Assessing the Knowledge, Attitude, and Practice of Healthcare Workers on the Herpes Zoster Vaccine in Saudi Arabia: A Cross-Sectional Study
Nouran M Moustafa, Norah F Alsaif, Esra Alsaeed, Alreem Alanezi, Amani Algarni, Lian Alkathery, Rania Mohamed

TL;DR
This study examines healthcare workers' knowledge and attitudes about the shingles vaccine in Saudi Arabia, finding gaps in understanding and recommending it, especially for immunocompromised patients.
Contribution
The study identifies specific knowledge gaps and barriers among Saudi healthcare workers regarding the recombinant zoster vaccine and proposes targeted strategies to improve vaccine uptake.
Findings
Most healthcare workers correctly identified the RZV vaccine doses, but many incorrectly believed side effects from the first dose were a reason to skip the second.
Many HCWs recommended the vaccine for healthy adults aged 18-49, outside of ACIP guidelines.
Patient concerns about risk and side effects, along with limited vaccine availability, were major barriers to vaccine recommendation.
Abstract
Background and objectives: Herpes zoster (HZ), known as shingles disease, has several complications that greatly affect elderly and immunocompromised people. Despite evidence for HZ vaccine efficiency and cost-effectiveness, the uptake of the HZ vaccine is lower than that of other common adult vaccines. Strong recommendations by healthcare workers (HCWs) for the HZ vaccine could increase vaccine uptake. Aim: This study aimed to investigate HCWs' knowledge, attitude, and practice of the recombinant zoster vaccine (RZV) in Saudi Arabia and identify gaps and barriers in vaccine recommendation. Materials and methods: A cross-sectional, questionnaire-based study was conducted in different hospitals in Riyadh, Saudi Arabia, between December 2023 and March 2024. An electronic self-administered validated questionnaire that assesses the knowledge, attitude, and practice of HCWs regarding the…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
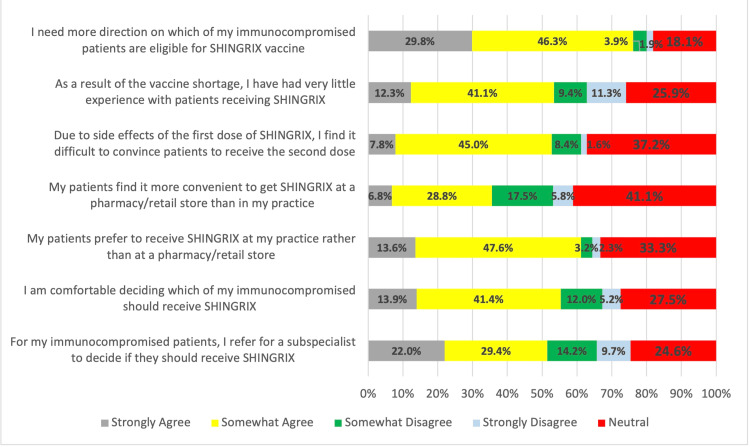 Figure 1
Figure 1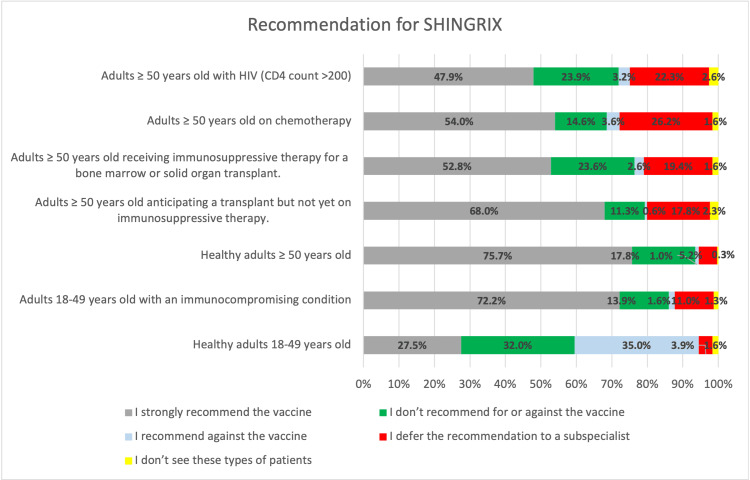 Figure 2
Figure 2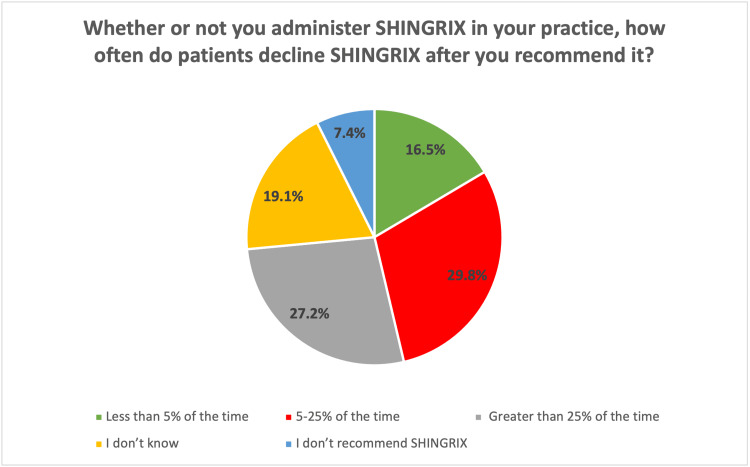 Figure 3
Figure 3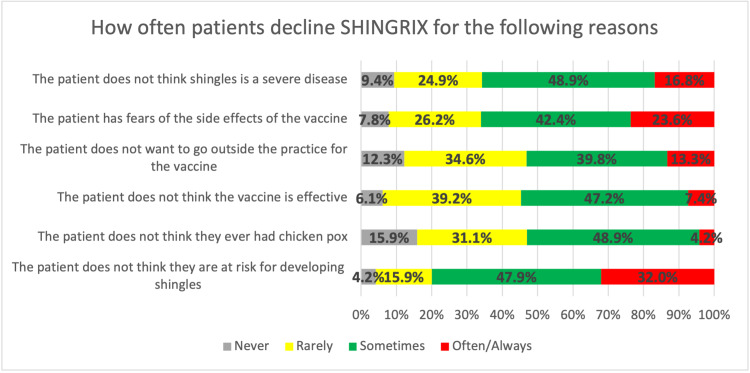 Figure 4
Figure 4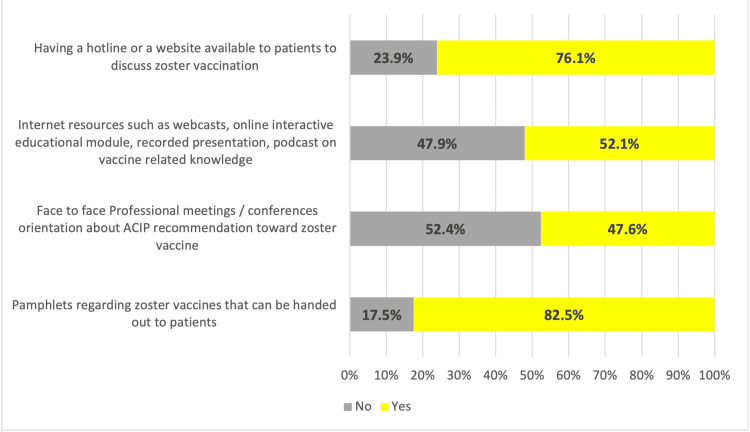 Figure 5
Figure 5| No. | % | |
| Sex | ||
| Male | 157 | 50.8 |
| Female | 152 | 49.2 |
| Age | ||
| 25-34 y | 125 | 40.5 |
| 35-44 y | 108 | 35.0 |
| 45-54 y | 57 | 18.4 |
| 55-65 y | 19 | 6.1 |
| Specialty | ||
| Family physician | 71 | 23.0 |
| Infectious disease | 63 | 20.4 |
| Dermatologist | 48 | 15.5 |
| Neurologist | 31 | 10.0 |
| General internist | 33 | 10.7 |
| Geriatrician | 22 | 7.1 |
| Oncologist | 17 | 5.5 |
| Nurse | 24 | 7.8 |
| level of expertise | ||
| General practitioner | 46 | 14.9 |
| Resident | 31 | 10.0 |
| Specialist | 51 | 16.5 |
| Fellow | 15 | 4.9 |
