A comprehensive evaluation system for ultrasound-guided infusion of human umbilical cord-derived MSCs in liver cirrhosis patients
Guo Zhou, Yijuan You, Binghua Wang, Simin Wang, Tianhang Feng, Chunyou Lai, Guangming Xiang, Ke Yang, Yutong Yao

TL;DR
This study evaluates a new method for delivering stem cells to treat liver cirrhosis using an improved catheter system guided by ultrasound.
Contribution
The study introduces an improved catheter technique for safer and more effective stem cell delivery in liver cirrhosis patients.
Findings
The new catheter method successfully delivered hUC-MSCs to the portal vein in liver cirrhosis patients.
Liver fibrosis and damage markers significantly decreased after hUC-MSCs transplantation.
Liver biopsy showed reduced hepatocyte necrosis and improved liver stiffness after treatment.
Abstract
Infusion of mesenchymal stem cells (MSCs) via portal vein is one of the main ways for MSCs transplantation to treat liver cirrhosis (LC). As the tissue of LC showed diffuse fibrosis and thickened Glission sheath, the soft pig-tail catheter, or central venous catheter can not successfully insert the portal vein. Thus, our study used an improved method and performed a relatively comprehensive system to evaluate the effect for human umbilical cord-derived mesenchymal stem cells (hUC-MSCs) transplantation. Fifteen patients with hepatitis B-related cirrhosis were enrolled in the study, and we performed hUC-MSCs transplantation via portal vein by using an 16-G needle and 0.035-inch guide wire combined with 7FR “retentional metal stiffner trocar” of pig-tail catheter under the guidance of contrast-enhanced ultrasound. Serum liver function, fibrotic indicators, tissue stiffness, coagulation…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
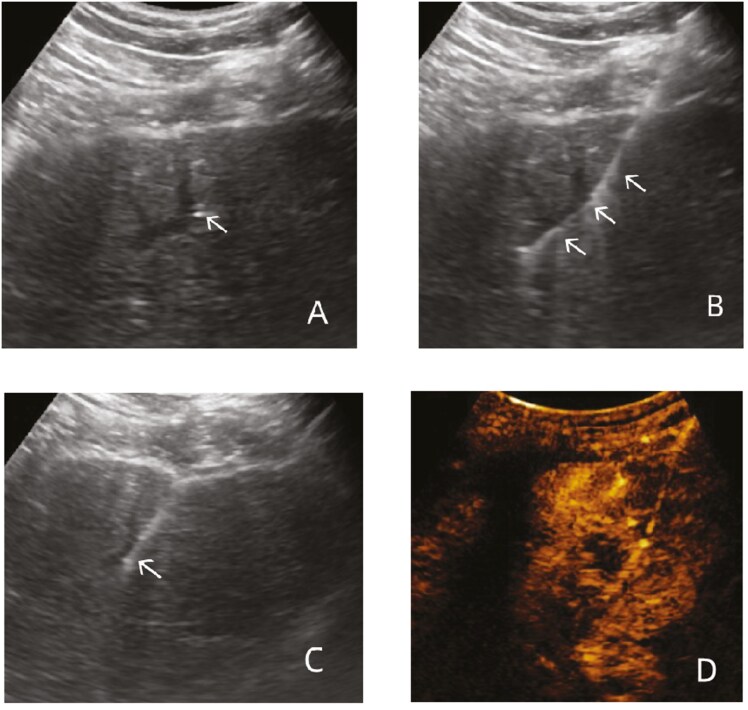 Figure 1
Figure 1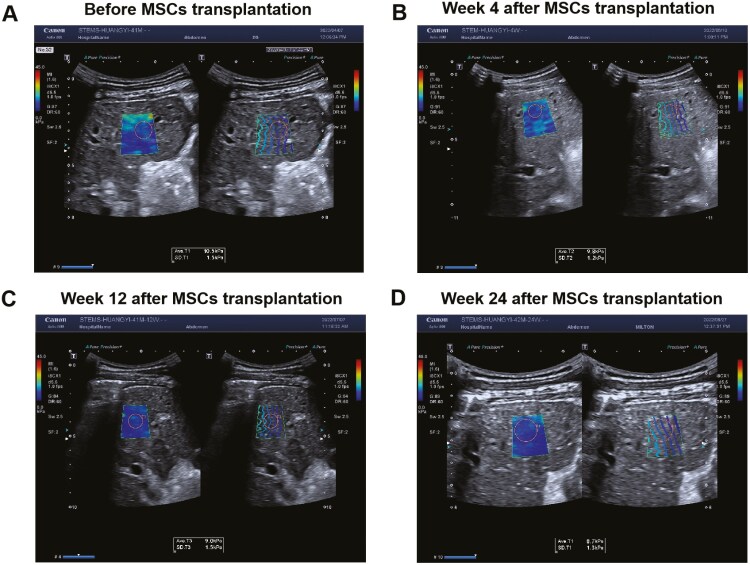 Figure 2
Figure 2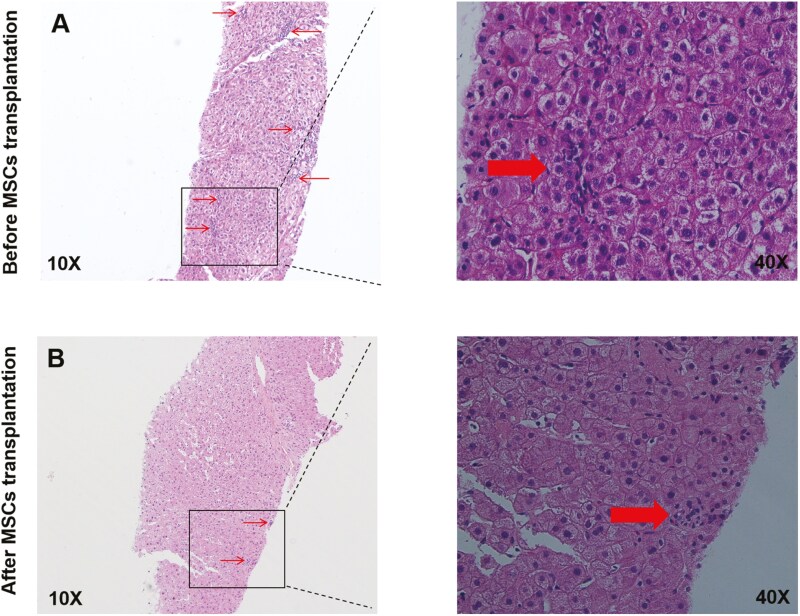 Figure 3
