Sentinel Node Biopsy in Laryngeal Cancer: A Systematic Review and Meta-Analysis
Pegah Sahafi, Ramin Sadeghi, Emran Askari, Azadeh Sahebkari, Mitra Ghahraman, Ehsan Khadivi, Kamran Khazaeni, Vahid Reza Dabbagh Kakhki, Sara Harsini

TL;DR
This study reviews and analyzes the effectiveness of sentinel node biopsy in laryngeal cancer, finding it reliable for staging, especially for supraglottic tumors.
Contribution
The paper provides a systematic review and meta-analysis of sentinel lymph node biopsy accuracy in laryngeal SCC, comparing tumor location and mapping materials.
Findings
SLN detection rate was 90.8% with a sensitivity of 88% in laryngeal SCC.
Supraglottic tumors showed higher detection rates (93.7%) and sensitivity (96%) compared to transglottic tumors.
Radiotracers outperformed blue dye in both detection rates and sensitivity.
Abstract
Background: Sentinel lymph node (SLN) biopsy offers a minimally invasive approach to staging lymph node involvement in laryngeal squamous cell carcinoma (SCC). Despite its adoption in other cancers, its accuracy in laryngeal SCC remains under investigation. This systematic review and meta-analysis evaluates the diagnostic performance of SLN mapping in laryngeal cancer. Methods: A systematic search of MEDLINE, Scopus, and Google Scholar was conducted using the keywords “(larynx OR laryngeal) AND sentinel”, with no date or language restrictions. Studies reporting SLN detection rates and/or sensitivity in laryngeal SCC were included. A random-effects model was applied for data pooling, and subgroup analyses were performed based on tumor location (supraglottic versus transglottic) and mapping material (radiotracer versus blue dye). Publication bias was assessed using funnel plots and…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