| Consultant | 166 | 53.7 |
| Experience years | ||
| 10 or fewer | 158 | 51.1 |
| 11–20 | 93 | 30.1 |
| 21–30 | 40 | 12.9 |
| >30 | 18 | 5.8 |
| Practice setting | ||
| Private hospital | 58 | 18.8 |
| Government hospital | 177 | 57.3 |
| Clinic | 26 | 8.4 |
| 1ry healthcare | 48 | 15.5 |
| No. of patients | ||
| 10 or fewer | 25 | 8.1 |
| 11-15 | 49 | 15.9 |
| 16-20 | 51 | 16.5 |
| 21-25 | 70 | 22.7 |
| >25 | 114 | 36.9 |
| Vaccine availability | ||
| No | 82 | 26.5 |
| Yes | 227 | 73.5 |
| Answer | Correct | Incorrect | Don’t know | ||||
| The two doses of RZV should be 2-6 months apart. | True | 267 | 86.4% | 27 | 8.7% | 15 | 4.9% |
| If the recommended interval between RZV doses is exceeded, then the series should be restarted. | False | 130 | 42.1% | 135 | 43.7% | 44 | 14.2% |
| A patient should get RZV, even if he/she has already had shingles. | True | 205 | 66.3% | 56 | 18.1% | 48 | 15.5% |
| Before administering RZV the provider must ensure a history of chickenpox or positive VZV serology. | False | 120 | 38.8% | 146 | 47.2% | 43 | 13.9% |
| If a patient experiences side effects from the first dose of RZV that prevents normal activities, then that person should not receive the second dose of RZV. | False | 94 | 30.4% | 148 | 47.9% | 67 | 21.7% |
| Specialty | Percentage of correct answers | ||
| 1: The two doses of SHINGRIX should be two to six months apart (correct answer: true). | |||
| Family physician | 52 | 73.2% | |
| Infectious disease | 60 | 95.2% | |
| Dermatologist | 39 | 81.3% | |
| Neurologist | 30 | 96.8% | |
| General internist | 26 | 78.8% | |
| Geriatrician | 21 | 95.5% | |
| Oncologist | 17 | 100.0% | |
| Nurse | 22 | 91.7% | |
| 2: If the recommended interval between SHINGRIX doses is exceeded, the series should be restarted (correct answer: false). | |||
| Family physician | 21 | 29.6% | |
| Infectious disease | 39 | 61.9% | |
| Dermatologist | 11 | 22.9% | |
| Neurologist | 17 | 54.8% | |
| General internist | 16 | 48.5% | |
| Geriatrician | 9 | 40.9% | |
| Oncologist | 7 | 41.2% | |
| Nurse | 10 | 41.7% | |
| 3: A patient should get SHINGRIX, even if he/she has already had shingles (correct answer: true). | |||
| Family physician | 40 | 56.3% | |
| Infectious disease | 52 | 82.5% | |
| Dermatologist | 28 | 58.3% | |
| Neurologist | 24 | 77.4% | |
| General internist | 21 | 63.6% | |
| Geriatrician | 15 | 68.2% | |
| Oncologist | 14 | 82.4% | |
| Nurse | 11 | 45.8% | |
| 4: Before administering SHINGRIX, the provider ensures a history of chickenpox or positive serology (correct answer: false). | |||
| Family physician | 27 | 38.0% | |
| Infectious disease | 38 | 60.3% | |
| Dermatologist | 12 | 25.0% | |
| Neurologist | 14 | 45.2% | |
| General internist | 13 | 39.4% | |
| Geriatrician | 4 | 18.2% | |
| Oncologist | 5 | 29.4% | |
| Nurse | 7 | 29.2% | |
