Case of a 57‐year‐old woman with acute confusion and inability to recognize her husband
Elizabeth Anderson

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
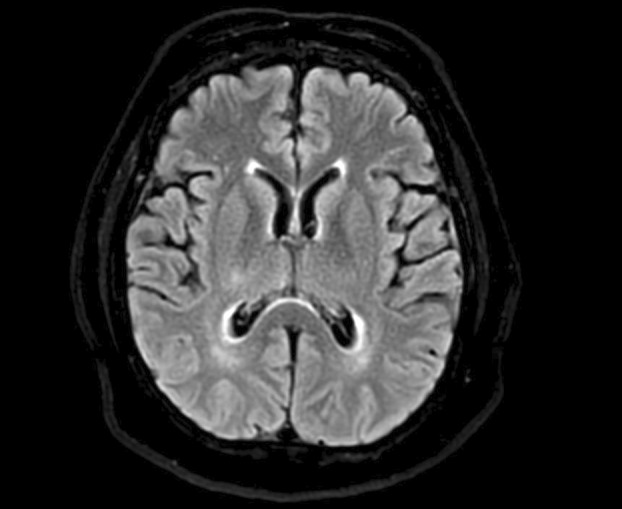 Figure 1
Figure 1| Essential feature |
Dementia; progressive cognitive decline of sufficient enough magnitude to interfere with normal social/occupational functions |
| Core clinical features |
Fluctuating cognition (variations in attention/alertness) Recurrent visual hallucinations (well formed/detailed) REM sleep behavior disorder (can precede cognitive decline) |
| Supportive clinical features |
Severe sensitivity to anti‐psychotic medications Postural instability, repeated falls, syncope or unresponsiveness Severe autonomic dysfunction Hypersomnia or hyposomnia Hallucinations (in other modalities than mentioned) Systematized delusions Apathy, anxiety, or depression |
| Indicative biomarkers |
Reduced dopamine transporter uptake on SPECT or PET Abnormal myocardial scintigraphy Polysomnographic confirmation of REM sleep disorder without atonia |
| Supportive biomarkers |
Relative preservation of medial temporal lobe structures on CT or MRI Generalized low uptake on SPECT or PET perfusion/metabolism scan Prominent posterior slow‐wave activity on EEG with periodic fluctuations in the pre‐alpha/theta range |
|
| |
| Probable DLB | |
|
Two or more core clinical features of DLB are present, with or without the presence of indicative biomarkers, or Only one core clinical feature is present, but with one or more indicative biomarkers | |
| Possible DLB | |
|
Only one core clinical feature of DLB is present, with no indicative biomarker evidence, or One or more indicative biomarkers is present but there are no core clinical features | |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsBody Image and Dysmorphia Studies · Migraine and Headache Studies · Face Recognition and Perception
Summary of Case
Patient is a 57‐year‐old Hispanic female with a past medical history of hypertension, asthma, and type II diabetes mellitus who presented to the emergency room (ER) for evaluation of 7 days of altered mental status. Upon initial presentation, the patient had difficulty following one step commands and was not fully oriented. Additionally, she appeared to be responding to external auditory and visual stimuli. Magnetic resonance imaging (MRI) completed in the ER was without acute intracranial abnormality (Figure 1), and electroencephalogram (EEG) was significant for diffuse slowing but no epileptiform activity was noted. She was admitted to the neurology service for further workup and treatment for possible autoimmune encephalitis, plasma exchange (PLEX), high‐dose steroids, as well as intravenous immunoglobulin (IVIG) treatments. However, despite treatments, the patient continued to remain altered. Therefore, psychiatry was consulted as well as a cognitive specialist. Per patient's husband, he was able to recall that she had in fact had several years of cognitive decline, periods of altered mental status, hallucinations, and slowed gait. During her admission she had periods of not recognizing her husband, and identified him as an imposter, consistent with Capgras syndrome.1 Given clinical findings, our cognitive team determined the patient's most likely diagnosis and started her on rivastigmine 1.5 mg bid with improvement.2
Diagnosis
Lewy body dementia.
Take‐Home Points
- It is important to elicit a thorough history from family members and other collateral, including medications, comorbidities, and duration of symptoms when patients present with change in mental status.
- Lewy body dementia can be difficult to recognize clinically, as it is often insidious in onset and can present similarly to other conditions. However, to make a diagnosis of probable dementia with Lewy bodies, in addition to dementia, two additional features must be present, which include cognitive fluctuations, visual hallucinations, REM sleep behavior disorder, and parkinsonism.3
- To aid in diagnosis, one can utilize the revised criteria for the clinical diagnosis of probable and possible dementia with Lewy bodies (DLB), which is set of clinical features and biomarkers used to identify if cognitive decline is secondary to Lewy body pathology (Table 1).
- Once recognized clinically, treatment of Lewy body dementia is supportive, and includes cholinesterase inhibitors, memantine, and levodopa. New‐generation medications are also being introduced to help with psychosis/hallucinations. However, there are currently no preventative treatments for this disease process.2
MRI brain w/wout contrast. Notable for chronic lateral right thalamic infarct, mild generalized volume loss. No acute intracranial abnormality. Ambra Imaging, Dignity Health Systems/St. Joseph Hospital Medical Center.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Josephs KA . Capgras syndrome and its relationship to neurodegenerative disease. Arch Neurol. 2007;64(12):1762‐1766. doi:10.1001/arch-neur.64.12.1762 18071040 · doi ↗ · pubmed ↗
- 2Taylor JP , Mc Keith IG , Burn DJ , et al. New evidence on the management of Lewy body dementia. Lancet Neurol. 2020;19(2):157‐169.31519472 10.1016/S 1474-4422(19)30153-XPMC 7017451 · doi ↗ · pubmed ↗
- 3Jellinger KA . Dementia with Lewy Bodies and Parkinson's disease‐dementia: current perspectives. Int J Neurol Neurother. 2018;5:615‐650. doi:10.23937/2378-3001/1410076 29222591 · doi ↗ · pubmed ↗
- 4Raffa S , Donegani MI , Borra A , et al. Role of [18F]‐FDG PET in patients with atypical parkinsonism associated with dementia. Clin Translat Imaging. 2020;8:107‐122.
- 5Caminiti SP , Sala A , Iaccarino L , et al. Brain glucose metabolism in Lewy body dementia: implications for diagnostic criteria. Alzheimers Res Ther. 2019;11:20.30797240 10.1186/s 13195-019-0473-4PMC 6387558 · doi ↗ · pubmed ↗
- 6Schneider Williams S . The terrorist inside my husband's brain. Neurology. 2016;87:1308‐1311. doi:10.1212/WNL.0000000000003162 27672165 · doi ↗ · pubmed ↗
- 7Cuadrado‐Corrales N , Jimenez‐Huete A , Hortigüela R , et al. Impact of the clinical context on the 14–3‐3 test for the diagnosis of sporadic CJD. BMC Neurol. 2006;6:25.16872484 10.1186/1471-2377-6-25PMC 1570138 · doi ↗ · pubmed ↗
- 8Galvin JE . Lewy body dementia. Pract Neurol. 2019;67‐71.