The Influence of Postmenstrual Age and Neurological Impairments on the Modified Pain Assessment Tool Score in Infants Admitted to Neonatal Intensive Care: A Retrospective Medical Record Review
Jamie Murray, Jeremy Lam, Jeewan Jyoti, Kaye Spence, Himanshu Popat, Emre Ilhan

TL;DR
This study found that the modified Pain Assessment Tool (mPAT) can be used for infants in NICUs regardless of their age or neurological impairments, though younger infants showed higher behavioral pain responses.
Contribution
The study provides evidence that the mPAT is suitable for assessing pain in infants regardless of postmenstrual age or neurological impairment.
Findings
Neither postmenstrual age nor neurological impairment predicted total mPAT or physiological pain scores.
Extremely-to-very preterm infants showed 3.7 times higher behavioral pain scores compared to term infants.
The mPAT is suitable for use in NICUs regardless of infant age or neurological status.
Abstract
Repetitive and prolonged experience of pain by infants in neonatal intensive care units (NICUs) may adversely affect growth and alter pain responses. The degree of infant prematurity and/or presence of neurological impairment (NI) may impact an infant's ability to behaviorally respond to pain. This study aimed to determine whether the scores on the mPAT, a widely used pain assessment tool, is impacted by postmenstrual age (PMA) at assessment, irrespective of neurological impairment. Data from medical records were collected on infants admitted to the NICU who underwent a pain assessment with the modified Pain Assessment Tool (mPAT) between March 2019 and September 2021. Total mPAT, behavioral, and physiological pain scores were independently analyzed using logistic regression to detect differences based on PMA categories (< 33 weeks, 33–36 weeks, ≥ 37 weeks) and presence of NI.…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
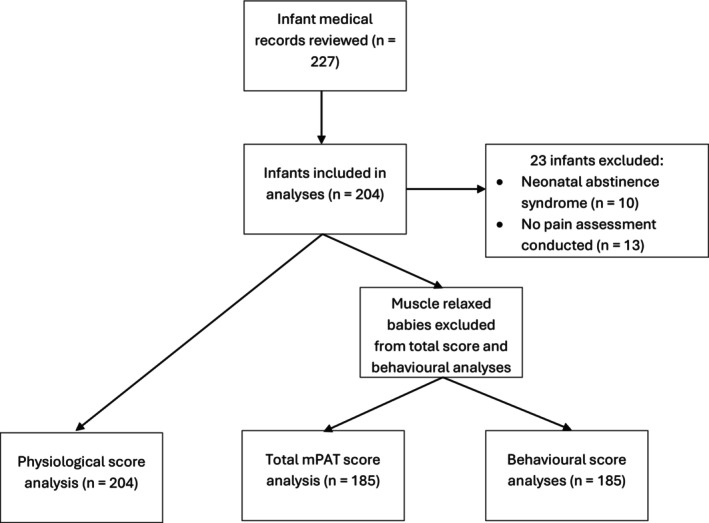 FIGURE 1
FIGURE 1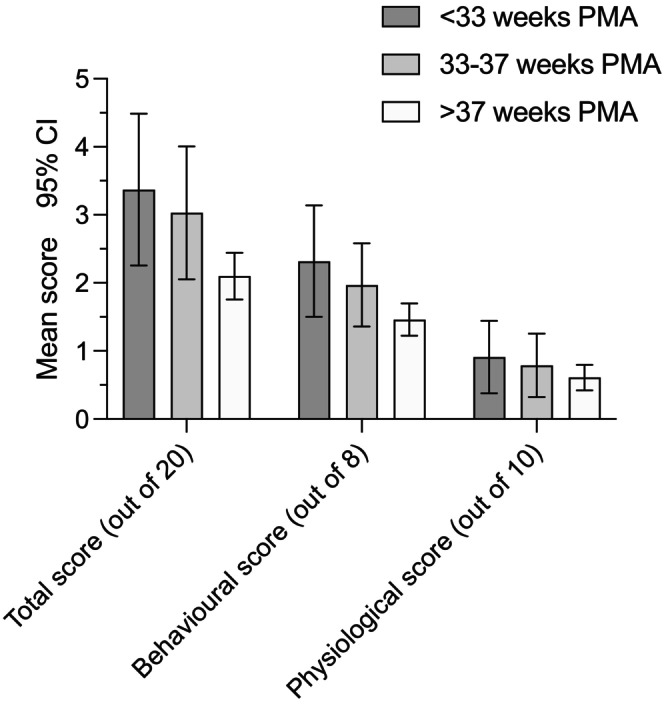 FIGURE 2
FIGURE 2| Points | ||||
|---|---|---|---|---|
| Dimension | Parameter | 0 | 1 | 2 |
| Behavioral | 1. Posture/Tone |
Normal Some flexion |
Digits widespread Trunk rigid Limbs drawn out Shoulders raised off bed |
Fists clenched Trunk guarded Limbs drawn to midline Head and shoulders resist posturing |
| 2. Cry | No |
Consolable Can be settled |
When disturbed Does not settle after handling Loud Whimpering Whining | |
| 3. Sleep Pattern | Relaxed | Easily woken |
Agitated or withdrawn Wakes with startle Restless Squirming No clear sleep/wake pattern Eye aversion ‘shut out’ | |
| 4. Expression |
Relaxed Normal |
Frown Shallow furrows Eyes lightly closed |
Grimace Deep furrows Eyes tightly closed Pupils dilated | |
| Physiological |
5. Color | Pink well perfused | Occasionally mottled or pale |
Pale/dusky/flushed Palmar sweating |
| 6. Respirations | Normal baseline rate | Tachypnoea—at rest | Apnea—at rest or with handling | |
| 7. Heart Rate | Normal baseline rate | Tachycardia—at rest | Fluctuating—spontaneous or at rest | |
| 8. Oxygen Saturation | Normal | Fleeting desaturation | Desaturation with or without handling | |
