Aspirin Desensitization in the Course of Non-ST-Segment Elevation Acute Coronary Syndrome: A Case Report and Review of the Literature
Hicham Faliouni, Lalla Ghita Alaoui, Youssef Fihri, Mehdi Laaroussi, Mouad Lamtai, Zouhair Lakhal, Aatif Benyass

TL;DR
This paper presents a case where a patient allergic to aspirin was successfully desensitized to allow necessary heart treatment.
Contribution
The study demonstrates the feasibility of aspirin desensitization in managing aspirin-allergic patients with acute coronary syndrome.
Findings
A patient with NSTEMI and aspirin allergy successfully underwent aspirin desensitization.
Desensitization allowed initiation of dual antiplatelet therapy after angioplasty.
The case supports the use of desensitization protocols in cardiac emergencies.
Abstract
Antiplatelet therapy is essential for patients with acute coronary syndrome (ACS). Aspirin (acetylsalicylic acid, or ASA) is one of the most commonly used medications for this purpose, particularly in the context of dual antiplatelet therapy (DAPT). However, hypersensitivity to aspirin can pose significant challenges, especially when this treatment is indispensable. This report discusses the case of a patient with non-ST-segment elevation myocardial infarction (NSTEMI) who presented with an allergic reaction to aspirin. An aspirin desensitization protocol was successfully implemented, allowing for the initiation of DAPT following dual angioplasty. This case highlights the importance and feasibility of aspirin desensitization in ensuring optimal management of patients with aspirin allergy, in a cardiac emergency setting.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
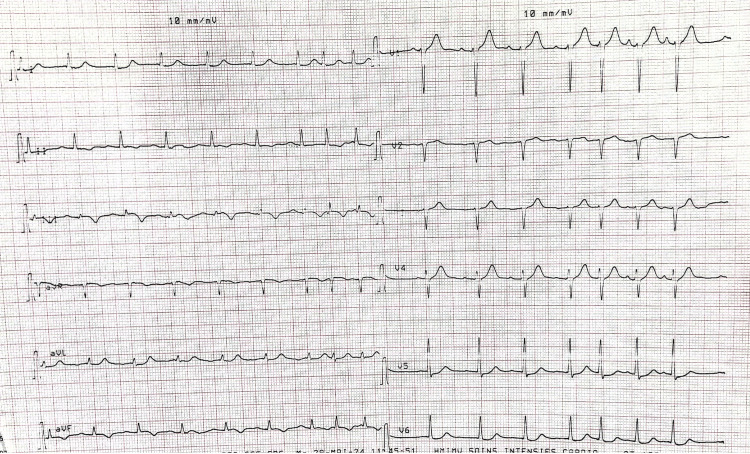 Figure 1
Figure 1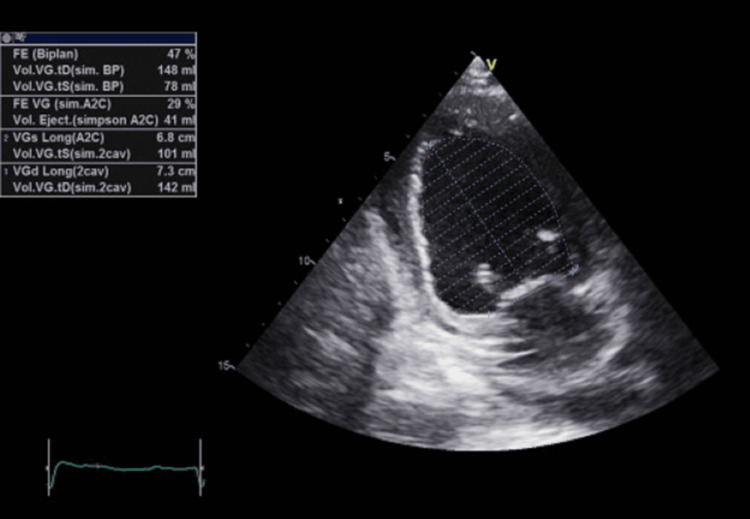 Figure 2
Figure 2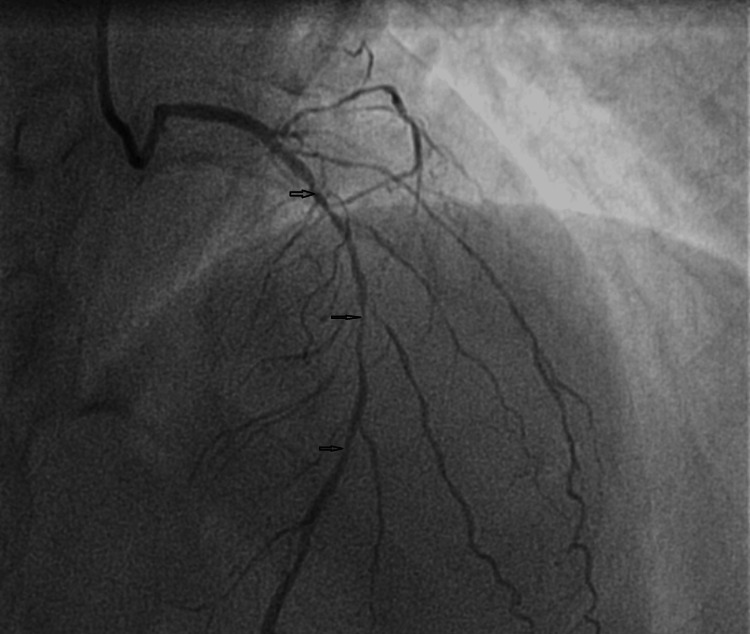 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAntiplatelet Therapy and Cardiovascular Diseases · Atrial Fibrillation Management and Outcomes · Acute Myocardial Infarction Research
Introduction
