Direct and indirect relationships between Food Parental Practices, diet quality, and food satisfaction in adolescents
Carola Del Valle, Horacio Miranda, Ligia Orellana, Cristian Adásme-Berrios, Cristina Calvo-Porral, Berta Schnettler

TL;DR
This study explores how parental feeding practices influence adolescents' food satisfaction, either directly or through their impact on diet quality.
Contribution
The study identifies diet quality as a mediator between specific parental practices and adolescent food satisfaction.
Findings
Diet quality mediates the relationship between parental modeling and adolescent control over food satisfaction.
Monitoring and restrictive practices for weight control have a direct effect on food satisfaction.
Parental feeding practices are linked to adolescent food satisfaction through both direct and indirect pathways.
Abstract
The relationship between four parental feeding practices from the Comprehensive Feeding Practices Questionnaire for adolescents (CFPQ-Teen) and Satisfaction With Food-related Life (SWFoL) in adolescents was evaluated using diet quality measured using the Adapted Healthy Eating Index (AHEI) as a mediating variable. Participants were 860 adolescents aged 10–16 years of both sexes who responded to four factors on the CFPQ-Teen, food satisfaction scale, and diet quality index. Structural equation analysis was used in a structural mediation model on a polychoric correlation matrix using the weighted least squares mean-variance adjusted (WLSMV) method. Diet quality was a mediating factor in the interaction between two parental practices related to parental modeling and adolescent control over SWFoL. There was evidence of a direct relationship between monitoring and restrictive factors for…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
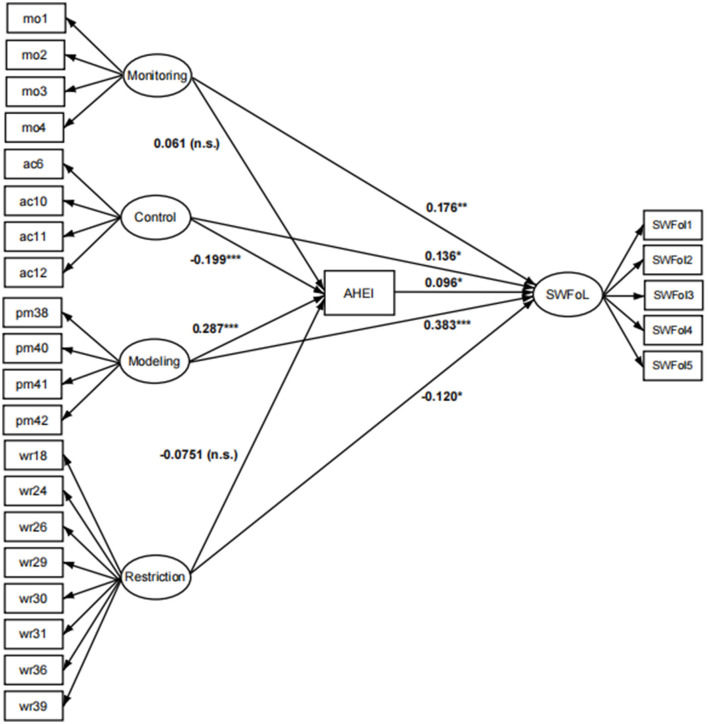 Figure 1
Figure 1|
|
|
|---|---|
|
| |
| Male | 13.04 (2.05) |
| Female | 13.28 (2.02) |
|
| |
| Male | 50.5 |
| Female | 49.5 |
| Family members [mean (SD)] | 4.38 (1.36) |
| Number of children [mean (SD)] | 2.18 (0.87) |
|
| |
| High | 5.0 |
| Medium | 81.3 |
| Low | 13.7 |
| SWFoL [mean (SD)] | 23.37 (4.77) |
| Monitoring [mean (SD)] | 13.79 (4.75) |
| Adolescent control [mean (SD)] | 10.55 (3.43) |
| Parental modeling [mean (SD)] | 15.07 (3.79) |
| Restriction for weight control [mean (SD)] | 22.18 (8.06) |
| AHEI [mean (SD)] | 63.58 (13.97) |
|
|
|
|---|---|
| Monitoring | |
| Adolescent control | |
| Restriction for weight control | |
| Parental modeling | |
|
|
|
|
|
|
|
|
|
|---|---|---|---|---|---|---|---|
| Monitoringa | 0.071** | 0.068** | 0.294 | 0.008* | 0.002 | −0.001 | 0.008 |
| Monitoringb | 0.182 | 0.176 | 0.061 | 0.096 | 0.006 | −0.006 | 0.017 |
| Controla | 0.083*** | 0.097** | −1.738*** | 0.008* | −0.014 | −0.030 | −0.001 |
| Controlb | 0.117 | 0.136 | −0.199 | 0.096 | −0.019 | −0.038 | −0.001 |
| Modelinga | 0.371*** | 0.346*** | 3.193*** | 0.008* | 0.025 | 0.003 | 0.049 |
| Modelingb | 0.410 | 0.383 | 0.287 | 0.096 | 0.027 | 0.003 | 0.052 |
| Restrictiona | −0.174* | −0.164* | −1.259 | 0.008* | −0.010 | −0.027 | 0.001 |
| Restrictionb | −0.127 | −0.120 | −0.075 | 0.096 | −0.007 | −0.018 | 0.003 |
|
|
|
|
| |||||
|---|---|---|---|---|---|---|---|---|