| 9. Blood Pressure | Normal | Hypo/hypertension at rest | ||
| Clinician's Perception | 10. Nurse's Perception | “No pain perceived” | “I think the baby is in pain only with handling” | “I think the baby is in pain” |
| Sex assigned at birth | |
| Male, | 127 (62%) |
| Female, | 77 (38%) |
| Gestational age (GA) at birth | |
| GA Mean ± SD, wks | 35.5 ± 4.8 |
| (< 33 wks) extremely‐to‐very preterm, | 50 (24%) |
| (33–37 wks) moderate‐to‐late preterm, | 38 (19%) |
| (37 ≥ wks) term, | 116 (57%) |
| Postmenstrual age (PMA) at the time of pain assessment | |
| PMA Mean ± SD, wks | 37.7 ± 3.7 |
| (< 33 wks) extremely‐to‐very preterm, | 22 (11%) |
| (33–37 wks) moderate‐to‐late preterm, | 38 (19%) |
| (37 ≥ wks) term, | 144 (70%) |
| Birth Weight | |
| Mean ± SD, gm | 2529.8 ± 1100 |
| Delivery Method | |
| Vaginal Delivery, | 84 (41%) |
| Cesarean Section, | 106 (52%) |
| Unknown, | 14 (7%) |
| Ventilation type at time of pain assessment | |
| % FiO2, Mean ± SD | 27.6 ± 17.1 |
| Spontaneous Ventilation—Room Air, | 93 (46%) |
| Non‐Invasive Ventilation, | 9 (4%) |
| Non‐Invasive Mechanical Ventilation, | 45 (22%) |
| Invasive Mechanical Ventilation, | 57 (28%) |
| Surgery | |
| Postsurgical patients at time of assessment, | 28 (14%) |
| Presence/Query neurological condition ( | 36 (18%) |
| Medication at time of pain assessment | |
| Analgesia, | 52 |
| Sedative, | 16 |
| Muscle relaxant, | 18 |
| Reasons for admission | |
| Surgical, | 113 (55%) |
| Medical, | 91 (45%) |
| Variables | mPAT total pain | Behavioral pain | Physiological pain | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| B | Lower | OR | Upper | Sig. | B | Lower | OR | Upper | Sig. | B | Lower | OR | Upper | Sig. | |
| Constant | −1.39 | 1 | 0.86 | 2.36 | −2.47 | 1 | |||||||||
| PMA 33–37 | 0.02 | 0.25 | 1.02 | 4.12 | 0.98 | −0.59 | 0.17 | 0.55 | 1.82 | 0.33 | 0.52 | 0.29 | 1.69 | 9.77 | 0.56 |
| PMA ≥ 37 | −0.88 | 0.12 | 0.42 | 1.45 | 0.17 | −1.29 | 0.1 | 0.27 | 0.77 | 0.01 | −0.38 | 0.14 | 0.69 | 3.42 | 0.65 |
| Neurological impairment | 0.25 | 0.43 | 1.29 | 3.86 | 0.65 | −0.31 | 0.33 | 0.73 | 1.62 | 0.44 | 0.61 | 0.54 | 1.84 | 6.26 | 0.33 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPediatric Pain Management Techniques · Infant Development and Preterm Care · Family and Patient Care in Intensive Care Units
Introduction
1
Advances in the neonatal intensive care unit (NICU) have led to neonates (infants less than 28 days old) and infants (less than 1 year old) surviving beyond hospitalization but also experiencing repeated painful procedures [1]. Neonates and infants can experience pain acutely following procedures such as heel lancing and nonacutely following major surgery [2]. The consequences of repeated painful procedures in the NICU include an increased risk of the development of prolonged pain [3], neurodevelopmental impairments [3], and alterations in pain sensitivity [1, 3], which highlight the importance of detecting pain accurately to minimize the negative effects of repeated pain later in life [1].