Figure 3| Serum indicators | Before MSCsT | Week 4 after MSCsT | Week 12 after MSCsT | Week 24 after MSCsT |
|
|
|---|---|---|---|---|---|---|
|
| ||||||
| ALT (U/L) | 28.00 ± 12.28 | 29.93 ± 10.71 | 27.80 ± 6.89 | 28.07 ± 9.11 | 0.301 | .824 |
| AST (U/L) | 32.47 ± 8.12 | 31.53 ± 10.53 | 31.8 ± 8.69 | 31.8 ± 8.81 | 0.088 | .966 |
| TBIL (umol/L) | 23.35 ± 13.06 | 19.30 ± 9.41 | 16.40 ± 9.94 | 19.55 ± 15.49 | 2.133 | .149 |
| ALB (g/L) | 45.83 ± 4.32 | 44.26 ± 5.37 | 45.34 ± 4.59 | 46.39 ± 5.80 | 1.474 | .235 |
|
| ||||||
| PT(s) | 13.02 ± 1.45 | 12.73 ± 0.93 | 12.67 ± 0.99* | 12.53 ± 1.13* | 3.22 | .03 |
| PTA(%) | 75.83 ± 12.06 | 78.35 ± 10.86 | 79.30 ± 9.29 | 67.22 ± 21.41 | 2.07 | .16 |
| APTT(s) | 26.33 ± 2.57 | 27.30 ± 2.06 | 27.11 ± 1.27 | 25.98 ± 7.39 | 1.64 | .23 |
| FIB (g/L) | 2.28 ± 0.35 | 2.31 ± 0.53 | 2.27 ± 0.29 | 2.31 ± 0.35 | 0.06 | .98 |
|
| ||||||
| HA (ng/mL) | 295.84 ± 95.09 | 286.67 ± 91.76 | 285.85 ± 80.82 | 259.17 ± 85.16 | 3.59 | .04 |
| LN (ng/mL) | 154.38 ± 46.3 | 154.89 ± 40.28 | 150.59 ± 54.36 | 149.44 ± 45.97 | 0.31 | .82 |
| IV-C (ng/mL) | 148.59 ± 22.22 | 149.85 ± 27.69 | 135.86 ± 29.57 | 130.94 ± 35.80 | 2.90 | .04 |
| PCIIINP (ng/mL) | 21.44 ± 7.02 | 21.41 ± 6.84 | 19.57 ± 7.21 | 21.44 ± 7.54 | 1.12 | .35 |
| Time | Liver Young’s modulus (KPa) |
|---|---|
| Before MSCsT | 10.36 ± 1.52 |
| Week 4 after MSCsT | 10.05 ± 1.49 |
| Week 12 after MSCsT | 10.19 ± 1.57 |
| Week 24 after MSCsT | 9.69 ± 1.21 |
| F | 3.23 |
| P | 0.03 |
| Time | Clastic necrosis | Fusion necrosis | Lytic necrosis | Portal inflammation | Score of fibrosis stage |
|---|---|---|---|---|---|
| Before MSCsT | 2.00(1.00,3.00) | 0.00(0.00,0.00) | 2.00(1.00,2.00) | 2.00(1.00,2.00) | 5.00(5.00,6.00) |
| Week 24 after MSCsT | 2.00(2.00,3.00) | 0.00(0.00,0.00) | 1.00(1.00,2.00) | 2.00(1.00,2.00) | 2.00(4.00,5.00) |
| Z | 0.45 | 0.82 | 2.11 | 1.00 | 1.40 |
| P | 0.66 | 0.41 | 0.04 | 0.32 | 0.16 |
| Liver hemodynamics | Before MSCsT | Week 4 | Week 12 | Week 24 | F |
|
|---|---|---|---|---|---|---|
|