|
|
|
|
|
| ||||
| Direct | Monitoring | → | SWFoL | 0.176 | 0.068** | H1: Confirming | ||
| Direct | Monitoring | → | AHEI | 0.061 | 0.294 | H2: Rejecting | ||
| Indirect | Monitoring | → | AHEI | → | SWFoL | 0.006 | 0.002 | H9: Rejecting |
| Direct | Control | → | SWFoL | 0,136 | 0.097** | H3: Confirming | ||
| Direct | Control | → | AHEI | −0.199 | −1.738*** | H4: Confirming | ||
| Indirect | Control | → | AHEI | → | SWFoL | −0.019 | −0.014* | H9: Confirming |
| Direct | Modeling | → | SWFoL | 0.383 | 0.346*** | H5: Confirming | ||
| Direct | Modeling | → | AHEI | 0.287 | 3.193*** | H6: Confirming | ||
| Indirect | Modeling | → | AHEI | → | SWFoL | 0.027 | 0.025 | H9: Confirming |
| Direct | Restriction | → | SWFoL | −0.120 | −0.164* | H7: Confirming | ||
| Direct | Restriction | → | AHEI | −0.075 | −1.259 | H8: Rejecting | ||
| Indirect | Restriction | → | AHEI | → | SWFoL | −0.007 | −0.010 | H9: Rejecting |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsObesity, Physical Activity, Diet · Psychological Well-being and Life Satisfaction · Food Security and Health in Diverse Populations
1 Introduction
The population is becoming more aware of the association between healthy eating habits and better health and wellbeing (1). Hence, understanding the factors that influence adolescents' quality of life and wellbeing is increasingly necessary to develop strategies to improve this condition in the early stages of life (2). In the area of food, quality of life has been measured through the Satisfaction With Food-related Life (SWFoL) scale, which assesses people's subjective perception of wellbeing regarding their eating habits (3).
In recent decades, life expectancy has increased considerably, but this has been accompanied by non-communicable diseases such as those associated with overweight and obesity (4). It is a major public health problem for all cultures and age groups (5). Although autonomy in food choices increases during adolescence, adolescents still depend on the food provided by parents and Food Parental Practices (FPP) in which parents exercise at home (6). FPP refer to the specific eating habits parents use to influence what, when, and how much their children eat (7), both during and between meals (8). Healthy eating habits refer to different conditions, such as appropriate times for food intake, hydration, and a varied and healthy diet in portions that correspond to each person according to their age, sex, physical activity, and other contextual variables (9).
A healthy diet is based on one that provides the nutrients that the body needs for its proper functioning, considering the amount of calories, proteins, carbohydrates, lipids, water, and fiber depending on different variables such as age, sex, and stage. Among other conditions, the estimation of a healthy diet can be facilitated by grouping foods based on their nutritional value (e.g., fruits and vegetables, cereals, dairy products, and meat) (10). An unhealthy diet is characterized by an imbalance in the consumption of these nutrients, excessive intake of trans- and saturated fatty meats, refined cereals, high levels of sodium and simple sugars, and deficiency in fruits and vegetables.
