Successful Treatment With Evocalcet Against Familial Hypocalciuric Hypercalcemia Type 3 (FHH3) Identified by AP2S1 Gene Mutation (p.Arg15Leu)
Ai Chida, Yutaka Hasegawa, Toshie Segawa, Daisuke Yamabe, Hirotaka Yan, Yusuke Chiba, Hiraku Chiba, Hirofumi Kinno, Tomoyasu Oda, Yoshihiko Takahashi, Koji Nata, Yasushi Ishigaki

TL;DR
A 21-year-old woman with a rare genetic disorder causing high blood calcium levels was successfully treated with a new drug called evocalcet.
Contribution
This case demonstrates that evocalcet, a calcium-sensing receptor agonist, can effectively treat FHH3 caused by an AP2S1 gene mutation.
Findings
Evocalcet normalized serum calcium levels in a patient with FHH3.
The treatment improved bone metabolism without serious side effects.
The patient had a confirmed AP2S1 gene mutation (p.Arg15Leu).
Abstract
Background: Familial hypocalciuric hypercalcemia type 3 (FHH3) is a rare hereditary disorder caused by a heterozygous AP2S1 gene mutation, characterized by hypocalciuria and hypercalcemia due to impaired intracellular signal transduction of calcium (Ca)-sensing receptors (CaSRs). All affected patients harbored a heterozygous missense mutation at the Arg15 residue of the encoded AP2σ1. Case Presentation: A 21-year-old female was referred to our hospital with hypercalcemia and reduced bone mineral density (BMD) detected during a preoperative examination for scoliosis surgery. She had a developmental disorder and exhibited hypocalciuria on urinalysis. Genetic testing revealed a heterozygous AP2S1 gene mutation (p.Arg15Leu), and the patient was diagnosed with FHH3. In the present case, we investigated the effects of evocalcet, a newly approved CaSR agonist. Treatment with evocalcet…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
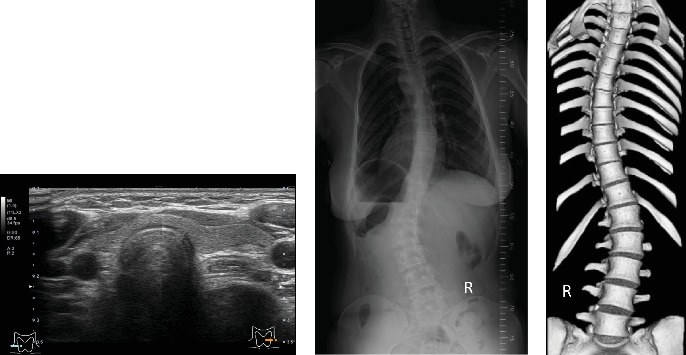 Figure 1
Figure 1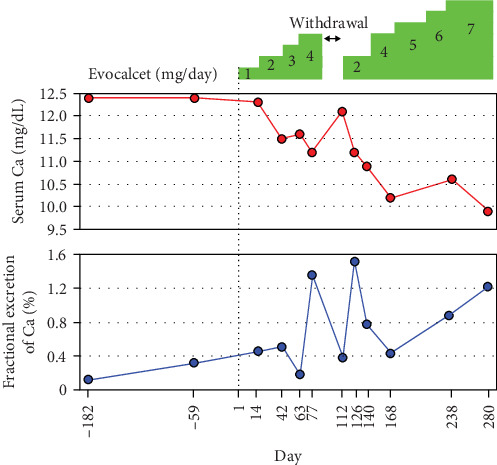 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsParathyroid Disorders and Treatments · Bone health and treatments · Magnesium in Health and Disease
1. Introduction
Familial hypocalciuric hypercalcemia (FHH) is a rare autosomal dominant genetic disease caused by abnormalities in calcium (Ca)-sensing receptors (CaSRs) and their signal transduction [1]. They are classified into three different types depending on the location of the responsible genes. Type 1 is caused by loss-of-function mutations of CASR encoding CaSR; type 2 is by mutations of GNA11 encoding G-protein subunit α11 (Gα11), and type 3 is by mutations of AP2S1 encoding adapter-related protein complex 2 subunit sigma 1 (AP2σ1). These phenotypes are characterized by a persistent increase in the serum Ca level, inappropriately low urinary Ca excretion, and a nonsuppressed serum parathyroid hormone (PTH) level [2, 3]. Regarding FHH type 3 (FHH3), AP2S1 gene mutations have been reported to date; all patients have heterozygous missense substitutions of AP2σ2 at the Arg15 residue (Arg15Cys, Arg15His, and Arg15Leu) [4], which causes a decrease in CaSR-mediated intracellular signaling [4]. Among FHH3 cases, stronger phenotypes, such as marked hypercalcemia, reduced bone density, comorbid cognitive, and behavioral disorders, have been reported with Arg15Leu mutations [1, 5–7].
