Ultrasound assessment and scoring of tendinopathy in hemophilia: Development of the Tendon Haemophilic Damage ‐ Ultrasound (THD‐US) method
Danilo Donati, Flavio Origlio, Stefano Galletti, Marco Miceli, Paolo Spinnato, Lelia Valdrè, Lydia Piscitelli, Vincenzo Ricci, Giuseppina Mariagrazia Farella, Fabio Vita, Roberto Tedeschi, Maria Grazia Benedetti

TL;DR
This study created a new ultrasound method to assess tendinopathy in people with hemophilia, helping improve diagnosis and treatment.
Contribution
The THD-US protocol is a novel ultrasound-based scoring system for evaluating hemophilia-related tendinopathy.
Findings
The THD-US method assessed 200 tendons in hemophilia patients, identifying structural changes, hyperemia, and calcifications.
The protocol offers a standardized and efficient way to evaluate tendinopathy in hemophilia patients.
The method can improve patient management and clinical outcomes for those with hemophilic arthropathy.
Abstract
This study aimed to develop and validate the tendinopathy hemophilia detection with ultrasonography (THD‐US) protocol for assessing hemophilia‐related tendinopathy. Twenty male patients with hemophilic arthropathy underwent ultrasound evaluations of 200 tendons. The THD‐US scoring method assessed structural changes, hyperemia, and calcifications, revealing various tendon abnormalities. This protocol provides a standardized, efficient method for assessing tendinopathy in hemophilia patients, potentially improving patient management and outcomes. This study introduces the THD‐US protocol, a novel ultrasound‐based scoring system for assessing tendinopathy in hemophilia patients. It effectively identifies and grades tendon abnormalities, facilitating better management and treatment strategies in clinical practice.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
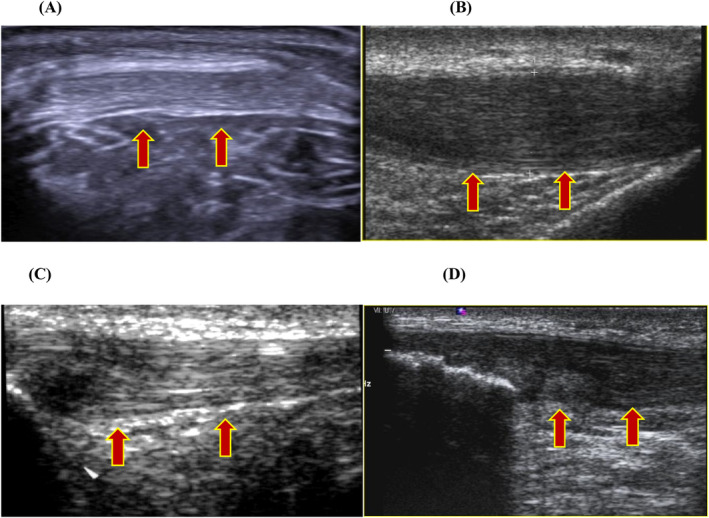 FIGURE 1
FIGURE 1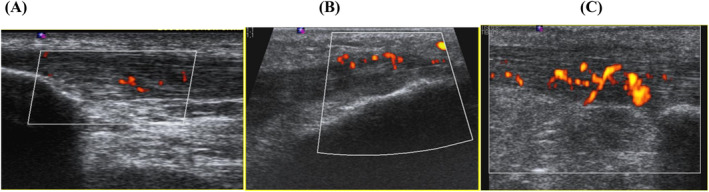 FIGURE 2
FIGURE 2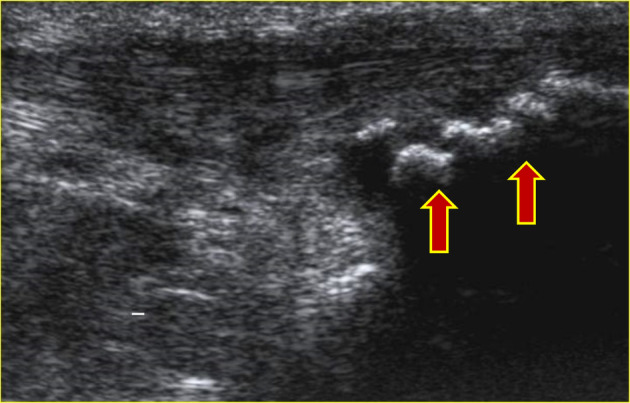 FIGURE 3
FIGURE 3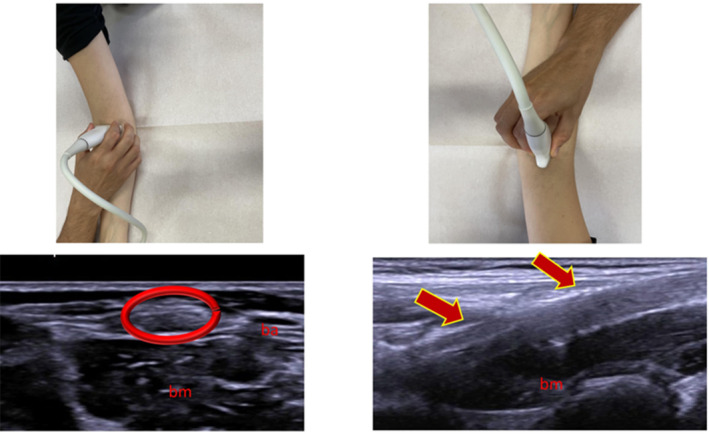 FIGURE 4
FIGURE 4| Echogenicity and eco‐structural alteration | Score |
|---|---|
| Grade 0 | 0 |
| Grade 1 | 1 |
| Grade 2 | 2 |
| Grade 3 | 3 |
| Signs of hyperemia on power‐color Doppler | |
| Grade 0—no new vessels visible | 0 |
| Grade 1—1–2 new vessels | 1 |
| Grade 2—few vessels/low blood flow | 2 |
| Grade 3—many vessels/significant blood flow | 3 |
| Tendon calcifications | |
| Absence of calcifications | 0 |
| Presence of calcifications | 1 |
| Tendon location | Echogenicity (0–3) | Hyperemia (0–3) | Calcifications (0–1) | Total THD‐US Score | Frequency |
|---|---|---|---|---|---|
| Biceps tendons | 0 | 0 | 0 | 0 | 20 |
| Triceps tendons | 3 | 3 | 1 | 7 | 1 |
| Triceps tendons | 3 | 1 | 1 | 5 | 1 |
| Quadriceps tendons | 1 | 0 | 1 | 2 | 1 |
| Patellar tendons | 0 | 1 | 1 | 2 | 1 |
| Achilles tendons | 1 | 1 | 1 | 3 | 1 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHemophilia Treatment and Research · Tendon Structure and Treatment · Blood Coagulation and Thrombosis Mechanisms
BACKGROUND
1