In the family context, recent studies have shown that healthy FPP in adolescents can have a positive impact on eating habits (11, 12). FPP, including monitoring and parental modeling, have been associated with improved diet quality in adolescents in various countries (7, 13–17). However, other FPP, such as restriction of weight control, have been associated with unhealthy diets and higher weight (43). Other studies have reported a negative association between adolescent control and diet quality, because parents control less of what adolescents eat in response to their quest for autonomy in food choice (11), leading to a decrease in adolescents' diet quality (44).
Variables that are positively related to higher SWFoL include healthy eating habits and better diet quality (7, 13, 16–19). Similarly, several studies have suggested a positive association between the FPP that parents apply for home and SWFoL (20, 21). In addition, Vaughn et al. (22) suggested that there is evidence linking structural FPP with non-obesogenic environments, whereas McGowan et al. (23) asserted that the monitoring factor acts as a predictor of fruit consumption.
The background presented indicates that diet quality is associated with FPP and SWFoL in adolescents, and that FPP are also associated with SWFoL. However, the relationships between FPP, diet quality, and SWFoL have not been explored.
The CFPQ-Teen was used, which Piccoli et al. (6) adapted to Portuguese, to measure the perception of FPP in Brazilian adolescents. This study used four latent factors—monitoring, parental modeling, weight control restriction, and adolescent control—adapted and validated by Del Valle et al. (43) to be answered by teenagers in Chile.
Based on the above, this study aimed to assess the direct and indirect relationships between the four FPP on the CFPQ-Teen and SWFoL mediated by the AHEI in adolescents in two cities in Chile.
Based on the study objectives, the following hypotheses were established:
H1: Monitoring FPP are directly and positively associated with SWFoL in adolescents.H2: Monitoring FPP are directly and positively associated with AHEI in adolescents.H3: Adolescent control of FPP are directly and negatively associated with SWFoL.H4: Adolescent control of FPP are directly and negatively associated with AHEI.H5: Parental modeling of FPP are directly and positively associated with SWFoL in adolescents.H6: Parental modeling of FPP are directly and positively associated with AHEI in adolescents.H7: Restriction of weight control of FPP are directly and negatively associated with SWFoL in adolescents.H8: Restriction of weight control of FPP are directly and negatively associated with diet quality in adolescents.H9: The AHEI has an indirect relationship with the CFPQ-Teen FPP and SWFoL in adolescents.
2 Methods
2.1 Sampling and procedure
The participants were selected through proportional quota sampling in order to access a sample that reflected the communal distribution of families according to socioeconomic level (high, medium, and low) in Temuco and Santiago, Chile. Prior to data collection, parents were asked to sign a consent form authorizing the participation of a child. The children were asked to sign the consent form. Consent and assent will ensure voluntary participation and endorse the confidentiality and anonymity of the data obtained. The inclusion criteria for this study stipulated that the participants were adolescents aged 10–16 years who came from households with one father and one mother, each of whom contributed to household income. Participants were recruited through contact with the authorities of educational establishments located in urban areas between March and July 2021 in Santiago (n = 430) and between July and December 2021 in Temuco (n = 430), Chile. The questionnaires were hosted on the QuestionPro platform (QuestionPro Inc.) and were sent by email to the adolescents' mothers by previously trained interviewers. After receiving the completed questionnaire, each family received USD 15. The Ethics Committee of the University of La Frontera approved the study protocol (Protocol Number 007/2019).
2.2 Instruments
In this study, a four-factor model of the CFPQ-Teen was used, adapted, and validated by Del Valle et al. (43) to be answered by adolescents. This model is composed of 20 items representing four factors of the CFPQ-Teen, which are represented by four items that assess adolescents' perception of the frequency with which parents monitor the consumption of unhealthy foods; the adolescent control factor is represented by four items that assess the frequency with which parents are more permissive concerning adolescent eating behavior and habits; the weight control restriction factor is represented by eight items that assess adolescents' perception of control over food intake to reduce or maintain their weight; and the parental modeling factor is represented by four items that determine how adolescents perceive their parents as a model or reference for them in terms of healthy eating habits. Del Valle et al. (43) obtained the following McDonald's omega for each factor of the Spanish-validated model: Monitoring = 0.91, Adolescent Control = 0.69, Restriction for Weight Control = 0.90, and Parental Modeling = 0.83.
