Pulmonary rehabilitation under supervision of health-professional at institute versus conventional exercise-based pulmonary rehabilitation at home in COPD patients: A longitudinal cohort study
Guxiang Zhang, Jiajing Yu, Zhiqiang Pei, Fei Xie, Ruiyang Ding, Lili Bao, Anyang Li

TL;DR
Institute-based pulmonary rehabilitation with professional supervision improves COPD outcomes more than home-based exercise programs in China.
Contribution
Demonstrates the superior efficacy of supervised institute-based pulmonary rehabilitation over home-based methods for COPD patients in China.
Findings
Institute-based rehabilitation improved walking test results and reduced BODE index scores and exacerbations after 6 months.
Patients in the institute cohort had significantly better outcomes compared to home-based and no-rehabilitation groups.
Chinese COPD patients face higher risks of undertreatment without proper rehabilitation.
Abstract
•Guidelines recommended pulmonary rehabilitation in COPD.•Self-driven pulmonary rehabilitation is an undertreatment for COPD patients in China.•Chinese patients with COPD have worse clinical conditions.•Treatment with pulmonary rehabilitation at institutes improves clinical outcomes.•Chinese COPD patients are required to be treated as per proper guidelines. Guidelines recommended pulmonary rehabilitation in COPD. Self-driven pulmonary rehabilitation is an undertreatment for COPD patients in China. Chinese patients with COPD have worse clinical conditions. Treatment with pulmonary rehabilitation at institutes improves clinical outcomes. Chinese COPD patients are required to be treated as per proper guidelines. To evaluate the efficacy and safety of pulmonary rehabilitation under the supervision of health professionals at the institute versus conventional exercise-based pulmonary…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
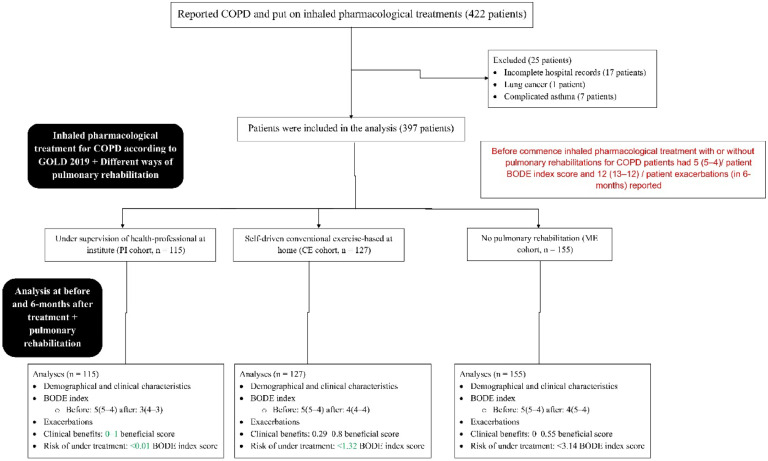 Figure 1
Figure 1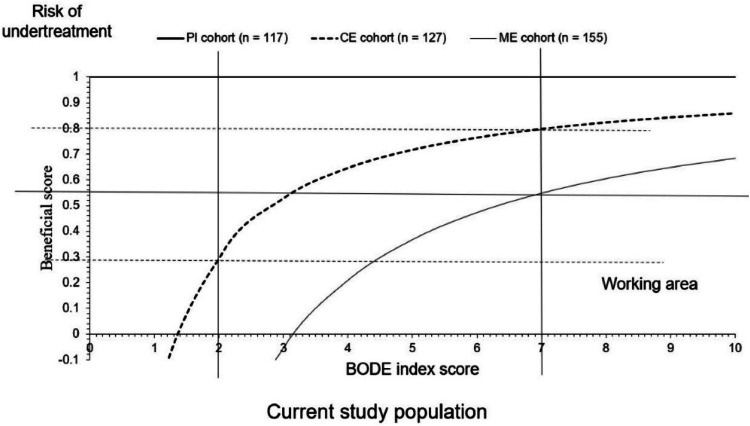 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsChronic Obstructive Pulmonary Disease (COPD) Research · Health and Wellbeing Research · Respiratory Support and Mechanisms
Introduction
Chronic Obstructive Pulmonary Disease (COPD) is a chronic lung disease that is associated with several factors.1 In COPD, patients have chronic airflow limitation because of airway and/or alveolar abnormalities.2 Pulmonary rehabilitation is an important component of the management of COPD3 because it is an evidence-based non-treatment intervention in symptomatic COPD patients in stable or exacerbations conditions.4 COPD is most prevalent in China but knowledge regarding its conditions and treatments is insufficient.5 In addition, in Chinese primary healthcare institutions, physicians have insufficient knowledge of pulmonary rehabilitation in COPD,6 Large numbers of patients with COPD are underdiagnosed and non-adherent to treatments in Chinese primary healthcare institutions.7 Several international guidelines recommend pulmonary rehabilitation for COPD.8 Chinese medicine lung rehabilitation body recommends Chinese traditional therapies (simplified Taijiquan, Baduanjin, Liuzijue, acupoint application therapy, acupuncture, Moxibustion, and pulmonary Daoyin) and the Western type modern therapies (physical exercise and relaxation therapies) to help treatment of pulmonary diseases and preserve physical and mental health.9 Different intensities of pulmonary rehabilitation are effective in different categories of COPD.10 Pulmonary rehabilitation improves the quality of life of patients with COPD.11 In addition, pulmonary rehabilitation improves dyspnea in routine life and decreases fat levels in the body among overweight and obese patients with compromised respiratory functions.12 However, the effects of pulmonary rehabilitation under the supervision of healthcare at institutes for COPD patients have not been evaluated, yet in Chinese settings. In China, there are significant discriminations among different settings for the management of COPD patients. In almost every patient in a home-based self-driven pulmonary rehabilitation is undertreatment.7