| 1.13 ± 0.22 | 1.16 ± 0.17 | 1.11 ± 0.21 | 1.04 ± 0.21 | 3.14 | .04 |
|
| 15.90 ± 5.89 | 16.98 ± 4.59 | 15.54 ± 3.97 | 16.98 ± 4.86 | 0.67 | .57 |
|
| ||||||
|
| 50.05 ± 16.84 | 51.17 ± 17.2 | 51.45 ± 16.99 | 50.65 ± 16.97 | 2.44 | .12 |
|
| 24.75 ± 5.28 | 25.08 ± 5.08 | 25.45 ± 5.43 | 24.51 ± 5.36 | 1.32 | .31 |
|
| 44.65 ± 11.6 | 44.98 ± 12.12 | 45.38 ± 12.03 | 45.49 ± 11.5 | 1.71 | .22 |
|
| ||||||
|
| 47.31 ± 17.78 | 47.17 ± 17.06 | 47.09 ± 16.47 | 46.83 ± 18.17 | 0.32 | .81 |
|
| 29.50 ± 5.07 | 28.81 ± 7.21 | 31.70 ± 4.10 | 29.27 ± 7.21 | 1.05 | .38 |
|
| 46.73 ± 13.37 | 47.62 ± 12.98 | 47.20 ± 12.77 | 47.43 ± 13.56 | 0.60 | .62 |
|
| ||||||
|
| 49.38 ± 18.59 | 50.76 ± 17.78 | 49.46 ± 19.58 | 49.45 ± 18.15 | 1.58 | .25 |
|
| 43.52 ± 14.24 | 43.96 ± 14.32 | 44.21 ± 14.09 | 43.9 ± 13.68 | 0.87 | .48 |
|
| 61.41 ± 20.16 | 61.98 ± 20.10 | 61.63 ± 19.75 | 61.35 ± 19.83 | 1.08 | .39 |
- —Sichuan Provincial Natural Science Foundation of China
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsOrgan Transplantation Techniques and Outcomes · Liver physiology and pathology · Liver Disease Diagnosis and Treatment
Introduction
Hepatitis B virus (HBV) infection is one of the common infectious diseases in the world. In 2019, it was estimated that 296 million people were infected with HBV worldwide and nearly 1 million died.^1^ Liver cirrhosis (LC) is characterized with the degeneration and necrosis of hepatocytes, the formation of false lobules and regenerative nodules, and loss of liver function.^2^ LC is one of the major serious complications of HBV,^3^ with an estimated 331 000 people died from HBV-related cirrhosis in 2019.^4^ In addition, LC is also one of the main risk factors to develop liver cancer.^5^ The formation of reactive oxygen species is currently considered to be a major driver of LC,^6^ but the antioxidant therapy has limited effect.^5^ In fact, there is currently no effective drugs to prevent the progression of LC, which brought serious economic and medical burdens to society.
