Isolated Gallbladder Melanoma: A Diagnostic Conundrum of Primary vs. Metastatic Disease
Ryan Patterson, Jessica Wernberg, Rohit Sharma

TL;DR
This paper presents a rare case of isolated gallbladder melanoma, highlighting the difficulty in determining if it is a primary tumor or a metastasis.
Contribution
The paper contributes a rare case report and discussion on managing isolated gallbladder melanoma.
Findings
An exhaustive workup failed to identify a primary site outside the gallbladder.
The patient was started on immunotherapy after a multidisciplinary review.
The case highlights the rarity and diagnostic challenges of isolated gallbladder melanoma.
Abstract
Melanoma is a malignant proliferation of melanocytes originating from neural crest cells. Gallbladder melanoma is typically reported as a metastatic disease involving the adjacent liver. Thus, isolated gallbladder melanoma must be either a primary tumor originating within the gallbladder without evidence of metastasis or an isolated metastatic lesion from an unknown or regressed primary site. Regardless of its classification as primary or metastatic, isolated gallbladder melanoma is an extremely rare diagnosis. We present a case of incidentally discovered isolated gallbladder melanoma in a resected specimen from a patient undergoing surgery for symptomatic cholelithiasis. An exhaustive workup failed to identify a primary site outside the gallbladder. The case was reviewed at a multidisciplinary tumor board, and the patient was started on immunotherapy. This case report aims to highlight…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
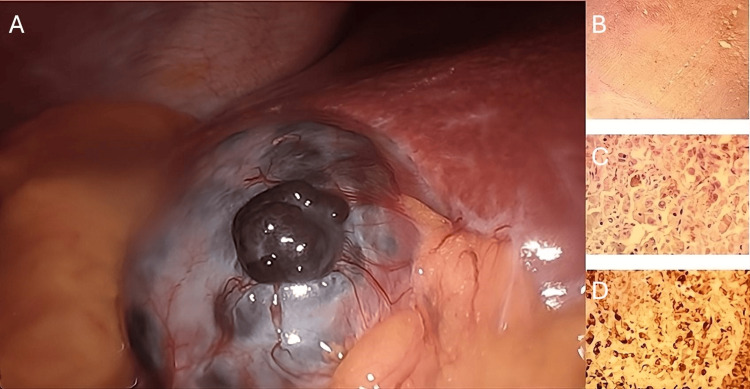 Figure 1
Figure 1| Clinical study | Primary or metastatic | Number of cases | Isolated gallbladder melanoma |
|
Heath and Womack (1988) [ | Primary | 19 | 5 cases |
|
Giannini et al. (2016) [ | Metastatic | 38 | 4 cases |
|
Jeon et al. (2021) [ | Metastatic | 4 | 0 cases |
|
Furumoto et al. (2013) [ | Metastatic | 1 | 0 cases |
|
Cassou-Mounat et al. (2019) [ | Metastatic | 1 | 0 cases |
| Characteristic | Primary | Metastatic | Our patient |
| Mucosal involvement | Involved | Not involved | Involved |
| Junctional activity* | Present | Absent | Absent |
| Focality | Single | Multiple | Multiple |
| Precursor lesion | Present | Absent | Absent |
| Alternate primary workup | Negative | Present | Negative |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCutaneous Melanoma Detection and Management · Multiple Myeloma Research and Treatments · Melanoma and MAPK Pathways
Introduction
Melanocytes are typically found in ectodermal derivatives such as the skin, eyes, and mucosa, but are not commonly present in endodermal derivatives like the gallbladder. While primary melanoma of the gallbladder is a debated clinical entity, it remains theoretically possible. However, gallbladder melanoma is most often identified as part of a metastatic disease pattern. Autopsy studies of patients with metastatic melanoma have reported biliary metastases in 4-20% of cases, typically in the context of widespread peritoneal disease [1]. Additionally, no identifiable primary lesion is found in 4-12% of metastatic melanoma cases [2].