Hemophilia, characterized by recurrent bleeding episodes, manifests primarily as hemophilia A (factor VIII deficiency) and hemophilia B (factor IX deficiency), both transmitted through the X chromosome. Intra‐articular bleeding (hemarthrosis) commonly affects major joints like the elbow, knee, and ankle, leading to complications such as degenerative arthropathy.1, 2 Haemophilic arthropathy is a result of the development of recurrent hemarthrosis in the same target joint.3 Synovitis in HA, associated with iron deposition, leads to synovial inflammation and joint damage. Recurrent hemarthrosis triggers inflammatory responses within the joint, leading to acute and then chronic synovitis, which subsequently results in haemophilic arthropathy characterized by degenerative and destructive joint changes. Periarticular structures, including tendons and surrounding soft tissues, are often involved due to the chronic inflammatory environment created by recurrent hemarthrosis, leading to their degeneration and contributing to musculoskeletal limitations.1 Diagnostic imaging, particularly ultrasound, is crucial for assessing joint and tendon damage in hemophilia patients. This joint damage often extends to surrounding tendons, leading to tendinopathy, which is commonly observed in hemophilia patients.4 It is important to note that hemophilia‐induced tendinopathy significantly differs from mechanical tendinopathy caused by overuse, as it results from recurrent bleeding and inflammation, affecting tendon structure differently.5 This study aimed to develop the tendinopathy hemophilia detection with ultrasonography (THD‐US) protocol for assessing hemophilia‐related tendinopathy and to provide preliminary insights into its application.2, 6
METHODS
2
Participants with hemophilic arthropathy from the Center for Congenital Hemorrhagic Diseases. The study included male participants aged 18–65 years with ultrasound signs of hemophilic arthropathy. Exclusion criteria were elbow, knee, and ankle arthroplasty, or synovectomy. Ultrasound assessments targeted the biceps and triceps brachii tendons at the elbow, quadriceps and patellar tendons at the knee, and Achilles tendons at the ankle. A consensus between an experienced musculoskeletal radiologist and a specialist in physical medicine and rehabilitation (physiatrist) was maintained to ensure unbiased evaluation. The THD‐US protocol scoring method assessed structural changes in echogenicity, hyperemia on power‐color Doppler, and the presence of calcifications, with scores ranging from 0 to 7 (Table 1). The ultrasound examination was performed with a linear probe with musculoskeletal presets for elbow's tendons evaluation (7–16 MHz)7, 8, 9 (Figures 1, 2, 3, 4). The following scanning procedures were performed to assess the elbow, knee, and ankle:
- Elbow: For the distal biceps brachii tendon (DBBT), the elbow was fully extended and the hand supinated. The DBBT was observed laterally to the brachial artery and superficial to the brachialis muscle. For the distal triceps brachii tendon, the elbow was flexed at 90°, and the tendon was assessed using a sagittal scan.