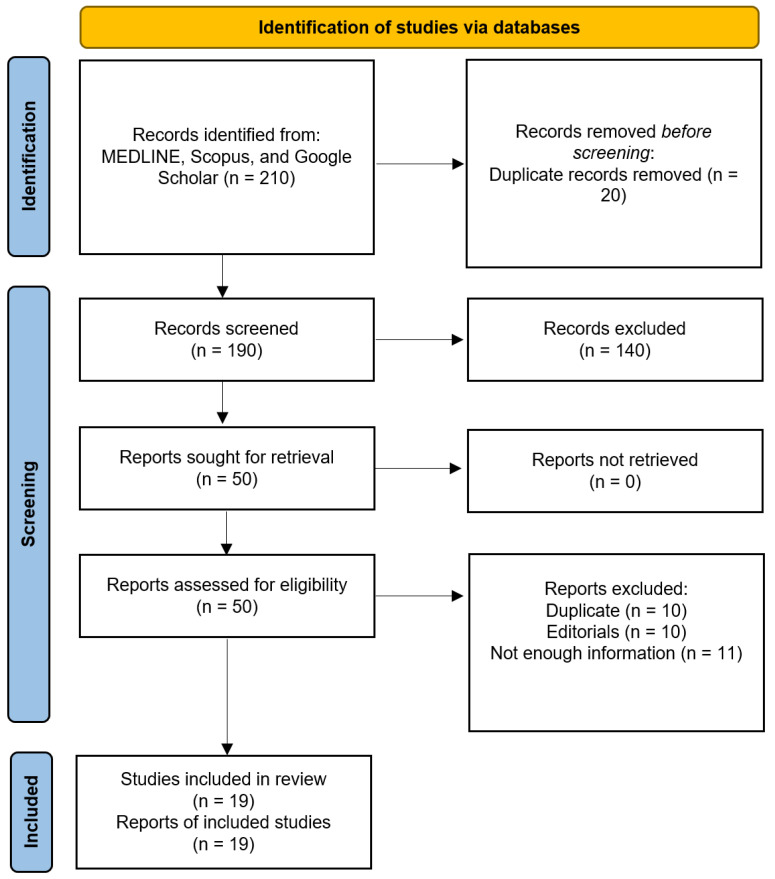 Figure 1
Figure 1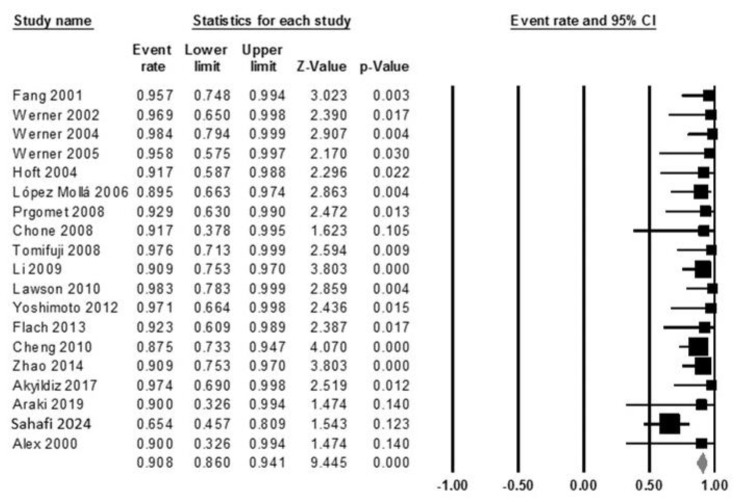 Figure 2
Figure 2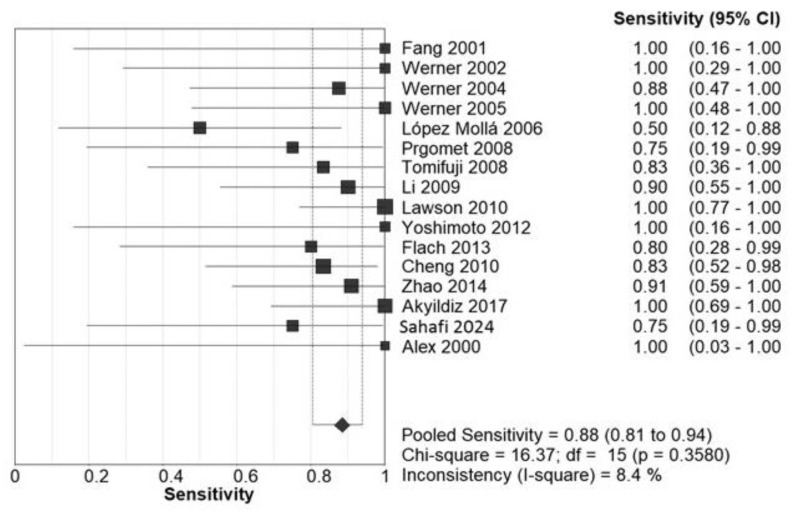 Figure 3
Figure 3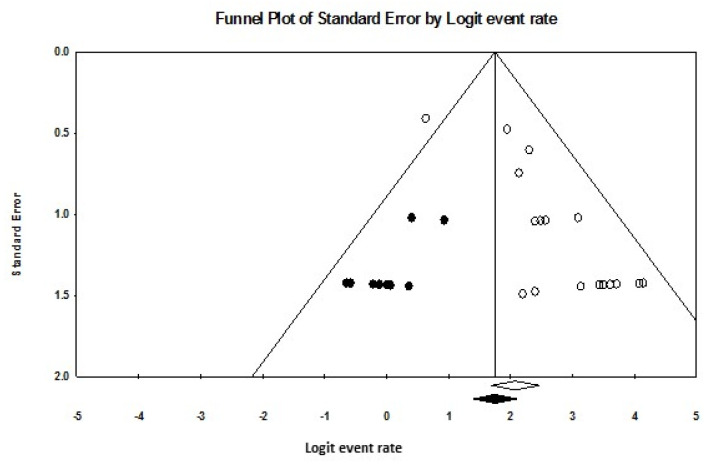 Figure 4
Figure 4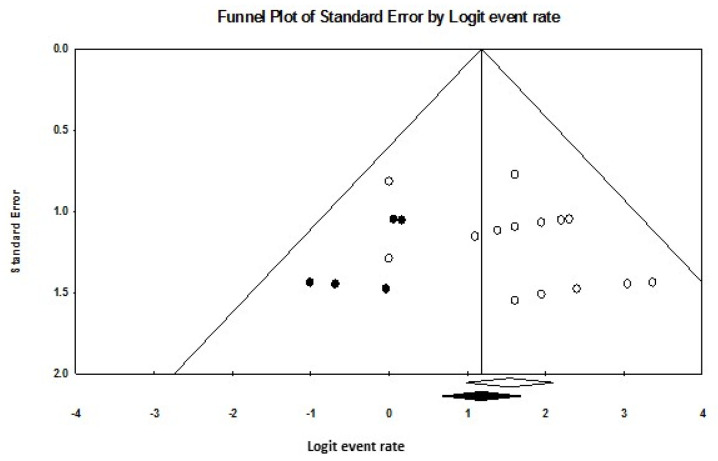 Figure 5
Figure 5Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHead and Neck Cancer Studies · Colorectal and Anal Carcinomas · Salivary Gland Tumors Diagnosis and Treatment
1. Introduction
Laryngeal cancer is among the most prevalent malignancies of the respiratory tract, with cervical lymph node metastases significantly influencing survival outcomes in laryngeal squamous cell carcinoma (SCC) [1,2,3]. About 50% of laryngeal cancer patients survive 7 years; survival varies by location, with glottic highest (84%) and supraglottic lowest [4,5]. Despite advances in imaging modalities, detecting metastatic lymph nodes remains a considerable challenge. Occult lymph node metastases are commonly observed in head and neck SCCs, particularly in supraglottic laryngeal carcinomas, due to the dense lymphatic network in this region [6]. While early-stage glottic tumors exhibit a low risk of cervical lymph node metastasis (0–10%), advanced-stage tumors have a higher incidence, ranging from 10% to 35% [7]. Lymph node metastases occur at a very low rate in T1–T2 stages and in well-differentiated tumors [8].
Managing the clinically node-negative (N0) neck in head and neck cancer has been a subject of debate for decades. Most treatment centers favor elective neck treatment—either through surgery or radiation—when the risk of occult metastases surpasses 15% to 20%. However, this approach may lead to