| 5: If a patient experiences side effects from the first dose of SHINGRIX that prevents normal activities, then that person should not receive the second dose of SHINGRIX (correct answer: false). | |||
| Family physician | 15 | 21.1% | |
| Infectious disease | 34 | 54.0% | |
| Dermatologist | 14 | 29.2% | |
| Neurologist | 10 | 32.3% | |
| General internist | 5 | 15.2% | |
| Geriatrician | 6 | 27.3% | |
| Oncologist | 3 | 17.6% | |
| Nurse | 7 | 29.2% | |
| Yes | No | |||
| We give patients an appointment to return and receive the second dose | 74 | 23.9% | 235 | 76.1% |
| We rely on the patient to remember to come back to receive the second dose | 142 | 46.0% | 167 | 54.0% |
| We conduct reminder/recall (mail, e-mail, phone or text, etc.) for patients to come back and receive the second dose | 118 | 38.2% | 191 | 61.8% |
| We refer them to the vaccine manufacturer for their reminder/recall system | 141 | 45.6% | 168 | 54.4% |
| Not a barrier | Minor barrier | Moderate barrier | Major barrier | |||||
| Limited supply of RZV | 60 | 19.4% | 95 | 30.7% | 123 | 39.8% | 31 | 10.0% |
| More pressing medical issues take priority, I often forget to discuss RZV with my patients | 48 | 15.5% | 155 | 50.2% | 94 | 30.4% | 12 | 3.9% |
| My concerns about safety of RZV | 104 | 33.7% | 117 | 37.9% | 79 | 25.6% | 9 | 2.9% |
| My concerns about side effects of RZV | 83 | 26.9% | 145 | 46.9% | 63 | 20.4% | 18 | 5.8% |
| The fact that two doses of RZV are required | 103 | 33.3% | 107 | 34.6% | 87 | 28.2% | 12 | 3.9% |
| RZV has not been studied enough in immunosuppressed patients | 109 | 35.3% | 100 | 32.4% | 79 | 25.6% | 21 | 6.8% |
| My patients having a severe reaction to the first dose of RZV | 85 | 27.5% | 91 | 29.4% | 82 | 26.5% | 51 | 16.5% |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHerpesvirus Infections and Treatments · Virology and Viral Diseases · Viral Infections and Vectors
Introduction
Herpes zoster (HZ) also known as shingles is a reactivated form of varicella-zoster virus (VZV) that causes chickenpox. It is characterized by contagious painful vesicular eruptions affecting specific dermatomes, commonly lumbar and thoracic, which last for seven to 10 days [1]. HZ occurs exclusively in elderly and immunocompromised people with a previous history of chickenpox [2]. Some chronic diseases are also related to increased incidence of HZ (e.g., chronic obstructive pulmonary disease, diabetes) [3]. HZ has several complications that greatly affect patients. One of its common complications is post-herpetic neuralgia (PHN), which is characterized by severe neuropathic pain lasting for a minimum of three months after the rash onset. HZ ophthalmicus and HZ encephalitis are other complications that could also happen, ruin social activity, and interfere with the quality of patient life [4,5]. The latest research included HZ as one of the top 10 most costly skin diseases that increase the healthcare burden [6].