Adolescent control factor items (e.g., “Do your parents allow you to eat whatever you want?”) and Monitoring [e.g., “How often do your parents check the number of sweets (or ice cream, cakes, chocolates, candies, pies, pastries) you eat?”] were answered on a 5-point Likert-type scale, from 1 “never” to 5 “always.” The factors Restrictions for weight control (e.g., “Do my parents need to be sure I don't eat high-fat foods?”) and parental modeling (e.g., “My parents eat healthy food to give me an example of healthy eating.”) were answered on a 5-point Likert-type scale, from 1 “strongly disagree” to 5 “strongly agree” (Supplementary Table 1).
The Adapted Healthy Eating Index (AHEI) is an adaptation of the US-HEI (10) developed by Norte and Ortiz (24) for the qualitative estimation of diet quality in Spanish-speaking populations. Participants were asked to respond to the AHEI variables indicating the frequency of consumption of the nine food groups: (1) Cereals and by-products, (2) Vegetables, (3) Fruits, (4) Milk and dairy products, (5) Meats, (6) Legumes, (7) Cold cuts and sausages, (8) Sweets, (9) Sugary drinks, and (10) Varieties of diets. The consumption frequency data for each food group were converted into a score from 0 to 10, according to the degree of compliance with the dietary recommendations. The AHEI score was calculated by adding the scores for each variable. The AHEI variable scores add up to a maximum of 100 points. Scores over 80 are indicative of a “healthy” diet; scores between 51 and 80 correspond to a diet that “requires change”; scores below 50 correspond to “unhealthy” diets (10) (Supplementary Table 2).
Satisfaction With Food-related Life (SWFoL) (3) comprises five items grouped into a single dimension that assesses a person's subjective perception of wellbeing concerning food and eating habits. The validated Spanish version of the SWFoL used in this study (25) showed good internal consistency in samples of adolescents in Chile (Cronbach's α = 0.89–0.91) (20, 26–28). Respondents indicated their degree of agreement with each statement on a 6-point Likert scale (e.g., food and meals offer great satisfaction in your daily life) from 1 “completely disagree” to 6 “completely agree” (Supplementary Table 3).
2.3 Data analysis
This study used a cross-sectional, nonexperimental, descriptive, correlational, and functional dependency design. Statistical Package for the Social Sciences (IBM SPSS) v. 23 was used for descriptive analyses.
The Mplus v. 8.4. software was used to analyze the structural mediation model. The weighted least squares mean-variance adjusted (WLSMV) method was used to estimate the parameters of this model, considering the ordinal response scale of the items and the optimization of the standard errors of the PATH (8, 29–32, 42).
The mediation effect was evaluated through structural equation modeling using AHEI as the mediating variable between the four factors on the CFPQ-Teen and SWFoL. The statistical significance of indirect associations in the model was verified through confidence intervals using the bootstrap method with an estimation of 5,000 iterations (33). The global and incremental goodness-of-fit indicators of the structural model, RMSEA, CFI, and TLI, were estimated using WLSMV to analyze non-normally distributed data (34).
3 Results
3.1 Descriptive analysis
The sample of 860 adolescents in Santiago and Temuco comprised 434 male and 426 female adolescents was composed of 50.5% male adolescents and 49.5% female adolescents, with a mean age of the adolescents of 13.04 (SD = 2.05) and adolescents 13.28 (SD = 2.02). The families had a mean number of family group members of 4.38 (SD = 1.36), and families with a medium socioeconomic level (81.3%). The SWFoL variable had a mean of 23.37 (SD = 4.77), the CFPQ-Teen factors presented means of Monitoring of 13.79 (SD = 4.75), adolescent control of 10.55 (SD = 3.43), parental model of 15.07 (SD = 3.79), and weight control restriction of 22.18 (SD = 8.06). The AHEI presented a mean of 63.58 (SD = 13.97). The AHEI measurement in adolescents showed that 10.58% of the participants of both sexes presented a “healthy” diet, while 72.56% “require changes” in their diet, and 16.86% had an “unhealthy diet” (Table 1).