The objectives of retrospectively collected medical records analyses of data of COPD patients were to evaluate the short-term effects of pulmonary rehabilitation under the supervision of healthcare at institutes against self-driven conventional short-term exercise-based pulmonary rehabilitation at home against those who did not receive any type of pulmonary rehabilitation at institutes or home except follow-up visits of consultants at 45 days.
Materials and methods
Ethics approval and consent to participate
The designed protocols of the established study were prepared by the authors themselves and approved by the human ethics committee of the Affiliated Hospital of West Anhui Health Vocational College (Approval number 15WAHVCfA dated May 14, 2024). The study was conducted following the 2008 Declaration of Helsinki and the law of China. Informed consent was waived by the human ethics committee of the Affiliated Hospital of West Anhui Health Vocational College (because of the retrospective study).
Inclusion criteria
Patients with reported COPD by a pulmonologist and under treatment and advised for pulmonary rehabilitation were included in the study.
Exclusion criteria
Patients with incomplete hospital records (missing of a minimum three important parameters), patients with reported lung cancer, and patients with complicated asthma were excluded from the study.
Treatments of COPD
Patients followed the Global Initiative for Chronic Obstructive Lung Disease (GOLD) 2019 inhaled pharmacological treatment for COPD.13
Sample size calculations
The study assumed that using pulmonary rehabilitation at institutes or at home with treatments of COPD could reduce −10 % of BODE (body-mass index, airflow obstruction, dyspnea, and exercise capacity; primary outcome) index score after treatments of COPD with or without pulmonary rehabilitation of 6 months (effect size).10 Besides that, α = 0.5, β = 0.1, and 95 % of the Confidence Interval, using OpenEpi (Open-Source Epidemiologic Statistics for Public Health, Version. www.OpenEpi.com), a total of 105 patients required in each cohort (sample size). The differences were calculated by subtracting the mode value of the BODE index score of the ME cohort before the commencement of inhaled treatment from the BODE index score of individual patients 6 months after the commencement of inhaled pharmacological treatment for COPD with or without pulmonary rehabilitation.
Cohorts
A total of 115 patients with COPD received pulmonary rehabilitation under the supervision of health professionals at the institutes (PI cohort). A total of 127 patients with COPD received self-driven conventional exercise-based pulmonary rehabilitation at home (CE cohort). A total of 155 patients with COPD did not receive any type of pulmonary rehabilitation at the institute or home except follow-up visits of consultants at 45 days (ME cohort). Besides pulmonary rehabilitation patients with COPD received inhaled pharmacological treatment for COPD according to GOLD 2019.13
Different ways of pulmonary rehabilitation
Pulmonary rehabilitation at institutes
Pulmonary rehabilitation of patients with COPD at institutes performed under the supervision of healthcare professionals. Healthcare professionals followed the Chinese medicine lung rehabilitation body9 recommendations for pulmonary rehabilitation. Healthcare-professional was available every day for 1 h from 8 to 9am. Patients had to attend sessions of minimum 2 days in week. Healthcare professionals (nursing staff or pharmacists) were available on phone calls.