overtreatment in a substantial proportion of patients [6,9]. In supraglottic and advanced T-stage glottic laryngeal SCC, where no lymph node involvement is evident upon examination and imaging, the standard procedure typically involves bilateral elective neck dissection (END) [10]. The prevalence of occult metastases is notably higher in supraglottic tumors (23%), exceeding that of glottic tumors by 10.8%. Furthermore, advanced T-stage tumors are significantly more likely to develop occult metastases compared to early T-stage tumors [9]. A systematic review revealed that even in low T-stage supraglottic tumors (T1–T2), the rate of occult lymph node metastases was 18.4% [1].
Advanced imaging techniques, such as fluorine-18 fluorodeoxyglucose positron emission tomography/computed tomography (F-18 FDG PET/CT), have demonstrated moderate specificity but limited sensitivity for detecting cervical lymph node metastases in clinically N0 head and neck SCC (HNSCC) patients [11]. Consequently, there remains a critical need for less invasive, yet reliable, approaches for staging regional lymph nodes in laryngeal carcinoma.
Sentinel lymph node mapping has emerged as a promising method for detecting lymph node metastases, with growing evidence supporting its utility in laryngeal carcinoma [6,12]. Sentinel lymph node biopsy (SLNB) operates on the principle that cancer metastasizes in a predictable pattern through the lymphatic system, initially involving sentinel lymph nodes (SLNs) before spreading to other nodes. Thus, SLN status serves as a reliable indicator of regional lymphatic involvement [13,14,15]. Accurate detection of metastases relies on advanced techniques such as step serial sectioning and immunohistochemistry [16].