Here, we present a case of incidental gallbladder melanoma, detailing the diagnostic workup, treatment options, and a brief review of the literature.
Case presentation
A 62-year-old Caucasian female presented with one day of right upper quadrant (RUQ) pain. Her medical history included morbid obesity, and her father had a history of non-melanoma skin cancer. She was a former smoker. Physical and laboratory examinations were unremarkable except for tenderness to palpation in the RUQ. A RUQ ultrasound revealed a large 5 cm stone and sludge. She was diagnosed with symptomatic cholelithiasis and, one month later, underwent elective laparoscopic cholecystectomy. Intraoperatively, an exophytic, darkly pigmented lesion approximately 2 cm in size (Figure 1) was identified on the gallbladder, with no lesions observed on the visualized hepatic surface. The gallbladder was aspirated, but otherwise not entered, and was removed in a specimen retrieval bag. No irrigation was performed during the operation.
Incidental lesions observed on the gallbladder surface during laparoscopy(A) Exophytic, darkly pigmented lesion identified during laparoscopic cholecystectomy. (B) Low-power view showing melanoma involvement of the gallbladder wall. (C) High-power view of melanoma cells with prominent nucleoli and dusky brown, coarsely pigmented cytoplasm. (D) Positive immunohistochemical staining for melanoma cocktail (courtesy of Dr. Ryan Bemke).
Histology revealed nests of melanoma extending transmurally from the mucosa, an equivocal cystic duct margin, and a positive cystic lymph node (LN; one of two). Stains were S100/melanin positive and CD68 negative. Molecular markers identified the lesion as NRAS and TERT mutated, while BRAF, KIT, GNA11/GNAQ, and BAP1 were wild type. Investigations for an alternate primary site, including PET-CT, esophagogastroduodenoscopy (EGD)/colonoscopy, and dermatological and ophthalmological exams, were negative. The case was presented at the multidisciplinary tumor board (MDTB), and treatment with pembrolizumab (Keytruda, Merck, Rahway, New Jersey, United States) was recommended. Restaging scans five months later showed FDG-avid aortocaval LNs and soft tissue adjacent to cystic duct clips. Ipilimumab (Yervoy, Bristol-Myers Squibb, New York, New York, United States) was added for four cycles. Tumor-infiltrating lymphocyte (TIL) therapy was not offered, as the patient presented prior to FDA approval for TIL therapy for patients with progression of melanoma while on first-line therapy. Post-ipilimumab PET scans showed improvement in aortocaval LNs and a left lower lung lobe avid density. Chest CT revealed interval enlargement of the pulmonary nodule, and biopsy showed chronic organizing pneumonia. Immunotherapy was discontinued due to hypoxia, requiring supplemental oxygen and steroids. A CT scan one month later showed metastatic deposits in the greater omentum, duodenum, and stomach. She is currently alive, three years post-cholecystectomy, but unfortunately has developed brain metastases unresponsive to radiation therapy. She is currently maintained on temozolomide (Temodar, Merck).
Discussion
In the English literature, only nine cases have been reported of either primary gallbladder melanoma without metastatic disease or isolated metastatic melanoma of the gallbladder without an identifiable primary lesion (Table 1) [3-7].
Heath and Womack (1988) proposed criteria for primary gallbladder melanoma, which include a single focus arising from the mucosa with junctional activity and the absence of other primary lesions following a thorough workup. Junctional activity is the most reliable histological indicator of a primary melanoma; however, it may be absent due to rapid tumor growth in true primary cases. It has also been observed in cases of metastatic disease [3]. The presented case exhibits features associated with both primary and metastatic melanoma, as summarized in Table 2.