- Knee: The quadriceps tendon was evaluated along a sagittal plane proximal to the patella with slight knee flexion to reduce anisotropy. The patellar tendon was observed inferiorly below the patella within a sagittal plane.
- Ankle: The patient assumed a prone position with the foot positioned outside the examination bed. The Achilles tendon was assessed using a posterior approach with the probe in a sagittal plane.
Echogenicity and eco‐structural alteration: (A) grade 0 normal tendon, (B) grade 1—mild ecostructure alteration, (C) grade 2—moderate ecostructure alteration, and (D) grade 3—severe ecostructure alteration and degeneration.
Signs of hyperemia on power‐color Doppler: (A) grade 1–1 to 2 new vessels, (B) grade 2—few vessels/low blood flow, and (C) grade 3—many vessels/considerable blood flow.
Presence of the insertional calcifications on the tendon.
Ultrasound image acquisition points and corresponding anatomical structures. Top row: Photographs showing the positioning of the ultrasound probe for scanning the distal biceps brachii tendon (left) and the distal triceps brachii tendon (right). Bottom row: Corresponding ultrasound images of the tendons. The left image (circled in red) shows the biceps brachii tendon (ba) and brachialis muscle (bm). The right image (indicated by arrows) shows the triceps brachii tendon (bm: Brachialis muscle).
RESULTS
3
Participants demographics and tendon evaluations
3.1
The study included 20 male participants with hemophilic arthropathy, consisting of varying severities of hemophilia A and B. The mean age of the participants was 40.6 years (SD ± 10.5). Each patient had 10 tendons assessed, resulting in a total evaluation of 200 tendons. Participants were included based on the presence of ultrasound‐detected joint damage, with a minimum score of 2 on the HEAD‐US score to ensure consistent assessment across varying age groups.
Biceps tendons
3.2
Upon ultrasound evaluation, the biceps tendons displayed no considerable echostructural alterations, hyperemia, or neovascularization on color Doppler imaging. Additionally, no intratendinous calcifications were detected in the biceps tendons, indicating that these tendons were relatively unaffected by hemophilic arthropathy in this cohort.
Triceps tendons
3.3
Notable alterations were observed in the triceps brachii tendons. Specifically, one patient exhibited grade‐three echostructural changes in the left triceps tendon, characterized by severe degeneration and eco‐structural alterations. Another patient showed grade‐three neovascularization in the right triceps tendon, indicating considerable blood flow changes associated with tendinopathy. Furthermore, one subject presented intratendinous calcifications in both triceps tendons, suggestive of advanced tendinopathic changes.
Quadriceps tendons
3.4
The quadriceps tendons demonstrated mild to moderate alterations. Grade‐one echostructural changes were observed bilaterally in one subject, indicating early stages of tendinopathy. However, there were no considerable changes in color Doppler signal, implying minimal vascular involvement. Bilateral insertional tendon calcifications were also noted in one patient, reflecting localized degenerative changes at the tendon‐bone interface.
Patellar tendons
3.5
In the patellar tendons, no considerable echostructural alterations were identified. However, one subject exhibited grade‐one neovascularization with color Doppler in the left patellar tendon, indicating mild vascular changes. Intratendon calcifications were present bilaterally in one subject, highlighting degenerative changes within the tendons.
Achilles tendons
3.6
The Achilles tendons presented with varying degrees of abnormalities. One subject showed grade‐one echostructural alterations in the right Achilles tendon, indicating early tendinopathic changes. Another subject exhibited grade‐one positive color Doppler signals in the right Achilles tendon, reflecting mild hyperemia. Bilateral insertional tendon calcifications were observed in one subject, suggesting localized degenerative processes at the Achilles tendon insertions.
THD‐US scores
3.7
The distribution of THD‐US scores across the evaluated tendons is summarized in Table 2. This table highlights the frequency of each score combination for echogenicity, hyperemia, and calcifications, providing a detailed overview of the tendinopathic changes observed in hemophilia patients.
The table presents the frequency distribution of THD‐US scores across various tendon locations (Biceps, Triceps, Quadriceps, Patellar, and Achilles) in hemophilia patients. The scores for echogenicity (0–3), hyperemia (0–3), and calcifications (0–1) are summed to obtain the total THD‐US score. The frequency column indicates the number of tendons with each specific scoring combination observed in the study.
Summary of findings
3.8
- Biceps tendons: No considerable echostructural alterations, hyperemia, neovascularization, or calcifications.
- Triceps tendons: Considerable findings included severe echostructural changes, neovascularization, and calcifications in specific cases.
- Quadriceps tendons: Mild echostructural changes and calcifications noted.