HZ therapeutic options mainly target pain relief and reducing complications [7]. Nevertheless, antiviral treatments such as acyclovir and anti-inflammatory drugs are only effective in decreasing the severity and duration of acute disease and do not reliably affect PHN [8]. The effective treatment of these conditions is usually vague and difficult, which makes prevention more convincing [9]. Preventive strategies are developed and considered the most efficient way to protect the health of patients, especially the elderly [10]. To prevent HZ and its complications, the US approved two vaccine products, namely, zoster vaccine live (ZVL) and recombinant zoster vaccine (RZV) [11].
Zoster vaccine live, known as Zostavax, is a single-dose live attenuated vaccine that was available for the elderly in the US from 2006 to 2017, yet Zostavax was not recommended for immunocompromised cases [12]. RZV, known as the Shingrix vaccine, is a two-dose vaccine that was approved in 2017 and exhibited greater and longer-lasting efficacy (>90% vs. 53%) [13]. It was recommended for use in immunocompetent and immunocompromised people ≥50 years to prevent VZ reactivation and decrease the severity of relapse [14]. It was recognized as effective and safe in immunocompromised cases having HIV, hematologic malignancies, and solid tumors, after renal and hematopoietic cell transplant [15]. Recently, in July 2021, the Food and Drug Administration (FDA) expanded the use of RZV in immunocompromised adults aged 18 years and older [16]. In October 2021, the Advisory Committee on Immunization Practices (ACIP) recommended RZV for immunocompromised adults aged 19 years and older [17]. The Centers for Disease Control and Prevention (CDC) recommended that the RZV vaccine be administered in two doses two to six months apart, even with a previous infection of HZ or with the last intake of Zostavax. Moreover, it is not compulsory to screen either through the laboratory or verbally for a previous infection with varicella. Immunocompromised patients or those who will be in an immunocompromised state should receive the two doses at ≥19 years. Although the second dose is typically administered after two to six months of the first dose, it can be received one or two months after the first dose in those people [18].
Despite the advances in the management of HZ infection, it remains a global serious public health concern. An estimated one million cases occur annually in the US among elderly individuals with an approximate ratio of four cases per 1,000 [19]. HZ burden and risk could be reduced by increasing HZ vaccine uptake [20]. Despite evidence for HZ vaccine efficiency and cost-effectiveness, the uptake of the HZ vaccine is lower than that of other common adult vaccines [21]. Global immunization rates demonstrate a lag for the HZ vaccine compared to annual influenza and pneumococcal vaccines [22]. Strong recommendations by healthcare workers (HCWs) for the HZ vaccine could reduce the lag [23]. Several studies have discussed HCW barriers to enhancing vaccine uptake [24]. Incomplete awareness of current HZ recommendations could also be considered. To our knowledge, there is a gap in the studies that evaluated the HCWs' knowledge of RZV. Thus, our goal is to investigate HCWs' knowledge, attitude, and practice (KAP) on the HZ vaccine, focusing on those caring for elderly and immunocompromised people. We aim also to identify gaps and barriers in vaccine recommendation and find opportunities to increase HZ vaccine knowledge and uptake in Saudi Arabia.
Materials and methods
Study design
A quantitative, cross-sectional, questionnaire-based study was conducted among HCWs from different hospitals in Riyadh, Saudi Arabia, during the period between December 2023 and March 2024.
Study population and sample size
A self-administered electronic questionnaire was sent to the hospital's staff and the response was requested from those treating patients susceptible to HZ. Participants were notified that all responses would be anonymous to ensure the transparency of all data collected.
OpenEpi (version 3.0) is used for sample size calculation considering a 95% confidence interval (CI), an anticipated frequency of 79%, and design effects of one [25].
Data collection tool
The questionnaire was adopted from other validated questionnaires used in different published studies [15,26,27,28]. it was reviewed, modified to fit with HCWs in Saudi Arabia, and then validated through a pilot study. Ethical approval (IRP) was provided by Dar Al Uloom University (IRB No.: HP-01-R-134-DAU-COM-24-11).
The questionnaire consisted of six sections (see Appendix). The first section asked about HCWs' demographics and practice characteristics. The second section involved questions about HCWs' knowledge regarding the shingles vaccine. The third section included HCWs' attitudes regarding zoster vaccine delivery. The fourth section covered the practice of HCWs and their recommendation of zoster vaccine to certain groups of patients including immunocompromised cases based on ACIP recommendations. The fifth section asked about experience with patients refusing the zoster vaccine. The sixth section covered barriers to recommending vaccination and strategies to overcome these barriers.
Piloting
The questionnaire was piloted by 20 HCWs (their results were also included in the final analysis), to assess the questions’ clarity, readability, and validity. According to their feedback, the questionnaire was amended as some items were changed to be clearer and applicable to HCWs. The overall questionnaire stability was measured by calculating Cronbach's alpha, which was 0.763.
Statistical analysis
The collected data were organized and entered on an Excel sheet (Microsoft Corpo., USA) and statistically analyzed using IBM SPSS Statistics for Windows, Version 25.0 (released 2017, IBM Corp., Armonk, NY). Qualitative data were presented by number and percent.