3.2 Relationships between FPP, diet quality, and food satisfaction
This study's structural mediation model presented medium to high goodness-of-fit levels: CFI: 0.914, TLI: 0.902, and RMSEA: 0.065. Convergent validity demonstrated that all saturations were statistically significant (p ≤ 0.05).
The four independent factors of the CFPQ-Teen questionnaire with the description of all indicator variable names (mo1 to wr39) and their relations with theory are found in Table 2.
The PATH values and statistical significances of the direct and indirect relationships between the CFPQ-Teen factors with SWFoL and AHEI are shown in Figure 1.
Standardized structural diagram of the model relating four parental feeding practices from the CFPQ-Teen, feeding quality (measured with the AHEI), and Satisfaction with food-related life (SWFoL) in adolescents. Monitoring = mo01, 02, 03, 04; Adolescent Control = ac05, 06, 10, 11; Parental Modeling = pm38, 40, 41, 42; Restriction for weight control = wr18, 24, 26, 29, 30, 31, 36, 39. Statistical significance: * p-value ≤ 0.05, ** p-value ≤ 0.01, *** p-value ≤ 0.001.
The monitoring factor showed a positive and highly significant direct relationship with SWFoL 0.068 (p ≤ 0.01), thus confirming H1, which establishes a positive relationship between monitoring and SWFoL in adolescents, and showed a positive and non-significant relationship with diet quality, 0.294 (p > 0.05), thus rejecting H2. The indirect effect of SWFoL through AHEI was positive and insignificant, as it included zero at 95% CI 0.002 (−0.001; 0.008), which ruled out H9; therefore there would be no indirect relationship of monitoring on SWFoL mediated by the AHEI.
The adolescent control factor showed a positive and highly significant direct relationship with SWFoL 0.097 (p ≤ 0.01); this confirms the significance but not the direction of the relationship in H3, which was negative, so that the control factor would positively influence food satisfaction in adolescents. Also the factor adolescent control showed a negative and very highly significant relationship with the AHEI, −1.738 (p ≤ 0.001), which confirms H4 that establishes that there is a negative and significant relationship between monitoring and the AHEI. The indirect relationship between adolescent control and SWFoL through the AHEI was negative and significant, as it did not include zero, with a 95% CI of −0.014 (−0.030; −0.001), confirming H9 that there would be an indirect relationship between adolescent control and SWFoL mediated by the AHEI.
The parental modeling factor showed a positive and highly significant direct relationship with SWFoL 0.346 (p ≤ 0.001), thus confirming H5, which establishes a positive relationship between the parental modeling factor and SWFoL in adolescents, as well as a positive and highly significant relationship with el AHEI 3.193 (p ≤ 0.001), confirming H6, which establishes that there is a positive and significant relationship between parental modeling and AHEI. The indirect relationship between the parental modeling factor and SWFoL through the AHEI was positive and significant, as it did not include zero with a 95% CI of 0.025 (0.003; 0.049), confirming H9 that there would be an indirect parental modeling factor relationship on SWFoL mediated by the AHEI.
The restriction for weight control factor showed a negative and significant direct relationship with SWFoL −0.164 (p ≤ 0.05), thus confirming H7, which establishes a negative and significant relationship between restriction for weight control factor and SWFoL in adolescents; also, the restriction for weight control factor showed a negative and non-significant relationship with the AHEI, −1.259 (p > 0.05), thus rejecting H8. The indirect relationship with SWFoL through AHEI was negative and insignificant, as it included zero at a 95% CI of −0.010 (−0.027; 0.001), thus rejecting H9. Therefore, there would be no indirect relationship between the restriction of weight control factors and SWFoL mediated by the AHEI (Table 3).
The relationships between the factors and the PATH estimated for each hypothesis are shown in Table 4.
4 Discussion and conclusion
This study aimed to assess the direct and indirect relationships between four FPP on the CFPQ-Teen and SWFoL mediated by the AHEI in adolescents in two cities in Chile. When this study was conducted, to the best of the authors' knowledge, no study had been reported that used a structural equation model to analyze the relationship of diet quality mediated through the AHEI between four FPP on the CFPQ-Teen and the SWFoL.