- Patellar tendons: Minimal neovascularization and bilateral calcifications observed.
- Achilles tendons: Mild echostructural alterations, hyperemia, and calcifications detected.
Implications
3.9
These findings underscore the variability in tendon involvement in hemophilic arthropathy, with certain tendons like the triceps and Achilles showing more pronounced changes compared to others such as the biceps. The THD‐US protocol demonstrated its utility in identifying and scoring tendinopathy severity, providing valuable insights for targeted patient management and treatment strategies.
The detailed results highlight the effectiveness of the THD‐US method in capturing subtle and considerable tendinopathic changes, thereby reinforcing its potential application in routine clinical practice for hemophilia participants.
DISCUSSION
4
This study highlights the potential of the THD‐US scoring system to standardize tendinopathy assessment in hemophilia participants. The THD‐US scanning protocols were designed to be accessible to non‐expert musculoskeletal sonographers, compatible with standard US machines, informative for joint status, reliable for monitoring treatment efficacy, and time‐efficient for clinical implementation. Future studies should explore the accuracy and effectiveness of the THD‐US score in longitudinal evaluations and its integration with other imaging modalities for comprehensive tendon assessment. The study provides considerable insights into tendon abnormalities in hemophilia participants. The THD‐US scoring method, which evaluates structural changes in echogenicity, hyperemia, and calcifications, offers a comprehensive assessment of tendinopathy. The absence of considerable changes in biceps tendons suggests varying susceptibility of different tendons to hemophilic arthropathy. The notable alterations in triceps, quadriceps, patellar, and Achilles tendons emphasize the importance of targeted ultrasound evaluations in these participants. This method aims to simplify examination and interpretation while ensuring strong intra‐ and inter‐reader reliability. The integration of THD‐US into routine hemophilia care could facilitate efficient evaluation and scoring of tendinopathy activity and damage, ultimately improving patient management and outcomes. Additionally, a comparison between ultrasound findings and clinically reported severity using validated outcomes, such as the TENDINS‐A, would provide further insights into the accuracy of the THD‐US protocol.10 Future studies should aim to validate these ultrasound findings against MRI to confirm their consistency.11
FUNDING INFORMATION
The authors received no fundings.
CONFLICT OF INTEREST STATEMENT
The authors declare no conflicts of interest.
ETHICS STATEMENT
Ethics Committee (PG n°. 0010368 del 17/06/2021), and all participants included signed the informed‐consent form to participate.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Roosendaal G , Lafeber FPJG . Blood‐induced joint damage in hemophilia. Semin Thromb Hemost. 2003;29:37‐42.10.1055/s-2003-3793812640563 · doi ↗ · pubmed ↗
- 2Dunn AL . Pathophysiology, diagnosis and prevention of arthropathy in patients with haemophilia. Haemophilia. 2011;17:571‐578.21342365 10.1111/j.1365-2516.2010.02472.x · doi ↗ · pubmed ↗
- 3Tedeschi R . Acquired haemophilia a in an elderly patient: a case report of functional recovery through physiotherapy. Int J Surg Case Rep. 2023;110:108769.37666165 10.1016/j.ijscr.2023.108769 PMC 10510055 · doi ↗ · pubmed ↗
- 4Poonnoose PM , Hilliard P , Doria AS , et al. Correlating clinical and radiological assessment of joints in haemophilia: results of a cross sectional study. Haemophilia. 2016;22:925‐933.27385495 10.1111/hae.13023 · doi ↗ · pubmed ↗
- 5Scott A , Squier K , Alfredson H , et al. ICON 2019: International Scientific Tendinopathy Symposium Consensus: Clinical Terminology. Br J Sports Med. 2020;54:260‐262.31399426 10.1136/bjsports-2019-100885 · doi ↗ · pubmed ↗
- 6Martinoli C , Della Casa Alberighi O , Di Minno G , et al. Development and definition of a simplified scanning procedure and scoring method for haemophilia early arthropathy detection with ultrasound (HEAD‐US). Thromb Haemost. 2013;109:1170‐1179.23571706 10.1160/TH 12-11-0874 · doi ↗ · pubmed ↗
- 7Donati D , Spinnato P , Valdrè L , et al. Ultrasound evaluation of tendinopathy in hemophiliac patients for the purpose of rehabilitation indications. J Clin Med. 2023;12:4513.37445548 10.3390/jcm 12134513 PMC 10342756 · doi ↗ · pubmed ↗
- 8Matthews W , Ellis R , Furness J , Hing WA . Classification of tendon matrix change using ultrasound imaging: a systematic review and meta‐analysis. Ultrasound Med Biol. 2018;44:2059‐2080.30007477 10.1016/j.ultrasmedbio.2018.05.022 · doi ↗ · pubmed ↗