Antiplatelet therapy is essential for patients with acute coronary syndrome (ACS). Aspirin is considered the reference treatment due to its efficacy, availability, and low cost, particularly in developing countries [1]. It is widely recommended for the management of ST-segment elevation myocardial infarction (STEMI) and non-ST-segment elevation myocardial infarction (NSTEMI) ACS, with demonstrated survival benefits, as shown in the ISIS-2 trial [2]. The combination of aspirin with a P2Y12 receptor antagonist, known as dual antiplatelet therapy (DAPT), is especially important when a coronary stent is implanted.
Managing ACS patients with hypersensitivity to aspirin poses significant challenges. However, studies have shown that aspirin desensitization is effective for patients requiring secondary prevention of cardiovascular events [3]. Alternative strategies include the use of P2Y12 receptor inhibitors such as clopidogrel, prasugrel, or ticagrelor, which can partially replace aspirin in monotherapy. Additionally, aspirin desensitization protocols offer a safe and effective option for reintroducing aspirin, thereby enabling optimal DAPT. These approaches are crucial in ensuring the prevention of thrombotic complications in patients sensitive to aspirin.
In this case report, we describe a short and successful desensitization protocol applied to a patient who experienced a hypersensitivity reaction to aspirin, during its introduction in the setting of NSTEMI ACS.
Case presentation
This is a 72-year-old patient with multiple cardiovascular risk factors: a 15-year history of poorly controlled type 2 diabetes treated with oral antidiabetic agents, newly diagnosed hypertension managed with angiotensin-converting enzyme (ACE inhibitors) and amlodipine besylate, and a history of dyslipidemia, treated with statins. The patient also has a smoking history but quit 15 years ago.
The patient presented to the Emergency Department with typical chest pain at rest, lasting for 30 minutes, initially neglected, and complicated by several recurrences on the day of admission.
Physical examination on admission was unremarkable. The electrocardiogram showed negative T waves in the inferior territory, along with ST-segment depression in the low lateral territory (Figure 1). Biological analysis revealed a troponin level, 200 times above the normal range. A diagnosis of high-risk NSTEMI ACS was established.