Pain assessment tools exist that measure various behavioral (e.g., muscular tone and facial expression) [4] and/or physiological indicators (e.g., heart rate and oxygen saturation) [4, 5], and/or contextual cues (e.g., gestational age), directing clinicians to appropriate pain reduction protocols [6]. Given the multidimensional nature of pain [7], such tools must incorporate behavioral and nonbehavioral indicators of pain [8], particularly as there is the potential for inappropriate pain management as a result of an underdetection of pain in preterm and neurologically impaired infants [8, 9, 10].
The Pain Assessment Tool (PAT) is a multidimensional pain assessment tool [11] that is currently used throughout NICUs in Australia and New Zealand. Recently, it has been modified to include additional descriptors to aid scoring, resulting in the modified PAT (mPAT) [12]. While the PAT has demonstrated reasonable inter‐rater reliability (intraclass correlation coefficient = 0.85) and concurrent validity (r = 0.76) for the use in detecting pain following surgery [13], the mPAT has demonstrated reasonable inter‐rater reliability (intraclass correlation coefficient = 0.83 at baseline, 0.86 at heel lance) and good concurrent validity (r = 0.81 at baseline, r = 0.91 at heel lance) for detecting acute episodic pain [12], highlighting a need to determine its use in nonacute pain states. The psychometric properties of the PAT and mPAT are comparable to other neonatal and infant pain assessment tools for use in the context of postsurgical and acute episodic pain [11]. The mPAT utilizes behavioral and physiological parameters as well as a stand‐alone, contextual item of nurse's perception to determine whether a neonate or infant is experiencing pain. It is used for nonacute pain, which specifically refers to pain that is not associated with an acute, noxious event. The mPAT, which is scored out of a total of 20 and indicates more intense pain with higher scores, is used to help decision‐making about pain management.
Guidelines for the use of the mPAT in guiding pain management stipulate adaptations based on the baseline state of the neonate or infant. Muscle‐relaxed and sedated infants are scored out of 12 by assessing only physiological parameters [14], as they will not have the ability to respond behaviorally. The mPAT, however, does not consider other variables that may minimize the expression of behavioral indicators of pain such as prematurity [8, 9]. In fact, discriminatory facial expressions in response to noxious stimuli seem to emerge at approximately 33‐weeks' gestation [15]. Consequently, it can be surmised that extremely and very preterm infants may lack the necessary motor capacity to mount a behavioral response to pain that is sufficient to be detected by clinicians. The problem of underdetection is compounded in the critical care setting of the NICU, where infants are sedated and muscle‐relaxed, further reducing their capacity to respond behaviorally to pain [16]. However, relying solely on physiological indicators of pain as a measure of pain may be inadequate, particularly as physiological markers such as heart rate are shown to be less responsive to noxious stimuli the more an infant is exposed to painful procedures [17].