Despite its potential, SLNB is not without limitations. For instance, PET/CT scans, while offering good specificity and positive predictive value, lack sufficient sensitivity and negative predictive value, making them unreliable for excluding neck dissection in salvage laryngectomy for recurrent laryngeal SCC [17]. Given these considerations, we conducted an extensive systematic review and meta-analysis to evaluate the accuracy and success of SLN biopsy in staging cervical lymph node involvement in laryngeal SCC. This analysis aims to provide robust evidence on the feasibility and clinical utility of this technique.
2. Materials and Methods
2.1. Search Strategy and Inclusion Criteria
The systematic review was conducted in accordance with the PRISMA protocol [18], structured around the following PICO framework: PICO Patient—patients with proven laryngeal cancer who are candidates for laryngectomy and lymph node dissection; Intervention—sentinel node biopsy; Comparison—cervical lymph node dissection; Outcome—false negative rate.
Comprehensive searches of Medline, Scopus, and Google Scholar were conducted using the keywords: (larynx OR laryngeal) AND sentinel. No restrictions on language or publication date were applied. Only studies focused on SLN mapping and biopsy in SCC of the larynx were included. To ensure thorough coverage, reference lists and citing articles of the retrieved studies were examined for additional relevant studies. The last search was completed in March 2024.
Eligibility criteria required that studies report sufficient data to extract the detection rate and/or false-negative rate of SLN mapping in laryngeal SCC. Database searches and study selection were conducted independently by two authors. Discrepancies between the two reviewers were resolved through consultation with a third author. In cases of duplicate studies, only the most recent or comprehensive publication was included.
2.2. Quality Assessment
The quality of the included studies was evaluated using the Oxford Center for Evidence-Based Medicine checklist for diagnostic studies [19]. This checklist assesses several key areas:
Patient recruitment: Prospective consecutive inclusion was considered the optimal recruitment method.
Reference standard: The preferred reference standard was radical neck dissection for all patients, regardless of SLNB pathology results. Alternatively, long-term follow-up of patients with pathologically negative sentinel nodes was acceptable as a gold standard. It was critical that the reference standard be applied blindly to SLNB results.
Spectrum of patients: An ideal patient spectrum included all clinically node-negative (cN0) laryngeal cancer patients.
2.3. Statistical Analysis
Meta-analyses of sensitivity and detection rate were performed using a random-effects model (Der-Simonian and Laird method) [20]. This approach accounts for variability between studies, making it particularly suitable for pooling data across studies with heterogeneous characteristics. Heterogeneity was assessed using the Cochrane Q test, with significance set at p < 0.05, and quantified using the I^2^ index, which measures variability attributable to true heterogeneity rather than sampling error [21].
Publication bias was evaluated using funnel plots, Egger’s regression intercept, and Duval–Tweedie’s trim and fill method [22,23]. Funnel plots display the standard errors of included studies on one axis and their effect sizes on the other. Funnel plot asymmetry suggests potential publication bias, which was quantified using Egger’s regression intercept (p < 0.05 indicating significant bias). Duval–Tweedie’s trim and fill method adjusts for bias by iteratively removing smaller studies to achieve symmetry in the funnel plot, yielding an adjusted pooled effect size to estimate the impact of publication bias.
Meta-analytical calculations were performed using Comprehensive Meta-Analysis (version 2) and Meta-DiSc (version 1.4) [24]. Key diagnostic indices, detection rate, and false-negative rate were defined as follows:
Detection rate: The proportion of patients in whom at least one SLN was successfully identified.
False-negative rate: The proportion of patients with pathologically involved non-sentinel nodes despite having pathologically negative SLNs.