As for the treatment, the majority of FHH cases do not require any treatment. As there are several reports of symptoms and morbidities related to hypercalcemia, effective treatments have been proposed for symptomatic cases [3]. Calcimimetic drugs, such as cinacalcet, have been reported to be effective against the symptoms and morbidity related to FHH [1, 8–10], including FHH3 [11–13]. Recently, a newly approved oral calcimimetic drug, evocalcet, has shown equivalent efficacy to cinacalcet and a lower incidence of gastrointestinal-related adverse events [14–16]. Therefore, evocalcet treatment for FHH3 could be considered an appropriate alternative treatment.
Herein, we describe a rare case of FHH3 patient with a heterozygous AP2S1 gene mutation (p.Arg15Leu). Treatment with evocalcet normalized the serum Ca level and contributed to the improvement of bone metabolism markers without obvious adverse events. To the best of our knowledge, this is the first report on the efficacy of evocalcet in FHH3.
2. Case Presentation
A 21-year-old female was referred to our clinic as hypercalcemia was detected on preoperative examination for scoliosis surgery. In the medical history, she was diagnosed with a pervasive developmental disorder and had hypercalcemia (serum Ca 12.6 mg/dL) at the age of five. However, the serum Ca level had never been measured while a patient at a psychiatric clinic. After being diagnosed with a pervasive developmental disorder during childhood, she attended a vocational school. Currently, she works in the hotel service business. She had been prescribed lithium carbonate for bipolar disorder since the age of 13 years and diagnosed with scoliosis at the age of 15 years. There was no family history of hypercalcemia, developmental disorders, or scoliosis.
Her height and weight were 167.0 cm and 58.1 kg, respectively, and blood pressure was 116/64 mmHg. Thyroid ultrasonography revealed no enlarged parathyroid glands (Figure 1A). Abdominal computed tomography (CT) imaging revealed no calcified lesions in the urinary tract. Scoliosis was observed on radiography and three-dimensional CT (Figure 1B,C). The Cobb angles on the proximal thoracic, main thoracic, and thoracolumbar/lumbar radiographs were 4.4°, 35.6°, and 41.2°, respectively. Lumbar spine bone mineral density (BMD) was 0.687 g/cm^2^, 67% of the young adult mean (YAM), and Z-score, −3.1, which were low values despite the young age. The serum Ca level was high (12.5 mg/dL), although the intact PTH level was not suppressed (50.7 pg/mL) (Table 1). The serum magnesium level was slightly elevated (2.4 mg/dL). Measurement of total 24-h urine Ca revealed lower urinary Ca excretion (60 mg/day) and fractional excretion of Ca (FECa = 0.33%). As the patient had hypercalcemia since childhood and exhibited hypocalciuria with an unsuppressed parathyroid PTH level, FHH was suspected. After obtaining informed consent from the patient for genetic analysis, next-generation sequencing was performed. A heterozygous missense mutation (c.44G >T, p.Arg15Leu) was detected in the AP2S1 gene, and the patient was diagnosed with FHH3. The asymptomatic parents did not consent to genetic analysis.
Owing to persistent hypercalcemia and concomitant low bone density, treatment of hypercalcemia was considered to be necessary. Previous reports have reported the efficacy of cinacalcet, which acts as an allosteric modulator on CaSRs, against FHH3 [8, 11, 12]. Notably, evocalcet, a newly approved calcimetric drug, has a mechanistic action similar to cinacalcet and is effective in improving bioavailability and reducing gastrointestinal tract-related adverse events [15, 17]. Therefore, this was considered to be an appropriate or superior treatment in this case. After obtaining approval from the hospital's Pharmaceutical Affairs Committee and obtaining patient consent, treatment with evocalcet was initiated.