Pulmonary rehabilitation at home
Patients with COPD performed self-driven conventional exercise-based pulmonary rehabilitation at home. The conventional exercise included Chinese traditional therapies (simplified Taijiquan, Baduanjin, Liuzijue, acupoint application therapy, acupuncture, Moxibustion, and pulmonary Daoyin). Patients performed conventional exercises at their convinces (in the morning or evening; one hour or half an hour every day or two to three times a week).
Outcome measures
Demographical and clinical characteristics
Demographical and clinical characteristics before the commencement of pulmonary rehabilitation including patients’ habits were collected from patients’ electronic records and analyzed.
BODE index
The primary outcome of the study was the BODE index. Body Mass Index (BMI) was calculated for patients in kg/m^2^. If BMI was >21 kg/m^2^ then the score was 0 and if BMI was 21 kg/m^2^ or less then the score was 1. The obstruction parameter of the BODE index was evaluated using the FEV1 % predicted (plethysmography was used to calculate the FEV1 % predicted).10 If the FEV1 % predicted was 65 % or more then the score was 0. If the FEV1 % predicted was 50–64 % then the score was 1. If the FEV1 % predicted was 36–49 % then the score was 2. For FEV1 % predicted 35 or less than the score was 3. The modified Medical Research Council (mMRC) dyspnea scale (Table 1)10^,^14 was used to evaluate the intensity of dyspnea in routine life.Table 1. The modified Medical Research Council (mMRC) dyspnea scale.Table 1. Different conditionsScaleCorresponding scale score used in BODE calculationsBreathless only with strenuous exercise00Short of breath when walking up a slight hill or hurrying on the ground10Short of breath on a large walking21Short of breath normally in walking32Short of breath during normal daily work43Conditions were self-assessed and validated by healthcare professionals.
If patients walked 350 m or more distance in 6 min then the score was 0 if they walked 250–349 m distance in 6 min then the score was 1 if they walked 250–150 m distance in 6 min then the score was 2, and for <150 m distance in 6 min, then score was 3. All three points were summed to calculate the BODE index. The score range was 0–10. Higher the score the worse the conditions.10
Six minutes walking test
The distance covered in meters in 6 min under the supervision of a healthcare professional was considered.10
Exacerbations
Severe coughing and required hospitalization were considered exacerbations.10
Outcome measures were evaluated after 6 months after inhaled pharmacological treatment for COPD with or without pulmonary rehabilitation at institutes.
Adverse effects
Any adverse effects of pulmonary rehabilitation and/or inhaled pharmacological treatment for COPD during 6 months were evaluated.
Clinical benefits for inhaled pharmacological treatment (with or without pulmonary rehabilitation)
Clinical benefits for inhaled pharmacological treatment of patients with COPD with or without pulmonary rehabilitation were evaluated as a function of the beneficial scores. The beneficial scores for inhaled pharmacological treatment of patients with COPD for different ways of pulmonary rehabilitation were calculated from the risk of under-treatment as expressed in Eq. (1). The risk of under-treatment was defined with a calculation that involves the BODE index score below which inhaled pharmacological treatment for COPD with or without pulmonary rehabilitation were not effective for patients with COPD (Eq. (2)). The BODE index score was considered as a numerical value from 0 to 10. The beneficial score for inhaled pharmacological treatment of patients with COPD for different ways of pulmonary rehabilitation is the area above the curve of the inhaled pharmacological treatment of patients with COPD with adopted pulmonary rehabilitation and the working area is the area under the curve of the inhaled pharmacological treatment of patients with COPD with adopted pulmonary rehabilitation. For all adopted pulmonary rehabilitation with inhaled pharmacological treatments, more than −10 % differences (with respect to the initial value of ME cohort patients) in the BODE index score were used as the reference standard.15 The differences in % in the BODE index score were calculated from Eq. (3).
Statistical analyses
InStat 3.01 was used for statistical analyses of variables. Non-normal continuous, categorial, and normal continuous variables are depicted as median with Q3–Q1 in parenthesis, frequencies with percentages in parenthesis, and mean ± Standard Deviation (SD), respectively. ꭓ^2^-test (Chi-Square test for large tables) or Fisher exact test (2 × 2 tables) was preferred for statistical analyses of categorical variables. Soup calculator® was used to calculate quartile values. Kruskal-Wallis’ test or Mann-Whitney test (between cohort) and Wilcoxon matched-pairs signed-ranks test or Friedman test (nonparametric repeated measures analysis of variance [ANOVA]) were used for statistical analysis of non-normal continuous variables. All results were considered significant if the p-value was <0.05.