Subgroup analyses were conducted to explore the impact of lymphatic mapping materials (blue dye versus radiotracer) and tumor anatomical location (supraglottic versus transglottic) on outcomes.
The sensitivity and false negative rate of the sentinel node biopsy were reported based on elective cervical lymph node dissection pathology reports. There was no follow up report or any prognostic data in the included studies.
3. Results
Figure 1 shows a summary of the search strategy and inclusion process of the study. Overall, 19 studies were included in the systematic review [12,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42]. Among these studies, 13 provided data for separate subgroups of supraglottic and transglottic tumors. Three studies did not report the tumor T-stages, while the remaining studies included patients across T1 to T4 stages, comprising 39 T1, 129 T2, 106 T3, and 39 T4 cases. Additionally, two patients had a history of recurrent disease. A detailed summary of the included studies is presented in Table 1.
3.1. Detection Rate
The pooled detection rate for SLNB was 90.8% (95% CI: 86–94.1), as shown in the forest plot in Figure 2. Heterogeneity analysis indicated a Cochrane Q value of 23.02 (p = 0.189) and an I^2^ index of 21.80%, suggesting low variability among studies.
Subgroup analysis demonstrated differences in detection rates based on the SLN mapping method and tumor location. For SLN mapping materials, studies employing blue dye injection reported a pooled detection rate of 81.5% (95% CI: 67.8–90.2), whereas those using radiotracer injection achieved a significantly higher pooled detection rate of 90.8% (95% CI: 85.5–94.3). Tumor location also influenced the detection rate, with transglottic tumors exhibiting a pooled detection rate of 84.7% (95% CI: 75.9–90.7) compared to supraglottic tumors, which had a pooled detection rate of 93.7% (95% CI: 88.9–96.5). The majority of sentinel nodes were localized in cervical levels II and III, although three studies did not report sentinel node locations.
3.2. Sensitivity
The pooled sensitivity for SLNB was 88% (95% CI: 81–94), as illustrated in the forest plot in Figure 3. Heterogeneity analysis revealed a Cochrane Q value of 36.2 (p = 0.0006) and an I^2^ index of 8.4%, indicating low heterogeneity.
Subgroup analyses for sensitivity highlighted differences based on mapping materials and tumor location. Blue dye injection yielded a pooled sensitivity of 77% (95% CI: 55–92), while radiotracer injection demonstrated superior sensitivity at 88% (95% CI: 80–94). Tumor location further impacted sensitivity outcomes, with supraglottic tumors showing a pooled sensitivity of 96% (95% CI: 88–99), significantly higher than transglottic tumors, which had a pooled sensitivity of 71% (95% CI: 52–86).
3.3. Quality Assessment
The quality of the included studies was evaluated using the Oxford Center for Evidence-Based Medicine checklist for diagnostic studies. Table 2 provides a detailed summary of the assessment, indicating that most studies adhered to high standards in patient recruitment, with consecutive or randomized inclusion, and robust application of reference standards, such as radical neck dissection. However, variability was observed in study design, particularly in the spectrum of patients and the completeness of blinding in reference standard application.
3.4. Publication Bias Evaluation
Publication bias was assessed through funnel plots and statistical methods. For detection rate, the funnel plot shown in Figure 4 displayed asymmetry, with Egger’s regression intercept calculated at 1.95 (p = 0.00006). After applying Duval–Tweedie’s trim and fill method and removing nine studies, the funnel plot achieved symmetry, resulting in an adjusted pooled detection rate of 81.8% (95% CI: 80.5–91.2), reflecting a 4% reduction from the original pooled rate.
For sensitivity, the funnel plot depicted in Figure 5 also showed asymmetry, with Egger’s regression intercept at 1.50 (p = 0.051). Following the removal of five studies through the trim and fill method, a symmetrical funnel plot was obtained. The adjusted pooled sensitivity was 76.4% (95% CI: 66.4–84.2), reflecting an 8% reduction from the observed pooled sensitivity.