Although there are no drugs that can effectively treat LC, liver transplantation is the only way to treat end-stage liver disease. However, the practical problem is that it is difficult to get suitable donors. Moreover, among adult patients of LC, the mortality rate waiting for a liver transplant is close to 11%.^7^ Thus, it is urgent to find a new treatment to prevent LC from progressing.
Immune dysfunction is another major driver of LC, and regulating immune dysfunction is consider to be an effective way to prevent the progression of LC.^8^ Mesenchymal stem cells (MSCs) are a group of self-renewing cells capable of differentiating into a variety of cell types and playing a vital role in tissue healing and regeneration of damaged tissues.^9^ Due to the low immunogenicity^10^ and the ability to regulate the function of immune cells of MSCs,^11,12^ some studies showed that the autologous and allogeneic MSCs play a vital role in alleviating fibrosis and improving liver function.^13-16^ Thus, treatment for liver fibrosis by MSCs is safe, effective, and has a good research prospect.
Moreover, it is worth exploring how to transplant MSCs to the cirrhotic liver. The common administration of intrahepatic transplantation for MSCs include intravenous hepatic injection, arterial hepatic injection, and peripheral intravenous injection.^17^ The study of Barbash IM et al^18^ showed that the administration for MSCs transplantation via peripheral veins mainly accumulate in the lungs, while the liver, heart, and spleen are less distributed in the rat model of myocardial infarction. In addition, transplantation of MSCs via the hepatic artery usually requires X-ray guidance, but this method has a higher risk of radiation and bleeding. In contrast, the ultrasound-guided MSCs transplantation via the portal vein is more safe. In addition, the portal vein supplies 70%-80% of blood to liver, and the administration of MSCs via the portal vein can be accurately positioned and directly reach the liver blood sinuses. More importantly, multiple studies have shown that the MSCs transplantation via the portal vein is benefit over peripheral intravenous injection and can prevent the progression of LC.^19-21^ Thus, we should firstly choose portal vein for MSCs transplantation to LC.
However, the liver tissue of LC presents with diffuse fibrosis and the formation of regenerative nodules, resulting in rough surface of liver, increased hardness of liver parenchyma, and the disorders of intrahepatic vascular structure (such as portal vein spongiosis).^2^ In addition, the accumulation of inflammatory cells and matrix deposition around the portal vein lead to a thickening of Glission sheath.^22^ These pathological changes require us to select a more suitable catheter for MSCs transplantation. If a simple pig-tail catheter or central venous catheter is used, the portal vein cannot be successfully inserted from the rigid liver parenchyma and thickened Glission sheath by the guide wire due to the low rigidity of the hose material.^23^ Therefore, we need to select a suitable catheter for MSCs transplantation.
It is also important to evaluate the effects of MSCs transplantation in the treatment of LC, but there is lack of a comprehensive evaluation system for it. In recent years, the Two-dimensional shear-wave elastography ultrasound (TSWE)^24-26^ and contrast-enhanced ultrasound (CEU)^27-29^ have been used to effectively evaluate liver fibrosis. In addition, pathological changes play a vital important role in the evaluation of MSCs transplantation for the treatment of LC. Therefore, other than the traditional indicators related to liver fibrosis, the TSWE, CEU and the pathological changes were also comprehensively used to evaluate MSCs transplantation in the treatment of LC.
Above all, our study used a “retentional metal stiffner trocar” of pig-tail catheter for MSCs transplantation via portal vein to evaluate the safety and efficacy of this improved method in patients with LC and evaluate the effect of MSCs transplantation by a relatively comprehensive evaluation system.
Methods
Patients enrolled in the study
Fifteen patients with end-stage cirrhosis of hepatitis B at SiChuan Provincial People’s Hospital in China were enrolled in the study from November 2021 to December 2022. The clinical baseline data and the flow chart of this study are shown in supplemental material. Thirteen of the 15 patients were male and 2 were female. The mean age of them was 47.73 ± 7.08 years, the mean course of disease was 20.33 ± 9.75 years, the mean BMI was 23.79 ± 2.57 kg/m^2^, and the Child-Pugh grade of pathology was grade B in all of them. Among the 15 patients, HBV DNA quantification was 2.06 × 10^5^ IU/mL in 1 patient, and it was <1 × 10^3^ IU/mL in the other patients. In addition, all patients have received antiviral therapy.
Ethical approval
All patients have signed the informed consent forms and received approval from the institute’s Committee on Human Research of SiChuan Provincial People’s Hospital (2019001). This study is registered with Chictr.org.cn, number ChiCTR2100052843.