The results were tabulated, grouped, and statistically analyzed using the Pearson chi-square test (χ²) to detect whether there is a significant association between different categorical variables, and when it was inappropriate, it was replaced by the Monte Carlo exact test. P-value was also used to indicate the level of significance (P ≤ 0.05: significant, and P < 0.001: highly significant).
Results
A total of 309 HCWs responded to the survey. They included n = 157 (50.8%) males and n = 152 (40.5%) females whose ages ranged from 25 to 65 years old. Most of the participants’ age (n = 233, 75.5%) ranges from 25 to 44 years. They belonged to different specialties, including family physicians (n = 71, 23.0%), infectious diseases (n = 63, 20.4%), dermatologists (n = 48, 15.5%), general internists (n = 33, 10.7%), neurologists (n = 31, 10.0%), geriatricians (n = 22, 7.1%), oncologists (n = 17, 5.5%), and nurses (n = 24, 7.8%). The respondents' HCWs were consultants (n = 166, 53.7%), specialists (n = 51, 16.5%), general practitioners (n = 46, 14.9%), residents (n = 31, 10.0%), and fellows (n = 15, 4.9%). Regarding their experiences, n = 158 (51.1%) of them have a maximum of 10 years’ experience, n = 93 (30.1%) have 11-20 years’ experience, n = 40 (12.9%) have 21-30 years’ experience, and n = 18 (5.8%) have more than 30 years of experience. Most of the respondents' healthcare were from governmental hospitals (n = 177, 57.3%), while n = 58 (18.8%) from private hospitals, n = 48 (15.5%) from 1ry healthcare facilities, and n = 26 (8.4%) from clinics. The vaccine was available in n = 227 (73.5%) of settings (Table 1).
HCWs' knowledge regarding RZV
Based on the HCWs' responses to various knowledge questions related to RZV, n = 267 (86.4%) know that the two doses of RZV should be two to six months apart, while n = 205 (66.3%) know that patients should get RZV, even if he/she has already had shingles. However, n = 148 (47.9%) thought that experiencing side effects from the first dose of RZV was a reason not to receive the second dose. Also, n = 146 (47.2%) thought that before administering RZV, the provider must ensure a history of chickenpox or positive VZV serology, and n = 67 (21.7%) do not know that even if a patient experiences side effects from the first dose of RZV, that person should receive the second dose of RZV (Table 2).
The relation between HCWs' knowledge and specialty is also addressed. Higher percentages of HCWs from all specialties truly answered the first and third statements, i.e., “the two doses of RZV should be two to six months apart” and “a patient should get RZV, even if he/she has already had shingles,” respectively. Around 50% and more of infectious disease doctors truly answered all the questions, indicating their higher knowledge regarding RZV than other specialties (Table 3).
HCWs' attitude regarding RZV
Regarding HCWs' attitudes regarding the zoster vaccine, most of them (n = 235, 76.1%) agreed that they need more direction on which immunocompromised patients are eligible for the RZV vaccine. Some had very little experience with patients receiving RZV due to vaccine shortage (n = 165, 53.4%), and some also referred to a subspecialist to decide if they should receive RZV (n = 159, 51.4%). Moreover, n = 189 (61.2%) agreed that their patients prefer to receive RZV at the practice rather than a pharmacy/retail store (Figure 1).
Healthcare workers' attitude toward zoster vaccine
HCWs' practices regarding RZV
HCWs' recommendations for RZV in various patient groups are presented. Most of the respondents follow ACIP recommendations for the vaccine. Among the respondents, n = 234 (75.7%) recommend the vaccine for healthy adults ≥50 years old, n = 223 (72.2%) recommend the vaccine for adults 18-49 years old with an immunocompromised condition, n = 210 (68%) recommend the vaccine for adults ≥50 years old anticipating a transplant but not yet on immunosuppressive therapy, n = 167 (54.0%) recommend the vaccine for adults ≥50 years old on chemotherapy, and n = 163 (52.8%) recommend the vaccine for adults ≥50 years old receiving immunosuppressive therapy for a bone marrow or solid organ transplant. However, n = 85 (27.5%) recommended the vaccine for healthy adults 18-49 years old (Figure 2).
Healthcare workers' practices regarding the zoster vaccine
The HCWs used different methods to bring patients back for their second dose. In particular, n = 142 (46%) rely on the patient to remember to come back to receive the second dose, n = 141 (45.6%) refer patients to the vaccine manufacturer for their reminder/recall system, n = 118 (38.2%) conduct a reminder/recall for patients to come back for the second dose, and n = 74 (23.9%) give patients an appointment to return and receive the second dose (Table 4).
HCWs' experience with patients declining RZV
Following the recommendation of zoster vaccine, n = 84 (27.2%) of HCWs reported that patients declined VZV >25% of the time, n = 92 (29.8%) reported that patients declined 5-25%, and n = 51 (16.5%) reported that patients declined 5% of the time after it is recommended (Figure 3).