Electrocardiogram on admissionAn electrocardiogram shows attenuation of the R-wave in the anteroseptal territory, ST-segment depression in the lateral territory, and negative T waves in the inferior territory, consistent with myocardial ischemia.
The transthoracic echocardiography revealed a normal-sized left ventricle and a non-hypertrophied left ventricle with segmental wall motion abnormalities. Specifically, there was akinesia of the basal and middle segments of the inferoseptal wall, as well as akinesia of the apex and adjacent segments. Additionally, hypokinesia of the basal segment of the inferior wall was noted, with moderately impaired systolic function and an ejection fraction of 47%, with no visible thrombus (Figure 2).
Transthoracic echocardiographyA transthoracic echocardiography two-chamber shows moderately impaired systolic function and an ejection fraction of 47%.
On the day of admission, the physical examination was unremarkable. The patient was given a loading dose of antiplatelet agents, consisting of 300 mg of aspirin and 300 mg of clopidogrel administered orally, along with low-molecular-weight heparin by subcutaneous injection. One hour after administration, the patient developed a generalized pruritic rash, with skin redness on the upper trunk. He was admitted to the Cardiac Intensive Care Unit (CICU) and treated with injectable corticosteroids and antihistamines. The rash resolved completely by the second day of treatment.
Given the patient’s high ischemic risk and the allergic reaction to aspirin, a rapid aspirin desensitization procedure was implemented to ensure prolonged and effective platelet aggregation inhibition. The procedure was performed in the CICU, under close supervision with corticosteroid and antihistamine coverage.
The desensitization protocol spanned six hours and involved incremental doses of aspirin: 0.1 mg, 1 mg, 5 mg, 10 mg, 20 mg, 50 mg, and 75 mg, administered at one-hour intervals, reaching a cumulative dose of 160 mg. Then, the patient was transferred to the catheterization laboratory. The coronary angiography (Figure 3) was performed via the radial approach and revealed a very long and multi-segment stenosis involving the proximal and middle segments of the left anterior descending artery (LAD). The LAD gives rise to four small-caliber diagonal branches (less than 2 mm in diameter), of which the first three exhibit significant stenoses, making the lesion unsuitable for percutaneous intervention and favoring medical management, which was chosen due to the lesion's anatomical complexity and the patient's clinical stabilization. This approach aligns with current guidelines for NSTEMI management in stable patients with anatomically challenging lesions.
Coronary angiographyCoronary angiography revealed a very long and multi-segment stenosis involving the proximal and middle segments of the LAD (black arrows). The LAD gives rise to four small-caliber diagonal branches (less than 2 mm in diameter), of which the first three exhibit significant stenoses.LAD: left anterior descending artery
Then, the patient was discharged on DAPT consisting of aspirin 75 mg daily and clopidogrel 75 mg daily, and he tolerated the desensitization procedure without any significant allergic reactions.
Discussion
Antiplatelet therapy, particularly DAPT combining aspirin and a P2Y12 receptor inhibitor, is essential in the management of ACS. This approach significantly reduces the risk of recurrent ischemic events and stent thrombosis following percutaneous coronary intervention (PCI) [4]. However, managing patients with aspirin hypersensitivity presents a significant challenge.
In our case, the patient developed an allergic reaction shortly after aspirin administration, complicating the continuation of standard treatment. The aspirin allergy was previously unknown, but its occurrence in an emergency setting necessitated rapid and effective management to prevent ischemic complications. Aspirin desensitization was therefore, chosen as the therapeutic strategy.
Rapid desensitization allowed for the safe reintroduction of aspirin without recurrence of the allergic reaction. The protocol was conducted under close supervision in the ICU, with corticosteroid and antihistamine coverage, in line with recommendations from the literature [5]. Several studies confirm the efficacy and safety of this approach, particularly in patients at high ischemic risk, where the alternative of monotherapy with a P2Y12 inhibitor may be insufficient to prevent thrombotic events [6,7].