Inclusion and exclusion criteria
Inclusion criteria for LC patients were as follow:
(1) The age of men and/or women between 20 and 65; all patients had a definite diagnosis of chronic hepatitis B, and their HBV DNA measurement was outside the normal range prior to receiving anti-HBV drugs.(2) All patients with decompensated cirrhosis of chronic hepatitis B was diagnosed with a disease course of more than 5 years;(3) Criteria for decompensation of chronic hepatitis B cirrhosis: Child-Pugh grade B or Child-Pugh grade C, with reduced serum ALB, or more than 2-fold increase in bilirubin levels, or mild coagulation abnormalities, and no abdominal fluid accumulation or controlled abdominal fluid accumulation. Portal hypertension (moderate to severe lower esophageal fundus varicose veins, the number of platelet less than 1 × 10^5^/DL);(4) Orthotopic liver transplantation is not clinically suitable, or there is no clear liver source;(5) No severe bleeding tendency or active bleeding;(6) There was no hepatic encephalopathy in clinical assessment;
Exclusion criteria for LC patients were as follow:
(1) Age < 20 years or > 65 years;(2) Other causes of cirrhosis include alcoholic hepatitis, viral hepatitis C, and autoimmune hepatitis;(3) Patients with liver malignancy and/or family history of liver malignancy in three immediate family members;(4) The patient had a history of tumors in other organs;(5) Prothrombin time is extended by more than 3 seconds;(6) Human ALB was transfused within 3 weeks before enrollment;(7) Clinically significant upper gastrointestinal hemorrhage occurred within the first 4 weeks of enrollment;(8) The patient had spontaneous peritonitis;(9) An active infection caused by a virus or bacteria;(10) Pregnant or lactating women;(11) Hypersensitivity to ultrasound contrast media, inability to cooperate with breathing, BMI≥30kg/m^2^;
Evaluation of indicators related to liver fibrosis
The indicators of liver function, coagulation function and liver fibrosis in serum were analyzed by automatic biochemical analyzer.
Color Doppler ultrasound examination
The cannon aplio i800 color Doppler diagnostic instrument was used in our study. The ultrasound probe was placed in the right intercostal scan, and the first hepatic portal and main portal vein were fully displayed. The distance between the inner wall of the portal vein and the blood flow spectrum of the portal vein were measured at the widest point in front of the inferior vena cava and perpendicular to the tube wall. The Angle between the sampling line and the blood flow was ≤60°, and the color sampling frame was taken to an appropriate size and the sampling volume was set to 2 mm. When the blood flow signal in the main portal vein was well filled, the patient was asked to temporarily hold his breath, and the portal vein blood flow spectrum was measured at the same time. The sampling position was fixed as much as possible during each measurement of the portal vein blood spectrum in the same patient, and the measurement was repeated three times each time, and the final result was averaged.
Contrast-enhanced ultrasound
The cannon aplio i800 color Doppler diagnostic instrument was used with a convex array probe, the probe frequency range was about 3.5-5.0MHz, the mechanical index was set to 0.08, and the injection sulfur hexafluoride microbubble from Bracco Italy was used as the ultrasonic contrast agent.
Preparation method of contrast agent
The white dry powder of sulfur hexafluoride was dissolved with 5 mL 0.9% sodium chloride injection before use and shaken to make milky white suspension for reserve use. The ROI of tracking sampling during the imaging process was Ellipse 2D (Boundary BOX: 2.78 mm × 2.78 mm).
Two-dimensional shear wave elastic ultrasound
As recommended by the guidelines,^30^ S5 or S6 segments of liver should be selected as far as possible each time. When the 2D B-mode image is clearly displayed, the sampling frame should be appropriately enlarged. The sampling frame should be placed in the center of the entire image, and its upper edge should be placed 1-2 cm below the liver capsule, with a maximum depth of no more than 5 cm, and interference from non-target structures such as large blood vessels and gallbladder in the liver should be avoided. The patient was require to breathe gently for 3-5s, freeze the elastic image after it reaches uniform stability, and measure the liver elasticity value, and the measurement ROI is fixed at 10 mm.