Percentage of patients declining zoster vaccine following recommendation
Physicians reported that patients most frequently decline RZV as they do not think they are at risk for developing shingles (n = 99, 32% "often/always"; n = 148, 47.9% "sometimes"), fears of side effects (n = 73, 23.6% "often/always”; n = 131, 42.4% "sometimes”), and patients don’t think shingles is a severe disease (n = 52, 16.8% “often/always”, n = 151, 48.9% “sometimes”) (Figure 4).
Healthcare workers' experience with patients declining zoster vaccine
HCWs reported barriers to recommending RZV
The most commonly reported barriers to recommending RZV included patients having a severe reaction to the first dose (n = 51, 16.5% "major”; n = 82, 26.5% “moderate” barrier), the limited supply of RZV (n = 31, 10% “major"; n = 123, 39.8% “moderate” barrier), RZV has not been studied enough in immunosuppressed patients (n = 21, 6.8% “major”; n = 79, 25.6% “moderate” barrier), and more pressing medical issues taking precedence (n = 12, 3.9% “major”; n = 94, 30.4% “moderate” barrier) (Table 5).
HCWs' strategies to increase vaccine uptake
A total of 255 (82.5%) HCWs chose the pamphlets regarding zoster vaccines that can be handed out to patients; n = 235 (67.1%) recommend having a hotline or a website available to patients to discuss zoster vaccination; n = 161 (52.1%) recommend Internet resources such as webcasts, online interactive educational modules, recorded presentations, and podcasts on vaccines; and n = 147 (47.6%) chose face-to-face professional meetings and conferences orientation about ACIP recommendation toward zoster vaccine (Figure 5).
Strategies to increase uptake of zoster vaccine
Discussion
To our knowledge, this represents the first assessment of the physicians’ perspective of RZV in Saudi Arabia following ACIP recommendations for licensure in 2021. This questionnaire study was administered to 309 HCWs who care for people with a higher risk of HZ infection and complications to recognize HCWs' KAP on HZ vaccination.
The survey findings reveal a mixed level of knowledge and varied practices regarding HZ vaccination among HCWs. The HCWs exhibited a relatively high level of knowledge about key aspects of the RZV, although some gaps remain. A significant 86.4% of HCWs correctly identified that the two doses of RZV should be spaced two to six months apart, and 66.3% knew that individuals who have had shingles should still receive the vaccine. These findings are consistent with recommendations from ACIP, which state that the RZV vaccine schedule involves two doses given two to six months apart and that individuals who have previously had shingles should still be vaccinated to reduce the risk of recurrence. However, the study also highlights gaps in HCWs’ understanding. For instance, 47.9% of the respondents incorrectly believed that side effects from the first dose were a valid reason not to receive the second dose. This knowledge gap is concerning because it could result in patients failing to complete the two-dose regimen, which is essential for optimal protection against shingles. Leigh et al. found that vaccine hesitancy due to concerns about side effects is a common barrier to vaccine uptake, particularly when healthcare providers themselves are unsure about the safety or necessity of completing a full vaccination course [29]. This is also consistent with findings from the study done by Yawn et al., which noted reluctance among pulmonologists to continue vaccination when patients report side effects [27]. Another notable gap is the belief held by 47.2% of HCWs that a history of chickenpox or positive varicella-zoster virus (VZV) serology is required before administering RZV. This misconception could lead to unnecessary delays in vaccination or missed opportunities for protection. According to Lin KY et al., it is not mandatory to confirm prior infection with chickenpox or perform VZV serology before administering RZV, as the vaccine is recommended for all individuals aged 50 years and older, regardless of history of shingles or chickenpox [30]. This indicates a need for better education about vaccine indications and contraindications. Singer D et al. reported also a knowledge gap in staff regarding the zoster vaccine where only 43% of specialists correctly answered all vaccine-related questions [31]. On the contrary, physicians were generally knowledgeable about RZV in a study done by Hurley et al. [15].
The difference in knowledge between specialties is also an interesting finding. The study reports that infectious disease specialists exhibited higher knowledge about RZV than other HCWs. This aligns with the findings of Wie SH et al., who noted that specialists in infectious diseases or immunology were more likely to be well-versed in the latest vaccine guidelines and to encourage vaccination in their patient populations [32]. The primary care providers or general practitioners reported to have less frequent exposure to vaccine-specific guidelines, and additional training and resources should be provided to close these knowledge gaps [33].
HCWs’ attitude toward RZV, as reported in this study, revealed a mixed response. The majority (76.1%) agreed that they need more guidance on which immunocompromised patients are eligible for RZV, suggesting a need for clearer guidelines or additional training on vaccinating high-risk populations. Peterson et al. also found that HCWs often feel uncertain about vaccinating immunocompromised patients, particularly in light of concerns about vaccine safety and efficacy in these groups [34]. In Hurley et al., a similar finding emerged, with a majority of family physicians indicating a need for guidance on patient eligibility for RZV [15]. As immunocompromised patients are at higher risk of shingles, targeted education is crucial to ensure that HCWs feel confident in recommending and administering the vaccine to these individuals.