The Échelle de Douleur et d'Inconfort du Nouveau‐né (EDIN) scale is behavioral neonatal pain assessment tool used for assessing prolonged pain in critically ill neonates and infants. It has demonstrated good levels of inter‐rater reliability and construct validity [18]. However, a study by Ancora et al. [19] found that the EDIN scale was better able to detect pain when the tool specifically accounted for gestational age (time elapsed from the last menstrual period to delivery date) and postmenstrual age (PMA, time elapsed since birth plus gestational age). Thus, the modified version of the EDIN scale assigned extra points to infants who were younger due to their reduced ability to express pain behaviorally. While previous research has validated the mPAT for acute pain assessment in infants born ≥ 24‐weeks' gestation [12], the mPAT requires further validation to assess nonacute pain and whether it is reliable across gestational ages.
Validation of the mPAT for potentially neurologically impaired populations is required, particularly as this cohort is often excluded from neonatal pain research. The facial expressions of neonates who are at higher risk of neurological impairment may not be as pronounced compared to those with no or lower risk of impairment [10, 20]. A survey conducted by Stevens et al. [21] found clinicians tend to rely more on physiological indicators than behavioral indicators during the assessment of acute pain in infants who are at risk of neurological impairment, which suggests that behavioral indicators of pain in this cohort may not be reliable.
Therefore, there is an obvious gap in knowledge leading to uncertainty about the reliability of using the mPAT for pain assessment in preterm and infants at risk of neurological impairment. To address this gap, the aim of the present study is to determine whether the mPAT is influenced by postmenstrual age at the time of assessment or the risk of neurological impairment. Therefore, this study has two research questions:
- Does postmenstrual age at the time of assessment influence the total score, and/or the behavioral and physiological scores of the mPAT?
- Does the risk of neurological impairment influence the total score, and/or the behavioral and physiological scores of the mPAT?
Methods
2
Study Design
2.1
This study was a retrospective analysis of medical records of infants that were admitted into Grace Centre for Newborn Intensive Care at the Children's Hospital Westmead, Sydney, Australia. This Centre is a Level III specialized unit at a tertiary hospital providing care to critically ill neonates and infants with complex medical conditions such as serious cardiac and surgical disorders. This study was designed to align with the STROBE checklist for cross‐sectional studies [22], with any missing components being supplemented by the ISPOR retrospective database analysis checklist [23]. This project (LNR/18/SCHN/298) was approved by the Human Research Ethics Committee of the Sydney Children's Hospital Network.
Eligibility Criteria
2.2
This study included all infants in the NICU who underwent a pain assessment using the mPAT between March 2019 and September 2021. Infants who did not undergo a pain assessment or infants with neonatal abstinence syndrome from maternal drug use were excluded from the study.
Data Collection
2.3
Data for this study were collected from an electronic medical record system (PowerChart, Cerner). Due to difficulty in obtaining time dependent variables, only the initial mPAT assessments conducted in the NICU were extracted and subsequent assessments were not extracted. Collected variables included scores on each of the mPAT parameters (Table 1), birthweight, sex assigned at birth, gestational age at birth, PMA at the time of mPAT assessment, primary reason for admission, query or presence of neurological impairment (e.g., Spina bifida and encephalopathy), any surgical procedures performed prior to the mPAT assessment, administration of medications such as analgesia, sedatives, or muscle relaxants within 12‐h prior to the initial pain assessment, ventilation type, clinician type, and action taken in response to the scoring of the pain assessment.
The mPAT
2.4
The modified Pain Assessment Tool (mPAT) comprises 10 parameters, each with corresponding descriptors, as shown in Table 1. Each item is scored on a scale of 0 to 2 and the aggregate score out of 20 is used to guide appropriate pain management. The clinician conducting the assessment observes the neonate's face and whole body for 2 min and then gently touches their limbs to evaluate muscle tone and record the scores. Any external factors that the clinician thought may have had an impact on the score should also be noted as well as the action(s) taken by the clinician as a result of the assessment [24]. Infants who are under the influence of muscle relaxants (e.g., vecuronium) are scored using only the physiological and nurse's perception parameters meaning that their total maximum score is 12 and the score thresholds to indicate are adjusted accordingly. Meaning ≥ 3 for pain requiring comfort care, and ≥ 5 for pain indicating analgesic management [14, 24].