Regarding H1, which states that FPP Monitoring is positively associated with SWFoL in adolescents, the results observed in the sample presented a positive and statistically significant relationship, which allows us to confirm H1, concluding that the monitoring factor improves SWFoL in adolescents.
In relation to H2, which states that Monitoring FPP are positively associated with AHEI in adolescents, the results observed in the sample present a non-significant relationship, which allowed H2 to be rejected, concluding that the monitoring factor does not present an indirect relationship with SWFoL through AHEI. This result contrasts with those of studies that associate FPP with better diet quality (7, 16). This finding may be due to adolescents at this stage of life exhibiting maladaptive eating behaviors (35) and disordered eating habits (36), leading to a decrease in diet quality (37–39). Maladaptive eating behaviors in adolescence can be partially attributed to the increased autonomy and independence attained during this developmental stage, including dietary choices (6, 11).
In relation to H3, which states that Adolescent control FPP are negatively associated with SWFoL in adolescents, the results observed in the sample presented a direct positive relationship, which is in contrast with the direction of H3, concluding that the adolescent control factor improves SWFoL.
In relation to H4, which states that Adolescent control FPP is negatively associated with AHEI in adolescents, the results observed in the sample allowed H4 to be preserved, evidencing a direct and negative relationship with the AHEI, concluding that the relationship of the adolescent control factor on SWFoL presents a suppression mediation relationship through the AHEI. The indirect relationship between the adolescent control factor and SWFoL via the AHEI corresponds to a suppression-type relationship, given that the direct relationship was greater than the total relationship, and there were also relationships with opposite signs with the AHEI and between the AHEI and SWFoL (40).
In relation to H5, which states that Parental modeling of FPP are positively associated with SWFoL in adolescents, the results observed in the sample presented a positive and statistically significant relationship, which allows us to confirm H5, concluding that the parental modeling factor improves SWFoL in adolescents. These results are consistent with studies that have shown that FPP, such as parental modeling for adolescents, can have a positive impact on diet quality (11, 12, 14).
In relation to H6, which states that Parental modeling FPP are positively associated with AHEI in adolescents, the results observed in the sample presented a positive and statistically significant relationship, which allows us to confirm H6, concluding that the parental modeling factor is related to the SWFoL indirectly and partially through AHEI in adolescents.
In relation to H7, which states that Restriction for weight control FPP are negatively associated with SWFoL in adolescents, the results observed in the sample presented a negative and statistically significant relationship, which allowed us to confirm H7, concluding that factor restriction for weight control reduces SWFoL in adolescents.
In relation to H8, which states that the Restriction for weight control FPP is negatively associated with AHEI in adolescents, the results observed in the sample present a non-significant relationship, which allowed H8 to be rejected, concluding that the factor restriction for Weight control does not present an indirect relationship with SWFoL through AHEI.
In this study, there were no statistically significant differences in the indirect relationship between weight control restriction and SWFoL mediated by the AHEI. This aligns with other research indicating that adolescents tend to reject coercive FPP, which is linked to increased body weight (7, 41).
In relation to H9, which states that AHEI has an indirect relationship between CFPQ-Teen FPP and SWFoL in adolescents, the results observed in the sample presented indirect and significant relationships; the AHEI fulfills a mediating role only through adolescent control and parental modeling factors on the CFPQ-Teen with SWFoL.
Based on the results, it can be concluded that the four factors of the CFPQ-Teen have a direct relationship with the SWFoL. There was evidence of an indirect relationship between adolescent control and parental modeling and SWFoL through the AHEI. Consequently, while all four FPP evaluated are associated with adolescents' subjective wellbeing in the dietary domain, only two exert an indirect influence through AHEI. Adolescent control has a negative association with AHEI because parents control what adolescents eat less in response to their search for autonomy in food choice (11), reducing the quality of their adolescents' diet (44). The parental modeling factor was associated with better diet quality in adolescents, which is consistent with previous studies with samples of adolescents from different countries (7, 13–17, 41).
A remarkable aspect of this study is that it was conducted with a large sample size (n = 860), which resulted in greater accuracy in estimating the parameters and global and incremental psychometric goodness-of-fit indices. This study used a polychoric correlation matrix for categorical variables with an ordinal Likert-type response by applying the WLSMV method to optimize the standard error of estimating saturations in structural equation model analyses.