Ultrasound-guided liver biopsy
After general anesthesia, the patient was positioned under ultrasound guidance and percutaneous liver biopsy was performed using Coaxial achieve 16GX15cm tissue biopsy needle. Three pieces of liver tissue were taken and fixed in 10% neutral formalin buffer. Slices were made according to standard methods. HE staining and Masson staining were performed, and inflammation and fibrosis stages were scored according to Ishak grading and staging system.^31^
MSCs transplantation
Material
16-G needle, 0.035-inch guide wire and “retentional metal stiffner trocar” of pig-tail catheter (7FR × 30 cm). Human umbilical cord mesenchymal stem cell were obtained from Shanghai Quansheng Biotechnology Co., Ltd (QSC1012021070601-2).
After the liver biopsy was successful, percutaneous portal vein puncture catheter (“retentional metal stiffner trocar” of pig-tail catheter of “Bonte” brand) was performed immediately under ultrasound guidance(as shown in Fig. 1A-D), and human umbilical cord mesenchymal stem cell injection (1 × 10^7^/mL, 10 mL/bag) was transfused after successful catheterization, and the process of infusion was not less than 30 minutes.
Ultrasound-mediated catheterization of the portal vein. (A) The 16G needle was inserted via the liver into the branch of the left lower external of the portal vein. The white arrow indicates that the tip of the needle is located on the left lower external of the portal vein; (B) The 0.035 inch guide wire was inserted along the needle core. The white arrow indicates the path of guide wire placement; (C) the “retentional metal stiffner trocar” of pig-tail catheter breaks through the capsule and parenchyma of liver into the portal vein. The white arrow indicates the “retentional metal stiffner trocar” of pig-tail catheter; (D) the Sonovue was injected by a drainage tube. Contrast-enhanced ultrasound showed that the contrast agent distributed diffusely into the hepatic parenchyma along the portal vein of the liver.
Safety monitoring
Subjects were followed in the hospital for immediate adverse events related with cell infusion (eg, anaphylactic reaction, fever, and bleeding) for 24 hours.
Follow-up
Liver biopsy was performed before and 24 weeks after MSCs transplantation, and Ishak grading and staging were performed according to pathological changes.
The following data were recorded for patients before and after MSCs transplantation in weeks 4, 12, and 24.
(1) Portal main internal diameter and portal blood flow velocity;(2) Liver Young’s modulus based on 2-dimensional shear wave elastic imaging measurement;(3) The following quantitative parameters of CEUS for portal vein, hepatic parenchyma and hepatic vein: peak intensity, peak time and mean transit time;(4) The levels of alanine aminotransferase, aspartate aminotransferase, albumin, and total bilirubin;(5) The indexes of serological fiber: hyaluronic acid, N-terminal peptide of type III procollagen, laminin and type IV collagen;(6) Coagulation function: prothrombin time(PT), prothrombin activity, activated partial thromboplastin time, and plasma fibrinogen;
Statistical analysis
Statistical software SPSS26 was used for data analysis, and all the collected data were tested for normality. The data conforming to normal distribution were represented by mean ± standard deviation, and the rank data were represented by median and interquart (25% and 75%). The comparison of data at different time points was performed by one-way repeated measurement ANOVA. If P < .05, the comparison before and after treatment was performed. Wilcoxon labeled rank sum test was used to compare the changes in Ishak grading and staging scores of patients before and after stem cell transplantation. P < 0.05 was considered statistically significant.
Result
The “retentional metal stiffner trocar” of pig-tail catheter was successfully used to MSCs transplantation for LC
All 15 patients were successfully infused with MSCs via the portal vein with “retentional metal stiffner trocar” pig-tail catheter under the guidance of CEU (Fig. 1). Moreover, the drainage tube did not escape with respiration within 30 minutes after the successful insertion of MSCs without any external interference (such as abdominal band pressure). A small amount of perihepatic bleeding occurred in 1 patient (6.67%) during the operation. Pleural effusion developed in 2 patients (13.33%) and abdominal effusion was increased in 3 patients (20.00%) within 3 days after surgery. The other 9 patients did not have any other complications. In addition, all patients were followed up to week 24, and none was lost or died. These data indicated that the improved “retentional metal stiffner trocar” of pig-tail catheter was effective and safe in the MSCs transplantation.
MSCs transplantation can alleviate some adverse changes associated with LC
As shown in Table 1, the levels of ALT, AST, TIBL, and ALB did not change significantly before and after MSCs transplantation. In the function of blood clotting, PT was lower than before with the treatment of MSCs transplantation. Also, we examined the indicators of liver fibrosis, including HA, LN, IV-C, and PCIIINP, and the results showed that the levels of HA and IV-C were significantly reduced after MSCs transplantation. To be specific, among the clinical indicators, PT, HA, and IV-C were statistically significant before and after transplantation. PT was decreased in 12 of 15 patients, HA was decreased in 13 patients, and IV-C was decreased in 9 patients before and 24 weeks after transplantation.