Data Analysis
2.5
To detect variations in total mPAT score, behavioral and physiological pain subscores, infants were categorized based on PMA at assessment and neurological impairment risk status. PMA categories were classified as [19] extremely‐to‐very preterm (< 33 weeks), moderate‐to‐late preterm (33‐36 weeks), and term (≥ 37 weeks). Neurological impairment risk status was dichotomized to presence or suspicion of neurological impairment and no presence of neurological impairment. Infants who had muscle relaxants (e.g., vecuronium) within 12‐h prior to the initial pain assessment were excluded from any analyses.
The collected data were analyzed using IBM SPSS Statistics for Windows version 29.0.2.0 (Armonk, NY; IBM Corp). Logistic regression was used to analyze the influence of PMA and neurological impairment status on mPAT total score, as well as total behavioral and physiological pain scores, with a p value of < 0.05 indicating statistical significance. Prior to analysis, mPAT scores were dichotomized to indicate pain (a score > 5) or no pain. Because a score of > 5 equates to 30% of the total score, to evaluate behavioral pain separately, we calculated 30% of the total score of the behavioral items (30% of 8) to determine that a score ≥ 2 indicated behavioral pain. Similarly, to evaluate physiological pain separately, we calculated 30% of the total score of the physiological items (30% of 10) to determine that a score ≥ 3 indicated physiological pain. We used Nagelkerke's R ^2^ test to assess goodness‐of‐fit for logistic regression [25]. Based on the planned analyses, and proportion of infants with the outcome of interest set at 0.10, a desired power of 0.90, and a Type I error rate of 0.05, the minimum sample size required was 170 (jStat, JavaScript Library, 2023).
Results
3
Sample Demographics
3.1
Of the 204 infants included in this study (Table 2, Figure 1), most were male (62%) and born at term‐age (≥ 37 wks, 71%). The remaining infants were moderate‐to‐late preterm (33–36 wks, 19%) and extremely‐to‐very preterm (< 33 wks, 24%). Ninety‐one infants (45%) were admitted for medical reasons, while 113 infants were admitted primarily for surgical interventions.
Participant flow through the analysis. mPAT indicates modified Pain Assessment Tool.
Twenty‐four infants (13%) had a total mPAT score > 5 indicating the presence of pain, with three of these infants (2%) having a score ≥ 10 indicating severe pain. The average total pain score was 2.4 (SD: 2.2) (Figure 2). Nurses gave a score of 0 for nurse's perception of pain to 193 infants (90%).
Mean total mPAT, behavioral, and physiological scores by postmenstrual age (PMA) group. Error bars represent upper and lower bounds of 95% confidence intervals.
Eighty‐two infants (44%) had a total behavioral score ≥ 2 indicating the presence of pain. Sixteen infants (8%) had a total physiological score ≥ 3 indicating pain presence. Thirty‐six (18%) infants had a queried or confirmed neurological impairment; however, only five had a total mPAT score ≥ 5. Only 6 (21%) of 28 postsurgical infants had pain presence indicated.
The Impact of Neurological Impairment and Postmenstrual Age at Assessment on Pain Scores
3.2
The analysis of the total mPAT score (Table 3) revealed that neither PMA nor the risk of neurological impairment were associated with pain presence, χ ^2^(3) = 3.9, p > 0.05. However, the logistic regression model using the behavioral pain score as the dependent variable was found to be significant, χ ^2^(3) = 9.16, p < 0.05. While the risk of neurological impairment did not independently predict the presence of behavioral pain (i.e., score of ≥ 2), the odds of pain in infants < 33 weeks PMA at assessment was 3.7 times more than infants ≥ 37 weeks PMA (odds ratio = 0.27, 95% CI 0.10 to 0.77, p = 0.01). No other pairwise comparisons were statistically significant (Table 3). In the physiological pain model, neither PMA nor the risk of neurological impairment was associated with the presence of physiological pain, χ ^2^(3) = 2.7, p > 0.05.
Discussion
4
Our study demonstrated that PMA at assessment may not influence total mPAT or physiological pain scores. However, our findings demonstrated that extremely‐to‐very preterm infants (< 33 weeks PMA at assessment) were almost four times more likely to display behavioral indicators of pain than term‐age infants (≥ 37 weeks PMA). This study also demonstrated that the presence of neurological impairment did not influence the total mPAT score, and physiological or behavioral pain expression.