After initiating treatment with evocalcet, the serum Ca level gradually decreased (Figure 2). The patient had indeterminate complaints about fingernails, so the treatment was discontinued for 14 days. The symptoms of the complaints improved during follow-up, and restarting the medication relowered the elevated serum Ca level. With a gradual increase in medication dose, oral administration of evocalcet (7 mg/day) normalized the serum Ca level (Figure 2). In parallel with the change in the serum Ca level, the FECa increased (Figure 2), whereas the level of intact PTH remained within normal limits. Although no apparent improvement in BMD was observed during this short-term treatment, the fasting level of total procollagen type I N-terminal propeptide (P1NP), a bone formation marker, increased from 83.5 to 98.5 ng/mL (Table 2). In contrast, the level of tartrate-resistant acid phosphatase 5b (TRACP-5b), a bone resorption marker, decreased from 337 to 303 mU/dL (Table 2). These data indicated that evocalcet is highly effective against FHH3 by normalizing the Ca level and promoting bone metabolism.
3. Discussion
FHH3 is a rare autosomal dominant genetic disease caused by a loss-of-function mutation in the AP2S1 gene. Due to a decrease in CaSR signal transduction, it typically exhibits hypercalcemia, hypocalciuria, hypermagnesemia, and hypophosphatemia. Despite the high level of serum Ca, the PTH level is normal or mildly elevated due to the decreased sensitivity of CaSR [3, 18]. Compared to FHH type 1, patients with FHH3 present with a higher plasma Ca concentration [5, 19]. Among the three variants of FHH3 (p.Arg15Cys, p.Arg15His, and p.Arg15Leu), this patient has a genetic variant of the AP2S1 gene at Arg15 residue (p.Arg15Leu). Previously, it has been reported that patients with the FHH3 variant (p.Arg15Leu) have marked hypercalcemia, which causes problems such as pancreatitis and decreased BMD and is associated with a high incidence of neurodevelopmental disorders. Regarding FHH3, it has been reported that ~60% of patients with the p.Arg15Leu mutation have a learning disability [5, 20]. This patient had cognitive impairment and attended vocational school during childhood. This case is a sporadic case of FHH3, and there is no family history of cognitive impairment. Although the detailed mechanism of cognitive impairment due to AP2S1 gene mutation is still unclear, exposure to marked hypercalcemia from infancy or childhood may lead to neurological developmental disability [21]. In addition, impaired CaSR signaling and transduction may impair neurological development [22]. Indeed, expression of mutant AP2σ2 subunits within the brain may directly influence neurological development and mediate receptor trafficking within neuronal synapses of the hippocampus [5, 23]. Furthermore, expression of the AP2 complex regulates synaptic vesicle recycling in neurons in a Ca-independent manner [24].
To date, the efficacy of treatment with calcimimetic drugs, that is, CaSR modulators, such as cinacalcet, has been reported in several symptomatic cases of FHH [11, 13, 25, 26]. A newly approved CaSR modulator, evocalcet, has been shown to be as effective as cinacalcet and has fewer gastrointestinal-related adverse effects [15, 16, 27]. Unlike cinacalcet, evocalcet does not affect the activity of cytochrome P450 enzymes, suggesting that it is a better alternative with higher bioavailability [28, 29]. The efficacy and safety of long-term administration of evocalcet have also been demonstrated [27, 30]. Therefore, we concluded that it was more appropriate to administer evocalcet rather than cinacalcet to this patient. As a result of evocalcet administration, the serum Ca level gradually declined and returned to a normal value. In this case, no obvious side effects, such as upper gastrointestinal disorders, were observed after treatment. Notably, 14 days after drug withdrawal, the elevated serum Ca level returned to a high level, confirming its reversibility. In fact, the correction of hypercalcemia alleviated the patient's anxiety and enabled her to obtain and continue work as a hotel staff member.