Moreover, Young’s modulus was detected by TSWE, which was one of the indicators related to tissue stiffness, and it was decreased after MSCs transplantation in LC (Table 2 and Fig. 2). In addition, Ishak grading and staging scores and liver biopsy were used to assess cell death, the data showed that the Lytic necrosis was decreased after MSCs transplantation (Table 3 and Fig. 3). The above data suggested that MSCs transplantation can alleviate the liver damage caused by LC.
The ultrasonic images of liver Young’s modulus detected by TSWE before and after MSCs transplantation. A–D represents the changes of Young’s modulus before and after transplantation. Abbreviations: Ave: the average of Young’s modulus value. SD: standard deviation.
Pathological changes of liver before and after MSCs transplantation. HE staining was performed after liver biopsy in the same patient before and after stem cell transplantation. The arrows indicate the inflammatory necrotic cells. By the Ishak scoring system, A and B scored 3 and 2 under 10× lens, respectively.
MSCs transplantation had no significant effect on liver hemodynamics detected by CEU in LC
To evaluate whether MSCs transplantation has an effect on liver hemodynamics, the hemodynamic measurements were measured by portal vein diameter, blood flow velocity, portal venography parameters, hepatic parenchymal contrast parameters, and hepatic venography parameters.
As we can see, the portal vein diameter was decreased after MSCs transplantation. However, other parameters showed no significantly change (Table 4). These data suggested that MSCs transplantation had no significant effect on liver hemodynamics detected by CEU at 24 weeks follow-up.
Discussion
Our study showed that MSCs transplantation can alleviate some adverse changes of LC, consistent with other studies,^32-34^ so it is worth to further research. MSCs transplantation via the portal vein is safe and effective, but due to the hardness and thickened Glission sheath of LC, and the traditional catheter is soft, it is difficult to implant MSCs into the liver. In order to overcome this difficulty, MSCs transplantation was performed by using the “retentional metal stiffner trocar” of pig-tail catheter in this study. The “retentional metal stiffner trocar” of pig-tail catheter preserves the hard casing of stainless steel, resulting in a higher hardness for the outer sheath hose of pig-tail, which can enter the portal vein via the hard liver tissue and thickened Glission sheath. Moreover, it has directional control when entering the tube. Our results showed that this improved method is safe and effective, and is worthy of further promotion in clinical practice.
However, it is lack of a more comprehensive evaluation system to evaluate whether MSCs transplantation is effective in the treatment of LC. Our results showed that MSCs transplantation improves some traditional indicators, such as coagulation function and serum markers of fibrosis. However, the liver function was not significant improved, consistent with other study.^35,36^ Oppositely, some studies showed that MSCs transplantation can improve liver function in patients with LC.^37,38^ These conflicting results suggested that more clinical studies are needed to confirm whether MSCs transplantation can improve liver function in LC.
In addition to those traditional indicators for evaluating LC, our study performed a relatively comprehensive evaluation for LC by TSWE, CEU, and pathological changes. TSWE has been widely used to evaluate liver fibrosis and has a good diagnostic accuracy for LC.^39^ In this study, we detected a decreased level in Young’s modulus by TSWE after MSCs transplantation, one of the indicators related to LC. On the other hand, the hemodynamic changes are one of the clinical features of LC.^40,41^ The increased portal vein diameter is a risk factor for portal vein thrombosis in LC patients.^42^ Our study showed that the portal vein diameter was decreased after MSCs transplantation, which suggested that MSCs transplantation may reduce the risk of portal vein thrombosis. However, other data showed that MSCs transplantation had no significant effect on other liver hemodynamics detected by CEU at 24 weeks follow-up. In addition, we also compared the changes of liver histopathology before and after MSCs transplantation. The pathology of LC patients confirmed that MSCs transplantation can improve inflammation and cell necrosis in liver tissue. Our results confirmed that MSCs transplantation can improve some clinical indicators in patients with LC, so it is worthwhile to further explore the molecular mechanisms.
