4, IL-6, TNF-β, and VEGF-A between the tocilizumab and filgotinib groups after treatment among cytokines and chemokines that significantly changed after tocilizumab administration. Here, we summarize and discuss previous reports on the relationship between these cytokines and iMCD or Castleman disease.
TNF-β, also known as lymphotoxin-α, plays a role in regulating the growth and function of lymphocytes. Elevated levels of TNF-β mRNA have been observed in lymph nodes in Castleman disease [15]. In addition, serum proteomic analyses have identified TNF signaling as a highly enriched pathway in iMCD patients [16], which is not limited to TNF-β. Elevated serum TNF-β levels in iMCD above the upper limit of the normal range from healthy donors may contribute to the inflammatory state and lymph node abnormalities of iMCD.
VEGF stimulates angiogenesis. Elevated VEGF levels were observed in the sera and lymph node supernatants of patients with Castleman disease compared with those of normal controls [17,18]. In addition, immunohistochemical analyses have revealed VEGF expression in plasma cells within the interfollicular regions of affected lymph nodes [17,18]. VEGF expression was also detected in the germinal center of Castleman disease cases, unlike in the normal tonsillar germinal center [19]. Based on these reports, VEGF is thought to contribute to the pathophysiology of iMCD.
Elevation of IL-6 levels after the initiation of tocilizumab in Castleman disease has been reported [20]. Therefore, our results of elevated serum IL-6 levels after tocilizumab treatment are consistent with a previous report. Regarding no changes in IL-6 in the filgotinib group, we concluded that filgotinib could not inhibit IL-6 at eight weeks in this study because a case report of iMCD-not otherwise specified (NOS) mentioned the time-dependent decrease of serum IL-6 by ruxolitinib with dexamethasone [21]. However, it should be noted that the transcriptomic levels of cytokines differ between iMCD-NOS/TAFRO and iMCD-IPL in lymph nodes [22], which may affect serum cytokines because our study included only patients with iMCD-IPL.
In RA, filgotinib decreased the serum levels of multiple cytokines, Th1-related cytokines (IL-2, IFN-γ, and IL-12), Th2-related cytokines (IL-4, IL-5, and IL-13), and Th17-related cytokines (IL-1β, IL-6, IL-17A, IL-21, and IL-23) at 12 weeks [23]. Another study in RA reported that filgotinib decreased CRP levels by 77.4% and IL-6 levels by 13.6% relative to placebo at 12 weeks [24]. Based on these reports, filgotinib in iMCD did not seem to suppress any cytokines at eight weeks, although attention is required for the short duration of treatment with filgotinib.
To the best of our knowledge, FGF-2 and IL-4 have not been reported to be associated with iMCD pathogenesis. The contributions of fibroblasts and Th2 cells to the pathogenesis of iMCD will be considered in the future.
This study has several limitations. First, this study compared only five patients in the tocilizumab group and five patients in the filgotinib group because the filgotinib trial recruited only five patients. The small sample size limits statistical power. Second, the evaluation at eight weeks in the filgotinib group may have been too short to evaluate the effects of filgotinib on serum cytokines and chemokines. The small sample size and short duration of treatment in the filgotinib group limit the generalizability of our findings. Third, the timing of serum collection after treatment initiation varied in the tocilizumab group because the tocilizumab group was retrospectively collected. Additionally, the retrospective nature of the tocilizumab group introduced a potential selection bias. Fourth, because none of the patients in the filgotinib group showed apparent efficacy, it was impossible to distinguish whether the differences in cytokines and chemokines between the tocilizumab and filgotinib groups were due to the difference in the effects and durations of treatment or the difference in disease activity after treatment. Fifth, the statistical significance found in this study was based on the p-values that presumed the values were not greater than the nominal type-1 error rate, that is, the usual definition of the p-value [12]. Therefore, the results lack statistical validity.
This study has its strengths. We have provided data on the time course of multiple cytokines and chemokines in iMCD, a rare disease. We focused on FGF-2, IL-4, IL-6, TNF-β, and VEGF-A based on the statistical analysis in this report; however, other intriguing findings in the data may be helpful for other clinicians and researchers. Despite the above-mentioned limitations, our speculative findings may suggest why filgotinib did not show apparent clinical efficacy.
Conclusions
In this exploratory analysis comparing the treatment of iMCD with tocilizumab and filgotinib, we identified significant differences in several key cytokines, which may explain the lack of apparent efficacy of filgotinib. Most notably, FGF-2, IL-4, IL-6, TNF-β, and VEGF-A levels showed distinct patterns. The persistent elevation of TNF-β and VEGF-A levels in patients treated with filgotinib suggests that JAK1-preferential inhibition may be insufficient to control the complex inflammatory cascade in iMCD. While our findings are limited by the small sample size and short duration of filgotinib treatment, these results not only help explain the outcomes of current standard treatment but also provide potential implications for the future development of effective treatments for patients with iMCD.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Idiopathic multicentric Castleman disease: an update in diagnosis and treatment advances Blood Rev Lang E van Rhee F 1011616420243808771610.1016/j.blre.2023.101161 · doi ↗ · pubmed ↗
- 2Humanized anti-interleukin-6 receptor antibody treatment of multicentric Castleman disease Blood Nishimoto N Kanakura Y Aozasa K 2627263210620051599883710.1182/blood-2004-12-4602 · doi ↗ · pubmed ↗
- 3Siltuximab, a novel anti-interleukin-6 monoclonal antibody, for Castleman's disease J Clin Oncol van Rhee F Fayad L Voorhees P 370137082820102062512110.1200/JCO.2009.27.2377 · doi ↗ · pubmed ↗
- 4International, evidence-based consensus treatment guidelines for idiopathic multicentric Castleman disease Blood van Rhee F Voorhees P Dispenzieri A 2115212413220183018117210.1182/blood-2018-07-862334 PMC 6238190 · doi ↗ · pubmed ↗
- 5The JAK-STAT pathway: impact on human disease and therapeutic intervention Annu Rev Med O'Shea JJ Schwartz DM Villarino AV Gadina M Mc Innes IB Laurence A 3113286620152558765410.1146/annurev-med-051113-024537 PMC 5634336 · doi ↗ · pubmed ↗
- 6Discovery and validation of a novel subgroup and therapeutic target in idiopathic multicentric Castleman disease Blood Adv Pierson SK Shenoy S Oromendia AB 34453456520213443844810.1182/bloodadvances.2020004016 PMC 8525223 · doi ↗ · pubmed ↗
- 7Effect of filgotinib vs placebo on clinical response in patients with moderate to severe rheumatoid arthritis refractory to disease-modifying antirheumatic drug therapy. The FINCH 2 randomized clinical trial JAMA Genovese MC Kalunian K Gottenberg JE 31532532220193133479310.1001/jama.2019.9055 PMC 6652745 · doi ↗ · pubmed ↗
- 8Filgotinib as induction and maintenance therapy for ulcerative colitis (SELECTION): a phase 2b/3 double-blind, randomised, placebo-controlled trial Lancet Feagan BG Danese S Loftus EVJ 2372238439720213409062510.1016/S 0140-6736(21)00666-8 · doi ↗ · pubmed ↗