The patient also exhibited reduced bone density and scoliosis. As more than 50% of patients with FHH3 exhibit decreased bone density, CaSR signals play important roles in bone formation, and patients are likely to develop osteoporosis or osteomalacia [1, 19]. Before the initiation of evocalcet treatment, this young patient presented with a decreased BMD in the lumbar vertebrae of −3.1SD (67% YAM). One year of evocalcet treatment slightly decreased the BMD in the lumbar vertebrae to −3.5SD (62.0% YAM). In contrast, a bone formation marker (total P1NP) increased, whereas a bone resorption marker (TRACP-5b) decreased after evocalcet treatment. These data clearly demonstrate the efficacy of evocalcet on bone mineral metabolism in this patient. Although there have been no reports of patients with FHH3 with scoliosis, mice lacking the CaSR exhibit bone defects and delayed cartilage and growth plate development [31, 32]. These reports suggest that defects in Ca signal transduction due to the mutant AP2σ1 protein may cause scoliosis. We expect that the precise mechanism will be elucidated in future studies.
4. Conclusion
We experienced a case in which evocalcet, a CaSR agonist, was effective against FHH3, identified by an AP2S1 gene mutation (c.44G >T, p.Arg15Leu). Evocalcet is considered to be an effective treatment for FHH3; however, long-term surveillance is required to assess its safety and monitor the serum Ca level and bone mineral metabolism.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Hannan F. M. Babinsky V. N. Thakker R. V. Disorders of the Calcium-Sensing Receptor and Partner Proteins: Insights Into the Molecular Basis of Calcium Homeostasis Journal of Molecular Endocrinology 2016573 R 127R 14210.1530/JME-16-01242-s 2.0-8499399208727647839 PMC 5064759 · doi ↗ · pubmed ↗
- 2Christensen S. E. Nissen P. H. Vestergaard P. Mosekilde L. Familial Hypocalciuric Hypercalcaemia: A Review Current Opinion in Endocrinology, Diabetes & Obesity 201118635937010.1097/MED.0b 013e 32834 c 3c 7c 2-s 2.0-8025513812121986511 · doi ↗ · pubmed ↗
- 3Lee J. Y. Shoback D. M. Familial Hypocalciuric Hypercalcemia and Related Disorders Best Practice & Research Clinical Endocrinology & Metabolism 201832560961910.1016/j.beem.2018.05.0042-s 2.0-8504877983030449544 PMC 6767927 · doi ↗ · pubmed ↗
- 4Nesbit M. A. Hannan F. M. Howles S. A. Mutations in AP 2S 1 Cause Familial Hypocalciuric Hypercalcemia Type 3 Nature Genetics 2013451939710.1038/ng.24922-s 2.0-8487194903823222959 PMC 3605788 · doi ↗ · pubmed ↗
- 5Hannan F. M. Howles S. A. Rogers A. Adaptor Protein-2 Sigma Subunit Mutations Causing Familial Hypocalciuric Hypercalcaemia Type 3 (FHH 3) Demonstrate Genotype-Phenotype Correlations, Codon Bias and Dominant-Negative Effects Human Molecular Genetics 201524185079509210.1093/hmg/ddv 2262-s 2.0-8494066464126082470 PMC 4550820 · doi ↗ · pubmed ↗
- 6Aashiq M. Malallah A. J. Khan F. Alsada M. Clinical and Biochemical Features in a Case of Familial Hypocalciuric Hypercalcemia Type 3 With AP 2S 1 Gene Mutation in Codon Arg 15His Case Reports in Pediatrics 20202020310.1155/2020/73128947312894 PMC 700793032047691 · doi ↗ · pubmed ↗
- 7Szalat A. Shpitzen S. Tsur A. Stepwise Ca SR, AP 2S 1, and GNA 11 Sequencing in Patients With Suspected Familial Hypocalciuric Hypercalcemia Endocrine 201755374174710.1007/s 12020-017-1241-52-s 2.0-8501187469128176280 · doi ↗ · pubmed ↗
- 8Mayr B. Schnabel D. Dorr H. G. Schofl C. GENETICS IN ENDOCRINOLOGY: Gain and Loss of Function Mutations of the Calcium-Sensing Receptor and Associated Proteins: Current Treatment Concepts European Journal of Endocrinology 20161745 R 189R 20810.1530/EJE-15-10282-s 2.0-8497002875626646938 · doi ↗ · pubmed ↗