Results
Study populations
From January 15, 2020, to March 18, 2022, a total of 422 patients with reported COPD and put on inhaled pharmacological treatments at the parent hospital and the referring hospitals. Among 422 patients with COPD, 17 patients had incomplete hospital records (missing of a minimum three important parameters), one patient with reported lung cancer, and seven patients with complicated asthma. Therefore, data from these (25 patients) were excluded from the study. Variables including BODE index score (primary objective), outcome measures, adverse effects, and clinical benefits (according to primary objective) for adopted treatments were extracted from hospital records for 397 patients with COPD. The flow chart of a retrospective study is presented in Fig. 1.Fig. 1. Flow diagram of retrospective analyses. The red color indicates worse parameters. The green color indicates comparatively better outcomes of treatments. COPD, Chronic obstructive pulmonary disease; GOLD, Global Initiative for Chronic Obstructive Lung Disease; BODE index, Body-mass index, airflow obstruction, dyspnea, and exercise capacity index (range 0–10, the higher the score worse the condition).Fig 1
Demographical and clinical characteristics
Male to female ratio was – . Patients were Han Chinese and 50 years or more years in age at the start of treatment. The distribution of patients according to GOLD categories was similar among cohorts. In addition, there were no statistical differences in the demographical and clinical characteristics before commencing pulmonary rehabilitation with inhaled pharmacological treatment for COPD among cohorts (Table 2).Table 2. Demographical and clinical characteristics before commencing pulmonary rehabilitation with inhaled pharmacological treatment for COPD.Table 2. CharacteristicsTotalCohortsComparisons among cohortPICEMEPulmonary rehabilitation‒Healthcare-professional at institutesSelf-driven at homeNoneNumbers of patients397115127155p-valueDfTest valueGenderMale260 (65)75 (65)80 (63)105 (68)0.7039 (ꭓ^2^ test for independence)20.7022Female137 (35)40 (35)47 (37)50 (32)Age (years)56 (60–54)55 (60–54)56 (60–54)58 (61–54)0.1037 (Kruskal-Wallis’ test)N/A4.532Inhaled pharmacological treatment according to GOLDGroup A62 (16)15 (13)15 (12)32 (21)0.131 (ꭓ^2^ test for independence)69.852Group B132 (33)45 (39)47 (37)40 (26)Group C115 (29)30 (26)40 (31)45 (29)Group D88 (22)25 (22)25 (20)38 (24)EthnicityHan Chinese367 (92)107 (93)118 (93)142 (92)0.9867 (ꭓ^2^ test for independence)60.3455Mongolian26 (7)7 (6)8 (6)11 (7)Tibetan4 (1)1 (1)1 (1)2 (1)Body mass index (kg/m^2^)25 (26–24)25 (26–24)25 (26–24)25 (26–24.5)0.1006 (Kruskal-Wallis’ test)N/A4.593FEV1 % predicted52 (54–51)52 (54–51)52 (54–51)52 (55–51)0.068 (Kruskal-Wallis’ test)N/A5.376mMRC3 (4–3)3(4–3)3(4–3)3(4–3)0.564 (Kruskal-Wallis’ test)N/A1.145Six minutes walking test (m)255 (261–249)257 (261–245)255 (268–248)257 (259–249)0.0736 (Kruskal-Wallis’ test)N/A5.219BODE index score5 (5–4)5 (5–4)5 (5–4)5 (5–4)0.2448 (Kruskal-Wallis’ test)N/A2.814Exacerbations in 6 months before commencement of treatments12 (13–12)12 (13–12)12 (13–12)12 (13–12)0.1741 (Kruskal-Wallis’ test)N/A3.496SmokingNo smoker370 (93)112 (97)119 (94)140 (90)0.0699 (ꭓ^2^ test for independence)25.409Previous smoker26 (7)3 (3)8 (6)15 (10)DrinkingNo drinking381 (96)108 (94)121 (95)153 (99)0.0984 (ꭓ^2^ test for independence)24.638Previous drinking15 (4)7 (6)6 (5)2 (1)Df, Degree of Freedom; COPD, Chronic Obstructive Pulmonary Disease; GOLD, Global Initiative for Chronic Obstructive Lung Disease; BODE index, Body-mass index, airflow obstruction, dyspnea (range 0–10, the higher the score worse the condition); mMRC, The modified Medical Research Council; N/A, Not Applicable.Non-normal continuous and categorical variables are depicted as median with Q3–Q1 in parenthesis and frequencies with percentages in parenthesis.Test value (ꭓ^2^-value for ꭓ^2^-test; Kruskal-Wallis’ statistics for Kruskal-Wallis’ test).All results were considered significant if the p-value was <0.05.