Aspirin remains the cornerstone of antiplatelet therapy, and its combination with a P2Y12 inhibitor is strongly recommended after PCI, especially when an active stent is present [8]. The omission of aspirin could expose the patient to a heightened risk of severe cardiovascular complications. Studies have reported that aspirin desensitization achieves tolerance in over 90% of cases, enabling successful long-term reintroduction [5,9]. These findings align with our experience, as desensitization was well tolerated, and enabled secure management of the patient.
This case underscores the importance of aspirin desensitization in scenarios where aspirin allergy occurs following ACS. Having an appropriate protocol and a trained team to execute the procedure is crucial, as it offers an effective, rapid, and safe solution to maintain optimal antiplatelet therapy [10]. Additionally, it highlights the importance of meticulous follow-up after desensitization to monitor for potential allergic recurrence or treatment-related complications.
Conclusions
The case highlights the effectiveness of rapid aspirin desensitization in a high-risk NSTEMI patient with aspirin hypersensitivity. For successful implementation of desensitization protocols in low-resource settings, it is crucial to simplify the protocol, utilize available medications such as corticosteroids and antihistamines, for supportive care, and ensure close monitoring in an ICU setting. Training medical staff and having clear, structured protocols can help mitigate challenges posed by resource limitations, ensuring safe and effective patient management.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Collaborative meta-analysis of randomised trials of antiplatelet therapy for prevention of death, myocardial infarction, and stroke in high risk patients BMJ Antithrombotic Trialists'Collaboration 718632420021178645110.1136/bmj.324.7329.71PMC 64503 · doi ↗ · pubmed ↗
- 2Randomized trial of intravenous streptokinase, oral aspirin, both, or neither among 17,187 cases of suspected acute myocardial infarction Lancet ISIS-2 (Second International Study of Infarct Survival) Collaborative Group 3493603321988 https://www.thelancet.com/journals/lancet/article/PIIS 0140-6736(88)92833-4/fulltext 2899772 · pubmed ↗
- 3Aspirin hypersensitivity in patients with coronary artery disease: an updated review and practical recommendations Biomolecules Cappannoli L Colantuono S Animati FM 13291420243945626210.3390/biom 14101329 PMC 11506836 · doi ↗ · pubmed ↗
- 4Rapid oral challenge-desensitization for patients with aspirin-related urticaria-angioedema J Allergy Clin Immunol Wong JT Nagy CS Krinzman SJ Maclean JA Bloch KJ 997100110520001080818210.1067/mai.2000.104571 · doi ↗ · pubmed ↗
- 5Hypersensitivity to nonsteroidal anti-inflammatory drugs (NSAI Ds) - classification, diagnosis and management: review of the EAACI/ENDA# and GA 2LEN/HANNA*Allergy Kowalski ML Makowska JS Blanca M 8188296620112163152010.1111/j.1398-9995.2011.02557.x · doi ↗ · pubmed ↗
- 6Aspirin-induced asthma: advances in pathogenesis and management J Allergy Clin Immunol Szczeklik A Stevenson DD 51310419991040083210.1016/s 0091-6749(99)70106-5 · doi ↗ · pubmed ↗
- 7Aspirin desensitization in patients undergoing planned or urgent coronary stent implantation. A single-center experience Int J Cardiol De Luca G Verdoia M Binda G Schaffer A Suryapranata H Marino P 56156316720132236531310.1016/j.ijcard.2012.01.063 · doi ↗ · pubmed ↗
- 82016 ACC/AHA guideline focused update on duration of dual antiplatelet therapy in patients with coronary artery disease: a report of the American College of Cardiology/American Heart Association Task Force on clinical practice guidelines: An update of the 2011 ACCF/AHA/SCAI guideline for Percutaneous Coronary Intervention, 2011 ACCF/AHA guideline for coronary artery bypass graft surgery, 2012 ACC/AHA/ACP/AATS/PCNA/SCAI/STS guideline for the diagnosis and management of patients with stable ischem