No further surgical intervention was offered to our patient due to the risk of widespread peritoneal disease associated with gallbladder entry and aspiration, as well as a positive cystic node and features more consistent with metastatic disease, despite some mixed results. Patients with preoperatively diagnosed isolated gallbladder melanoma have a median survival of 39 months, compared to 10 months for those with widespread disease. Additionally, patients who undergo cholecystectomy have a median survival of 19 months, compared to six months for those treated nonoperatively [8]. There is insufficient evidence to recommend an open or laparoscopic approach as long as the gallbladder is not entered and a specimen retrieval bag is used. Katz et al. reported three cases with a laparoscopic approach, two of which had port site recurrence; however, both patients had other sites of disease at the time of surgery. Subsequent cases of laparoscopic cholecystectomy, including our own, have been reported without port site recurrence [9].
Conclusions
Isolated gallbladder melanoma is an extremely rare diagnosis. When identified, the patient should undergo a thorough workup, including an ocular exam, flexible nasopharyngoscopy, EGD/colonoscopy, pelvic exam, dermatological exam, and PET-CT. The specimen should be reviewed by a specialized GI histopathologist, focusing on mucosal involvement and junctional activity, and testing should be conducted for available molecular targets to guide immunotherapy. The case should also be presented to the MDTB. Further surgical intervention should depend on the staging workup, intraoperative gallbladder entry, and the availability of systemic therapy. Most documented cases of isolated gallbladder melanoma occurred before the shift in systemic treatment from chemotherapy to immunotherapy. Future management will likely focus more on actionable aberrant molecular alterations than on the site of origin. In cases of preoperatively identified isolated gallbladder melanoma, surgery should be offered, as it improves both disease-free and overall survival. The choice between minimally invasive or open surgery should be at the discretion of the surgeon. The aim of this case report is to contribute to the literature in this evolving field.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Primary melanoma of the gallbladder: does it exist? Report of a case and review of the literature World J Gastroenterol Safioleas M Agapitos E Kontzoglou K Stamatakos M Safioleas P Mouzopoulos G Kostakis A 425942611220061683038910.3748/wjg.v 12.i 26.4259 PMC 4087388 · doi ↗ · pubmed ↗
- 2Decoding melanoma metastasis Cancers (Basel) Damsky WE Rosenbaum LE Bosenberg M 126163320102421261010.3390/cancers 3010126 PMC 3756353 · doi ↗ · pubmed ↗
- 3Primary malignant melanoma of the gall bladder J Clin Pathol Heath DI Womack C 10731077411988305697810.1136/jcp.41.10.1073 PMC 1141690 · doi ↗ · pubmed ↗
- 4Metastatic melanoma of the gallbladder: report of two cases and a review of the literature Clin Exp Med Giannini I Cutrignelli DA Resta L Gentile A Vincenti L 2953001620162592973610.1007/s 10238-015-0353-6 · doi ↗ · pubmed ↗
- 5Malignant melanoma of the gallbladder: a case report and literature review Ann Hepatobiliary Pancreat Surg Jeon HJ Kwon HJ Kim SG Hwang YJ 4454492520213440245110.14701/ahbps.2021.25.3.445PMC 8382871 · doi ↗ · pubmed ↗
- 6Solitary metastatic gallbladder malignant melanoma originated from the nasal cavity: a case report Int J Surg Case Rep Furumoto K Miyauchi Y Ito D Kitai T Kogire M 965968420132405591910.1016/j.ijscr.2013.08.005PMC 3825965 · doi ↗ · pubmed ↗
- 7Gallbladder metastasis from conjunctival melanoma Clin Nucl Med Cassou-Mounat T Luporsi M Huchet V Jehanno N 0944201910.1097/RLU.000000000000241330516663 · doi ↗ · pubmed ↗
- 8Laparoscopic cholecystectomy for melanoma metastatic to the gallbladder: is it an adequate surgical procedure? Report of a case and review of the literature World J Surg Oncol Marone U CaracòC Losito S 141520071807297210.1186/1477-7819-5-141PMC 2233626 · doi ↗ · pubmed ↗