Influence of Neurological Impairment on the Expression of Pain
4.1
The results of this study indicate that the mPAT may be suitable for infants at risk of neurological impairment given that there was no significant difference in scores between those with and without risk of neurological impairment. A possible explanation can be found within the tool's scoring criteria for facial expression. Previous research has indicated that facial expression is a highly reliable, sensitive, and consistent behavioral indicator of pain [7, 10]; however, infants with neurological impairment may express fewer facial expressions than those without [20]. In a study by Gibbins et al. [26], it was established that brow bulge, eye squeeze and nasolabial furrow were the only facial expressions consistently indicating pain irrespective of neurological impairment. Thus, because these facial actions can be found within the mPAT, the mPAT may be suitable for assessing pain in infants at risk of neurological impairment. Alternatively, nurses' good clinical reasoning and understanding of contextual factors such as the impact of neurological impairment on pain expression may enable them to be more attuned to the behavioral expressions of infants with neurological impairment.
Influence of Post‐Menstrual Age on the Expression of Pain
4.2
The findings of our study contradict the current understanding that more premature infants are less likely to display behavioral indicators of pain due to immaturity of their nervous systems [15, 19, 26]. The higher behavioral scores in the extremely‐to‐very preterm infants compared with term infants in our study may be interpreted in two ways. Firstly, it is possible that the modifications made to the PAT provides criteria that allows nurses to adequately assess pain behaviorally regardless of an infant's PMA at assessment. This is consistent with O'Sullivan et al.'s [12] findings which demonstrated no significant difference in mean total mPAT scores between the three gestational age groups (≤ 28 wks, 28–37 wks, and ≥ 37 wks). The study also considered that the tool's criteria include precise descriptors such as “clenched fists” that preterm infants are capable of performing [12]. Thus, it can be hypothesized that the mPAT provides nurses more clarity as to what is considered normal or abnormal through the addition of descriptive criteria along the spectrum of behaviors that could indicate pain. These additional descriptors were not previously included in the PAT. It should be noted, however, that the study by O'Sullivan et al. [12] evaluated the mPAT following a painful procedure (i.e., acute pain states). Therefore, it is possible that responses to pain that is ongoing or prolonged, as was the case in our study, may be even more difficult to detect in extremely‐to‐very preterm infants. Indeed, there is an urgent need to develop tools for non‐acute pain that is appropriate across the developmental age spectrum [27].
The second interpretation could be explained by the ramifications of premature extrauterine exposure meeting specific behavioral criteria. The extrauterine life creates challenges for early development due to losing the antigravity, dark, quiet, and temperature‐regulated environment that they had while in utero [28]. Given that premature infants are often hypotonic and lack the independent or passive ability to flex against gravity, extension becomes an overpowering force [29, 30]. An “extended posture” meets the criteria for one point to be allocated behaviorally, despite the fact that preterm infants may not be able to functionally perform “some flexion” which is considered as normal in the mPAT descriptor for posture/tone. Similarly, “eyes tightly closed” and “no clear sleep/wake‐pattern” as descriptors for expression and sleep pattern, respectively, are criteria that could better be accounted for by nonpainful responses to the environment such as the stress related to exposure to light, noise, and frequent procedures/handling [31]. Indeed, a study conducted by Grunau et al. [32] found that preterm infants have a lower threshold and a more pronounced reflex response to touch compared with full‐term infants. Although nurses may consider extrauterine effects when assessing pain, we could not identify any instances where nurses documented external influences to scoring despite this being part of the NICU's mPAT protocol (e.g., noisy environment disturbing sleep pattern) [24]. Nevertheless, these possible explanations require further research to identify which specific descriptors (e.g., extended and clenched fists) nurses are recognizing more frequently across PMA groups.
Nurses' Perception of Pain
4.3
By analyzing the behavioral and physiological indicators on the mPAT separately, our results suggest that more infants expressed pain behaviorally. This analysis has provided further evidence that behavioral and physiological indicators of pain do not necessarily correlate with one another [9]. Nurses' perception of pain may enable a context‐informed evaluation of pain but should be used in combination with behavioral and physiological indicators. Future research should explore how nurses score this final criterion of the mPAT to further refine how the score can be utilized to improve the detection of pain and increase inter‐rater reliability.