The limitations of this study include the fact that the AHEI does not measure the amount of food consumed or energy value, nor does it consider contextual variables, such as ethnicity, parental educational level, age, etc. The AHEI measures the frequency of consumption by food groups, which is considered an indicator of diet quality and nutritional health (24). Also provides evidence on the food consumption pattern in the country that applies (10). In Chile it is used by the Ministry of Health to measure the quality of the population's diet and has been used in numerous studies in adolescents (14, 15).
This study contributes to the application of research on eating behavior, generating a contribution to public health, specifically at the level of the Ministry of Health, health institutions, and educational institutions, to generate educational strategies for the application of healthy eating habits. Different interventions, considering that the AHEI provides evidence of the type of foods consumed, allow the construction of dietary guides to direct nutritional education in a more comprehensive way through nutritional assistance programs applied to adolescents and their parents to reduce obesity in adolescents in Chile. The study of perceptions about contributes to the construction of scenarios that include the mediating effect of the AHEI and its implications on SWFoL, considering eating habits in the orientation of the food industry in governmental and non-governmental organizations. These results constitute a relevant contribution to advance future research that promotes healthy eating habits in families with adolescent children in Latin America.
This shows the importance of including diet quality as a mediating variable in the relationship between CFPQ-Teen factors, parental model, weight control restriction, and SWFoL. This impacts structural models in future studies by necessitating the inclusion of the AHEI in the examination of FPP and SWFoL among adolescents.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1de Albuquerque Araújo LÁlvarez HAJ Palomo GI Bustamante UMA. Determinantes de la satisfacción con la alimentación en adultos mayores chilenos [Determinants of satisfaction with food-related life in older Chileans adults]. Nutr Hosp. (2019) 36:805–12. 10.20960/nh.0248131232574 · doi ↗ · pubmed ↗
- 2Liu R Grunert KG. Satisfaction with food-related life and beliefs about food health, safety, freshness and taste among the elderly in China: a segmentation analysis. Food Qual Prefer. (2020) 79:103775. 10.1016/j.foodqual.2019.103775 · doi ↗
- 3Grunert KG Dean M Raats MM Nielsen NA Lumbers M. A measure of satisfaction with food-related life. Appetite. (2007) 49:486–93. 10.1016/j.appet.2007.03.01017481776 · doi ↗ · pubmed ↗
- 4Fernandes DPS Lopes Duarte MS Pessoa MC Castro Franceschini SC Queiroz Ribeiro A. Healthy Eating Index: assessment of the diet quality of a Brazilian elderly population. Nutr Metab Insights. (2018) 11:117863881881884. 10.1177/117863881881884530626998 PMC 6311538 · doi ↗ · pubmed ↗
- 5Adasme-Berrios C Carreño C Aliaga-Ortega L Schnettler B Lobos G. Factores que determinan la elección de alimentos procesados por estudiantes universitarios en el contexto de las etiquetas de advertencia nutricional. Rev Chil Nutr. (2022) 49:451–8. 10.4067/S 0717-7518202200050045127315006 · doi ↗
- 6PiccoliÂB Neiva-Silva L Mosmann CP Musher-Eizenman D Pellanda LC. Adolescents' perception of parental feeding practices: adaptation and validation of the comprehensive feeding practices questionnaire for Brazilian adolescents-The CFPQ-Teen. P Lo S ONE. (2017) 12:e 0187041. 10.1371/journal.pone.018704129145485 PMC 5690605 · doi ↗ · pubmed ↗
- 7Costarelli V Michou M Panagiotakos DB Lionis C. Adherence to the Mediterranean diet and weight status in children: the role of parental feeding practices. Int J Food Sci Nutr. (2021) 72:112–22. 10.1080/09637486.2020.176515132458711 · doi ↗ · pubmed ↗
- 8Yang WY Burrows T Mac Donald-Wicks L Williams LT Collins CE Chee WSS. Parent-child feeding practices in a developing country: findings from the Family Diet Study. Appetite. (2018) 125:90–7. 10.1016/j.appet.2018.01.03729408380 · doi ↗ · pubmed ↗