The finding that 53.4% of HCWs had limited experience with administering RZV due to vaccine shortage in the private sector is consistent with the ongoing challenges faced by the healthcare system in maintaining an adequate supply of vaccines in all healthcare sectors. Wiot et al. also noted that vaccine shortage can create frustration among healthcare providers, potentially leading to delays in vaccination and reduced uptake [35]. This issue underscores the importance of improving vaccine distribution systems to ensure timely access to vaccines, particularly for high-risk populations who are more susceptible to complications from shingles in all healthcare facilities.
Moreover, the fact that 51.4% of HCWs referred patients to a subspecialist for vaccination decisions also points to a reluctance to make independent decisions about RZV in some healthcare settings. This trend is supported by research from Lin et al., which found that many healthcare providers defer vaccination decisions to specialists due to perceived uncertainty or a lack of familiarity with complex vaccination guidelines [36]. This suggests a need for increased confidence-building among HCWs, particularly in general practice settings, to empower them to make vaccination recommendations on their own.
In addition, 61.2% of HCWs agreed that patients prefer to receive RZV in their primary care practice rather than at a pharmacy or retail store. This finding reflects patients’ desire for convenience and trusted healthcare provider involvement in vaccine administration, as supported by Ahmed et al.'s study [37]. Offering vaccines within the primary care setting ensures that patients receive trusted medical advice and are more likely to complete the vaccine series, which can improve overall vaccination rates.
The study reflects that most healthcare providers follow the ACIP recommendations for RZV across patient demographics. For instance, high percentages of healthcare providers recommend RZV for healthy adults over 50 (75.7%) and adults aged 18-49 with immunocompromising conditions (72.2%). This adherence is consistent with findings in the article of Hurley et al., which shows that a significant portion of primary care physicians already recommends RZV to immunocompromised individuals, particularly those ≥50 with conditions like HIV or on immune-modulating treatments [15]. According to a study done by Dooling KL et al., HCWs' recommendation practices often reflect guidelines provided by health authorities like the CDC and ACIP, which in turn influences the willingness of patients to accept the vaccine [38]. While adherence is strong, some differences arise in the recommendations for specific groups. For example, 27.5% of HCWs in this study recommended the vaccine for healthy adults 18-49 years old. Similarly, Singer et al. noted that while a majority recognize herpes zoster as a risk and value RZV, specialists’ knowledge about all ACIP indications is low [31].
Regarding the strategies for ensuring patients receive their second dose of RZV, the current study reports that many healthcare systems rely on patient self-reporting with minimal follow-up measures, which can be ineffective in ensuring adherence. George et al. highlighted that using a more structured follow-up system (such as setting an appointment for the second dose or providing direct reminders) improves completion rates for vaccines like RZV [39]. The relatively low use of appointment setting (23.9%) in the study is concerning and reflects broader trends in healthcare practice, where time and resource limitations can reduce the effectiveness of follow-up strategies.
The study shows that a substantial proportion of patients decline the RZV, due to perceived low risk of shingles, fears of side effects, or doubts about the severity of the disease, which is consistent with findings in other studies. For example, Wang et al. found that many patients overestimate their personal immunity or underestimate the risks of shingles, which leads to vaccine hesitancy [40]. They also highlighted that education about the potential complications of shingles, such as post-herpetic neuralgia, is often insufficient. This supports the finding of our study that many patients do not see shingles as a severe disease (16.8% “often/always,” 48.9% “sometimes”) and therefore do not prioritize vaccination. A similar opinion was noted by AlMuammar et al. where the top reasons for vaccine refusal were related to misconceptions about the risk of shingles, concerns over side effects, and a belief that the vaccine wasn’t necessary for healthy individuals [41]. Alamri et al. reported that perceived side effects, particularly pain or swelling at the injection site, were common deterrents among vaccine recipients [42]. The study by López-Fauqued M et al. further supports this, noting that while the safety profile of RZV is generally positive, concerns about side effects often fear the patients, leading to significant declines in vaccination offers [43].
The barriers that HCWs face in recommending RZV, particularly the concerns about patient reactions to the first dose, the limited vaccine availability, and the perception that RZV has not been adequately studied in immunocompromised patients, are well-documented in the literature. Peterson et al. found that adverse reactions following the first dose of RZV were a significant concern among healthcare providers, which may explain the hesitancy to recommend the vaccine to certain groups [34]. This aligns with the findings in the present study, where 16.5% of HCWs described adverse reactions to the first dose as a major barrier. However, it is important to note that while side effects are a legitimate concern, studies such as Parikh et al., have shown that the risk of severe reactions is relatively low, and most adverse events are mild and transient [44]. Limited vaccine availability is another barrier, with 10% of HCWs citing this as a “major” obstacle. This issue was also identified by Iwu-Jaja et al. who reported that vaccine shortages, particularly during peak vaccination seasons, can lead to delays in patient vaccinations and reduced overall uptake [45]. The authors suggested that improving the supply chain for vaccines, increasing inventory management, and ensuring timely distribution could help alleviate this issue. Regarding immunocompromised patients, the concerns expressed by HCWs (6.8% major, 25.6% moderate) about the adequacy of RZV studies in these populations are well-founded, as there has historically been limited data on the safety and efficacy of vaccines in immunocompromised individuals. Stefanizzi et al. noted that while RZV is recommended for immunocompromised patients, some HCWs remain hesitant due to a lack of long-term data on how the vaccine performs in these vulnerable groups [46]. However, more recent studies, including the one by Omari et al., have shown that RZV is safe and effective in immunocompromised patients, suggesting that this concern may gradually decrease with greater dissemination of updated evidence [47].