Although the basic research was not performed in this study, with the increase of basic research on MSCs therapy for LC, the molecular mechanism of MSCs-based treatment is gradually understood. Hepatic stellate cell (HSC) activation is the main source of excessive accumulation of collagen and extracellular matrix (ECM), leading to the occurrence of LC.^43^ Therefore, inhibiting the activation of HSC is very important in inhibiting the progression of LC, and MSCs can inhibit the activation of HSC by regulating the inflammatory microenvironment.^44^ In addition, other mechanism of MSCs inhibits liver fibrosis is as follows^45^: (1) MSCs participate in liver tissue regeneration and repair by differentiating into hepatocytes or fusing with hepatocytes. (2) MSCs can produce a variety of cytokines and growth factors, which may enable the regeneration of endogenous cells in damaged tissues via their ability to exert paracrine effects. (3) MSCs participate in immunomodulatory effects in liver diseases by regulating a variety of immune cells, such as natural killer cells, B lymphocytes, and T lymphocytes. However, the anti-fibrotic effects of MSCs is due to the exogenous MSCs after transplantation, and the long-term fibrotic microenvironment in LC can change the characteristics and function of MSCs,^16^ so the therapeutic effect of MSCS may be weakened with the extension of time. Thus, on the basis of previous studies, we will continue to explore the molecular mechanism of MSCs in the inhibition of liver fibrosis in the following study.
In summary, we successfully implanted MSCs into the portal vein by using the improved “retentional metal stiffner trocar” of pig-tail catheter, and evaluated the efficacy of MSCs therapy by a relatively comprehensive evaluation system. The data showed that the improved method was effective and safe, and the results showed that MSCs transplantation can improve some adverse indicators related to LC. However, there are some shortcomings as follows: (1)The number of patients in our study is small; (2) the follow-up time is not long enough; (3) lack of in-depth molecular mechanism investigation. Based on the above shortcomings, we will increase the number of patients and extend the follow-up time in subsequent studies. In addition, we will study the molecular mechanism of MSCs transplantation in the treatment of LC on the follow-up research.
Conclusion
By a relatively comprehensive evaluation, MSCs transplantation can alleviate liver damage caused by LC. The improved “retentional metal stiffner trocar” of pig-tail catheter was effective and safe in the infusion of MSCs transplantation, which is worth promoting in the clinical practice.
Supplementary material
Supplementary material is available at Stem Cells Translational Medicine online.
szae081_suppl_Supplementary_Material
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Jeng WJ, Papatheodoridis GV, Lok A. Hepatitis B. Lancet. 2023;401:1039-1052.36774930 10.1016/S 0140-6736(22)01468-4 · doi ↗ · pubmed ↗
- 2Zhou WC, Zhang QB, Qiao L. Pathogenesis of liver cirrhosis. World J Gastroenterol. 2014;20:7312-7324.24966602 10.3748/wjg.v 20.i 23.7312 PMC 4064077 · doi ↗ · pubmed ↗
- 3Kramvis A, Chang K-M, Dandri M, et al. A roadmap for serum biomarkers for hepatitis B virus: current status and future outlook. Nat Rev Gastroenterol Hepatol. 2022;19:727-745. 10.1038/s 41575-022-00649-z 35859026 PMC 9298709 · doi ↗ · pubmed ↗
- 4Hsu YC, Huang DQ, Nguyen MH. Global burden of hepatitis B virus: current status, missed opportunities and a call for action. Nat Rev Gastroenterol Hepatol. 2023;20:524-537. 10.1038/s 41575-023-00760-937024566 · doi ↗ · pubmed ↗
- 5Parola M, Pinzani M. Liver fibrosis: pathophysiology, pathogenetic targets and clinical issues. Mol Aspects Med. 2019;65:37-55. 10.1016/j.mam.2018.09.00230213667 · doi ↗ · pubmed ↗
- 6Weiskirchen R. Hepatoprotective and anti-fibrotic agents: it’s time to take the next step. Front Pharmacol. 2015;6:303. 10.3389/fphar.2015.0030326779021 PMC 4703795 · doi ↗ · pubmed ↗
- 7Neuberger J. Liver transplantation in the United Kingdom. Liver Transpl. 2016;22:1129-1135. 10.1002/lt.2446227081833 · doi ↗ · pubmed ↗
- 8Albillos A, Lario M, Alvarez-Mon M. Cirrhosis-associated immune dysfunction: distinctive features and clinical relevance. J Hepatol. 2014;61:1385-1396. 10.1016/j.jhep.2014.08.01025135860 · doi ↗ · pubmed ↗