4. Discussion
About 50% of people with laryngeal cancer survive at least 7 years, with 31% living 10 years or longer. Survival rates depend on cancer location and spread. Glottis cancer has the highest survival rate, with a 5-year survival of 84% if localized. Supraglottic cancer has the lowest survival rates, around 30–61% [4,5].
At present, SLNB is a well established approach for evaluating lymph node involvement in certain cancer types, including breast cancer, melanoma, and select urogenital cancers [43,44,45,46]. Ongoing research continues to explore the potential application of this technique in other malignancies [47].
In the context of laryngeal cancer, the use of SLNB remains a topic of debate due to the intricate anatomy of the larynx and its complex network of lymphatic drainage pathways through the neck [48,49]. The presence or absence of cervical lymph node involvement is a critical factor that significantly impacts the staging and prognosis of laryngeal cancer.
Anatomical considerations also play a key role in understanding the distribution pattern of lymph node metastasis, with levels II and III being the most commonly affected regions [6].
While imaging modalities such as CT, MRI, and PET-CT provide valuable insights into cervical nodal disease and systemic metastases, they have limitations in reliably excluding metastases in clinically node-negative (N0) necks [17].
Additionally, SLNB shows considerable promise as a technique for staging cervical lymph nodes [12,25]. The findings from our meta-analysis highlight its potential as a reliable diagnostic tool, especially given the high pooled detection rate and sensitivity reported. Our study identifies key parameters in laryngeal cancers: mapping material (blue dye vs. radiotracer) and tumor location (supraglottic vs. infraglottic). These factors are crucial in diagnosis and may influence the risk of false-negative results in sentinel lymph node biopsy. These results support the adoption of SLNB as an alternative to more invasive procedures for staging cervical lymph node involvement in patients with laryngeal SCC.
While imaging modalities such as CT, MRI, and PET-CT provide valuable information about cervical nodal disease and systemic metastases, they fall short in reliably excluding metastases in clinically node-negative (N0) necks (38). In this context, SLNB offers a promising alternative, and our meta-analysis provides strong evidence of its diagnostic accuracy in laryngeal SCC.
This systematic review demonstrated pooled detection rates and sensitivity for SLNB of 90.8% and 88%, respectively, with low heterogeneity across studies (I^2^ indices of 21.8% and 8.4%). These findings affirm the reliability of SLNB in assessing lymph node involvement. Additionally, further analysis of diagnostic performance revealed significant variations based on mapping techniques and tumor location.
Radiotracer injection emerged as the superior mapping method, achieving significantly higher detection rates (90.8%) and sensitivity (88%) compared to blue dye injection (81.5% and 77%, respectively). These results are consistent with previous studies and highlight the advantages of radiotracers in identifying sentinel nodes that are deeply embedded in tissue layers, where blue dye may be less effective [12,27,50]. Additionally, accidental damage to the lymphatic vessels can result in the extravasation of blue dye, which not only impairs the overall visibility of the surgical field but may also delay wound healing [27]. Moreover, some patients have experienced allergic or anaphylactic reactions to blue dye [51]. The choice of tracer material is thus a critical factor in optimizing SLNB outcomes and should be carefully considered in clinical practice.
The location of the tumor also played a pivotal role in the success of SLN mapping. Supraglottic tumors demonstrated significantly better outcomes, with detection rates of 93.7% and a sensitivity of 96%, compared to 84.7% and 71%, respectively, for transglottic tumors. This finding underscores the anatomical differences between these regions, which likely influence lymphatic drainage patterns and accessibility of sentinel nodes. Complex lymphatic drainage in the supraglottic region allows for the undetected spread to regional lymph nodes. Furthermore, supraglottic tumors are often more advanced and histologically aggressive than glottic tumors, even at early stages [52]. Clinicians should take tumor location into account when planning SLNB, as it may directly impact the diagnostic yield of the procedure.