Before commencing inhaled pharmacological treatment with or without pulmonary rehabilitation for COPD patients had 5 (5–4) / patient BODE index score and 12 (13–12) / patient exacerbations (in 6 months) reported. The details of the BODE index score corresponding to individual parameters before commencing pulmonary rehabilitation with inhaled pharmacological treatment for COPD are reported in Table 3.Table 3BODE index score corresponding to individual parameters before commencing pulmonary rehabilitations with inhaled pharmacological treatment for COPD.Table 3. CharacteristicsTotalCohortsPICEMENumbers of patients397115127155Pulmonary rehabilitation‒Healthcare-professional at institutesSelf-driven at homeNoneBody mass index (kg/m^2^)0 (0–0)0 (0–0)0 (0–0)0 (0–0)FEV1 % predicted1 (1–1)1 (1–1)1 (1–1)1 (1–1)mMRC2 (3–2)2 (3–2)2 (3–2)2 (3–2)Six minutes walking test1 (2–1)1 (2–1)1 (2–1)1 (2–1)Variables are depicted as median with Q3–Q1 in parenthesis.BODE index, Body-mass index, airflow obstruction, dyspnea (range 0–10, the higher the score worse the condition); mMRC, The modified Medical Research Council.
Outcome measures
Six minutes walking test
After 6 months of inhaled pharmacological treatment for COPD with or without pulmonary rehabilitation six-minute walking test was improved across all the cohorts (p < 0.05 for all, Friedman test/Dann's multiple comparisons test). A six-minute walking test was better in the PI and CE cohorts than those of the ME cohort after 6 months of inhaled pharmacological treatment for COPD (p < 0.05 for all, Kruskal-Wallis’ test/Dann's multiple comparisons test). In addition, the six-minute walking test was better in the PI cohort than in the CE cohort after 6 months of inhaled pharmacological treatment for COPD (p < 0.05 for all, Kruskal-Wallis’ test/Dann's multiple comparisons test).
BODE index and exacerbations
BODE index score 6 months after commencing of pulmonary rehabilitation with inhaled pharmacological treatment for COPD and exacerbations during 6 months after commencing of pulmonary rehabilitation with inhaled pharmacological treatment for COPD were fewer for patients of the PI, CE, and ME cohorts as compared to before commencing of pulmonary rehabilitation with inhaled pharmacological treatment for COPD (p < 0.05 for all, Friedman test/Dann's multiple comparisons test). BODE index score 6-months after commencing of pulmonary rehabilitation with inhaled pharmacological treatment for COPD and exacerbations during 6 months after commencing of pulmonary rehabilitation with inhaled pharmacological treatment for COPD were fewer for patients of the PI cohort than those of patients of the CE and ME cohorts. BODE index score and exacerbations were statistically the same for patients of the CE and ME cohorts.
The details of the BODE index score corresponding to individual parameters 6 months after the commencement of pulmonary rehabilitation with inhaled pharmacological treatment for COPD are reported in Table 4. Treatment of COPD with or without pulmonary rehabilitation of 6 months reduced the BODE index score of patients of ME, PI, and CE cohorts were −25 (0–−25), −67 (−25–−67), and −25 (−25–−25), respectively. % Differences in BODE index score after 6 months of pulmonary rehabilitation with treatment of COPD in patients of PI were higher than those of patients of ME and CE cohorts (p < 0.0001 for both, Kruskal-Wallis’ statistics: 112, Kruskal-Wallis’ test). However, % differences in BODE index score after 6 months of pulmonary rehabilitation with the treatment of COPD in patients of the CE cohort were statistically similar to those of the ME cohort (p > 0.05, Kruskal-Wallis’ statistics: 112, Kruskal-Wallis’ test).Table 4BODE index score corresponding to individual parameters 6-months after commencing of pulmonary rehabilitation with inhaled pharmacological treatment for COPD.Table 4. CharacteristicsTotalCohortsPICEMENumbers of patients397115127155Pulmonary rehabilitation‒Healthcare-professional at institutesSelf-driven at homeNoneBody mass index (kg/m^2^)0 (0–0)0 (0–0)0 (0–0)0 (0–0)FEV1 % predicted1 (1–1)1 (1–1)1 (1–1)1 (1–1)mMRC1 (2–1)1 (2–1)2 (2–2)2 (2–2)Six minutes walking test1 (1–1)1 (1–1)1 (1–1)1 (1–1)Variables are depicted as median with Q3–Q1 in parenthesis.BODE index, Body-mass index, airflow obstruction, dyspnea (range 0–10, the higher the score worse the condition); mMRC, The modified Medical Research Council.