The strategies identified for increasing RZV uptake, such as providing educational pamphlets (82.5%), using hotlines or websites (67.1%), and offering online resources (52.1%), reflect a growing recognition of the importance of patient education and accessible information. A study by Almakhdob et al. found that educational outreach is one of the most effective methods for improving vaccine uptake, especially when combined with patient-centered communication strategies [48]. These findings align with the data provided in the study, where pamphlets and online resources were chosen as primary methods for promoting RZV.
The role of professional meetings and conferences in educating HCWs (47.6%) is also significant, as continuous professional development has been shown to improve vaccination recommendation rates. George et al. highlighted that face-to-face meetings and training sessions are particularly effective in ensuring that healthcare providers remain updated on the latest vaccine guidelines and best practices for patient communication [39].
Finally, AlMuammar et al. found that reminder and recall systems, including phone calls, text messages, and automated systems, significantly improved vaccination completion rates [41]. This supports the finding in our study that relying on patients to remember to return for their second dose was less effective compared to structured reminder systems. Integrating patient appointment scheduling with reminder systems may further enhance adherence rates.
While this survey study includes samples of HCWs in Saudi Arabia, certain limitations must be acknowledged. The findings are based on self-reported data rather than direct observation of actual practice or qualitative responses. In addition, physicians from smaller practices are slightly underrepresented. Moreover, our results do not clarify whether some physicians genuinely oppose vaccine use in immunocompromised patients or if they need more direction or prefer to defer the decision to a subspecialist.
Conclusions
Overall, HCWs demonstrated an understanding of the key recommendations for RZV, but still, there are areas, especially in vaccine indications and contraindications, where knowledge gaps exist. By addressing these gaps through targeted education and professional development, healthcare systems can increase confidence in recommending RZV. Moreover, fostering a positive attitude toward vaccination, particularly regarding immunocompromised patients and overcoming vaccine shortages, will be essential in achieving higher vaccination rates and reducing the incidence of shingles and its complications.
The main challenges toward vaccine uptake include patient misconceptions about the risk of shingles, concerns about side effects, and logistical barriers such as vaccine availability and inadequate follow-up systems. The strategies recommended by HCWs, including educational initiatives and digital resources, align with evidence-based practices that have been shown to improve vaccine uptake. By addressing these barriers and implementing comprehensive, multi-channel strategies for increasing HCWs' awareness, patient education, and follow-up, healthcare systems can increase RZV vaccination rates and reduce the burden of shingles, particularly in high-risk populations.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Evaluating physician attitudes and practices regarding herpes zoster vaccination Cornea Tsui E Gillespie C Perskin M Zabar S Wu M Cohen EJ 9479513720182957886510.1097/ICO.0000000000001582 · doi ↗ · pubmed ↗
- 2Varicella-Zoster virus infection: natural history, clinical manifestations, immunity and current and future vaccination strategies New Microbiol 2. Freer G Pistello M 95105412018 https://arpi.unipi.it/handle/11568/92728129498740 · pubmed ↗
- 3Comparison of varicella-zoster virus-specific immunity of patients with diabetes mellitus and healthy individuals J Infect Dis Okamoto S Hata A Sadaoka K Yamanishi K Mori Y 1606161020020091982171910.1086/644646 · doi ↗ · pubmed ↗
- 4Epidemiology, treatment and prevention of herpes zoster: a comprehensive review Indian J Dermatol Venereol Leprol Koshy E Mengting L Kumar H Jianbo W 2512628420182951690010.4103/ijdvl.IJDVL_1021_16 · doi ↗ · pubmed ↗
- 5Herpes zoster burden of illness and health care resource utilisation in the Australian population aged 50 years and older Vaccine Stein AN Britt H Harrison C Conway EL Cunningham A Macintyre CR 5205292720091902704810.1016/j.vaccine.2008.11.012 · doi ↗ · pubmed ↗
- 6The burden of skin disease in the United States J Am Acad Dermatol Lim HW Collins SA Resneck JS Jr 9589727620172825944110.1016/j.jaad.2016.12.043 · doi ↗ · pubmed ↗
- 7Management strategies for herpes zoster and postherpetic neuralgia J Am Osteopath Assoc Galluzzi KE 01072007 https://pubmed.ncbi.nlm.nih.gov/17488885/17488885 · pubmed ↗
- 8Herpes zoster and postherpetic neuralgia: prevention and management Am Fam Phys Fashner J Bell AL 14321437832011 https://www.aafp.org/pubs/afp/issues/2011/0615/p 1432.html 21671543 · pubmed ↗