Evaluation of publication bias revealed some asymmetry in the funnel plots for detection rate and sensitivity pooling. While the trim and fill method showed only a modest 4% reduction in the pooled detection rate, the adjusted sensitivity was reduced by 8%, indicating that publication bias could be a greater concern for sensitivity estimates. These findings suggest caution when interpreting sensitivity results, as smaller or less rigorous studies may disproportionately influence pooled estimates.
5. Conclusions
Overall, sentinel lymph node mapping demonstrates high diagnostic accuracy and reliability in staging cervical lymph nodes in laryngeal SCC, particularly when radiotracer techniques are employed. The technique is most effective in patients with supraglottic tumors, where the highest detection rates and sensitivity are observed. These findings support the adoption of SLNB as a viable alternative to more invasive staging procedures and provide valuable insights for optimizing its implementation in clinical practice.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Sanabria A. Shah J.P. Medina J.E. Olsen K.D. Robbins K.T. Silver C.E. Rodrigo J.P. Suárez C. Coca-Pelaz A. Shaha A.R. Incidence of occult lymph node metastasis in primary larynx squamous cell carcinoma, by subsite, T classification and neck level: A systematic review Cancers 202012105910.3390/cancers 1204105932344717 PMC 7225965 · doi ↗ · pubmed ↗
- 2Cho J.H. Lee Y.S. Sun D.I. Kim M.S. Cho K.J. Nam I.C. Kim C.S. Kim S.Y. Park Y.H. Joo Y.H. Prognostic impact of lymph node micrometastasis in oral and oropharyngeal squamous cell carcinomas Head Neck 201638 E 1777 E 178210.1002/hed.2431426676645 · doi ↗ · pubmed ↗
- 3Ferlito A. Rinaldo A. Controversies in the treatment of N 0 neck in laryngeal cancer: Neck dissection, no surgery or sentinel lymph node biopsy?ORL J. Oto-Rhino-Laryngol. Its Relat. Spec.20006228710.1159/00002777011054009 · doi ↗ · pubmed ↗
- 4Bradford C.R. Ferlito A. Devaney K.O. Mäkitie A.A. Rinaldo A. Prognostic factors in laryngeal squamous cell carcinoma Laryngoscope Investig. Otolaryngol.20205748110.1002/lio 2.353PMC 704265632128433 · doi ↗ · pubmed ↗
- 5Petrakos I. Kontzoglou K. Nikolopoulos T. Papadopoulos O. Kostakis A. Glottic and supraglottic laryngeal cancer: Epidemiology, treatment patterns and survival in 164 patients J. Buon 20121770070523335528 · pubmed ↗
- 6Sharbel D.D. Abkemeier M. Groves M.W. Albergotti W.G. Byrd J.K. Reyes-Gelves C. Occult metastasis in laryngeal squamous cell carcinoma: A systematic review and meta-analysis Ann. Otol. Rhinol. Laryngol.2021130677710.1177/000348942093774432608245 · doi ↗ · pubmed ↗
- 7Salzano G. Perri F. Maglitto F. Togo G. De Fazio G.R. Apolito M. Calabria F. Laface C. Vaira L.A. Committeri U. Pre-treatment neutrophil-to-lymphocyte and platelet-to-lymphocyte ratios as predictors of occult cervical metastasis in clinically negative neck supraglottic and glottic cancer J. Pers. Med.202111125210.3390/jpm 1112125234945723 PMC 8706672 · doi ↗ · pubmed ↗
- 8BayırÖ. ToptaşG. Saylam G. İzgi T.C. HanÜ. Keseroğlu K. Akyıldızİ. Korkmaz M.H. Occult lymph node metastasis in patients with laryngeal cancer and relevant predicting factors: A single-center experience Tumori J.202210843944910.1177/0300891621102697734192979 · doi ↗ · pubmed ↗