Strengths and Limitations
4.4
This study had several strengths. Firstly, the study used a dataset that was acquired from a clinical cohort of interest. Secondly, this study was inclusive of infants with potential neurological impairments and did not exclude any gestational age groups. However, because this study was a retrospective record review, it was difficult to estimate the extent of missing data. This also meant we were unable to accurately identify the number of painful procedures infants underwent prior to the assessment of their pain. Finally, given the retrospective nature of this study, several unknown factors—for example, time of assessment and proximity to a painful procedure, and use of analgesia—may have influenced the findings which would better be controlled for in a prospective study. It should also be noted that there were approximately six times fewer infants in the youngest PMA group compared with the oldest PMA group. It is possible that clinicians in the unit may have administered the mPAT on younger infants only if they displayed highly visible signs of pain.
Conclusions
5
The assessment of nonacute pain in NICUs is a relatively underexplored area of research that is urgently needed to improve pain detection. This study evaluated the changes in total, behavioral, and physiological indicators of pain using the mPAT in relation to PMA at assessment and neurological impairment. Although this study demonstrated that postmenstrual age and neurological impairment may not affect the expression of pain as assessed by the mPAT, further work is needed to validate the mPAT as a measure of nonacute pain. Furthermore, the high behavioral responses in younger infants and neonates are unusual which requires further exploration in a future prospective study.
Ethics Statement
This project (LNR/18/SCHN/298) was approved by the Human Research Ethics Committee of the Sydney Children's Hospital Network.
Consent
This was a retrospective medical record review.
Conflicts of Interest
The authors declare no conflicts of interest.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1R. E. Grunau , L. Holsti , and J. W. Peters , “Long‐Term Consequences of Pain in Human Neonates,” Seminars in Fetal & Neonatal Medicine 11, no. 4 (2006): 268–275.16632415 10.1016/j.siny.2006.02.007 · doi ↗ · pubmed ↗
- 2K. J. S. Anand , “Defining Pain in Newborns: Need for a Uniform Taxonomy?,” Acta Paediatrica 106, no. 9 (2017): 1438–1444.28556311 10.1111/apa.13936 PMC 5601230 · doi ↗ · pubmed ↗
- 3H. Bouza , “The Impact of Pain in the Immature Brain,” Journal of Maternal‐Fetal & Neonatal Medicine 22, no. 9 (2009): 722–732.19526425 10.3109/14767050902926962 · doi ↗ · pubmed ↗
- 4C. Johnston , M. Campbell‐Yeo , T. Disher , et al., “Skin‐To‐Skin Care for Procedural Pain in Neonates,” Cochrane Database of Systematic Reviews 2, no. 2 (2017): Cd 008435.28205208 10.1002/14651858.CD 008435.pub 3PMC 6464258 · doi ↗ · pubmed ↗
- 5V. A. Howard and F. W. Thurber , “The Interpretation of Infant Pain: Physiological and Behavioral Indicators Used by NICU Nurses,” Journal of Pediatric Nursing 13, no. 3 (1998): 164–174.9640010 10.1016/s 0882-5963(98)80075-4 · doi ↗ · pubmed ↗
- 6J. Foster , K. Spence , D. Henderson‐Smart , D. Harrison , P. H. Gray , and J. Bidewell , “Procedural Pain in Neonates in Australian Hospitals: A Survey Update of Practices,” Journal of Paediatrics and Child Health 49, no. 1 (2013): E 35–E 39.23279125 10.1111/jpc.12064 · doi ↗ · pubmed ↗
- 7Y. Lim and S. Godambe , “Prevention and Management of Procedural Pain in the Neonate: An Update, American Academy of Pediatrics, 2016,” Archives of Disease in Childhood. Education and Practice Edition 102, no. 5 (2017): 254–256.28724533 10.1136/archdischild-2016-311066 · doi ↗ · pubmed ↗
- 8S. J. Morison , R. E. Grunau , T. F. Oberlander , and M. F. Whitfield , “Relations Between Behavioral and Cardiac Autonomic Reactivity to Acute Pain in Preterm Neonates,” Clinical Journal of Pain 17, no. 4 (2001): 350–358.11783816 10.1097/00002508-200112000-00010 PMC 1852479 · doi ↗ · pubmed ↗