The details of outcome measures 6 months after the commencement of pulmonary rehabilitation with inhaled pharmacological treatment for COPD are reported in Table 5.Table 5. Outcome measures after and during 6-months after the commencement of pulmonary rehabilitation with inhaled pharmacological treatment for COPD.Table 5. ParametersCohortsComparisons between PI and CEMEPICEPulmonary rehabilitationNoneHealthcare-professional at institutesSelf-driven at homeNumbers of patients155115ap-valueTest value127ap-valueTest valuep-valueTest valueBODE index score4 (5–4)3 (4–3)<0.0011134 (4–4)>0.05113<0.001113Exacerbations12 (13–12)11 (12–10)<0.0019112 (12–12)>0.0591<0.00191Variables are depicted as median with Q3–Q1 in parenthesis.aConcerning ME cohort.Kruskal-Wallis’ test was used for statistical analysis. Dann's multiple comparisons test was used for post hoc analysis.All results were considered significant if the p-value was <0.05.BODE index, Body-mass index, airflow obstruction, dyspnea (range 0–10, the higher the score worse the condition).
The results of the assumptions tests are presented in Table 6.Table 6. Results of the assumption test.Table 6. VariablesStatical algorithm results for adopted testCategorial variablesFor 2 × 2 tablesFisher's exact test or Chi-Squared test (when the sample size is >40)For large contingency tablesChi-Squared test for independenceDemographical and clinical characteristicsAge (years)2 columns (p < 0.0001 & 0.0066) had not passed the normality test, i.e., Kruskal-Wallis’ test (nonparametric ANOVA)Body mass index (kg/ m^2^)3 columns (p = 0.0406; 0.0142; 0.0105) had not passed the normality test, i.e., Kruskal-Wallis’ testFEV1 % predicted (absolute value)3 columns (p = 0.0012; 0.0083; 0.0062) had not passed the normality test, i.e., Kruskal-Wallis’ testmMRC (absolute value) score3 columns (p < 0.0001 for all) had not passed the normality test, i.e., Kruskal-Wallis’ testSix minutes walking test (m)3 columns (p = 0.0021;<0.0001;<0.0001) had not passed the normality test, i.e., Kruskal-Wallis’ testOutcome measuresBODE index score before and 6-months after the commencement of pulmonary rehabilitation with inhaled pharmacological treatment for COPD within and between cohorts3 columns (p < 0.0001 for all) had not passed the normality test, i.e., Kruskal-Wallis’ test between cohorts and Friedman test withinExacerbations in 6-months before the commencement of treatments within and between cohorts3 columns (p < 0.0001 for all) had not passed the normality test, i.e., Kruskal-Wallis’ test between cohorts and Friedman test withinSix minutes walking test (m) 6-months after the commencement of pulmonary rehabilitation with inhaled pharmacological treatment for COPD within and between cohorts3 columns (p < 0.0001 for all) had not passed the normality test, i.e., Kruskal-Wallis’ test between cohorts and Friedman test withinExacerbations during 6-months after the commencing of pulmonary rehabilitation with inhaled pharmacological treatment for COPD within and between cohorts3 columns (p < 0.0001 for all) had not passed the normality test, i.e., Kruskal-Wallis’ test between cohorts and Friedman test withinCOPD, Chronic obstructive pulmonary disease; mMRC, The modified Medical Research Council; BODE index, Body-mass index, airflow obstruction, dyspnea, and exercise capacity index; ANOVA, Analysis of Variance.
Clinical benefits for inhaled pharmacological treatment (with or without pulmonary rehabilitation)
Clinical benefits for patients of PI, CE, and ME cohorts had 0–1, 0.29–0.8, and 0–0.55 beneficial scores for inhaled pharmacological treatment (with or without pulmonary rehabilitation), respectively. Patients of PI, CE, and ME cohorts had a risk of under treatment for <0.01 BODE index score, <1.32 BODE index score, and <3.14 BODE index score, respectively. Working areas for the current study population were 2–7 BODE index score, 2–7 BODE index score, and 3.14–7 BODE index score, respectively for Patients of PI, CE, and ME cohorts. The details of the clinical benefits of inhaled pharmacological treatment (with or without pulmonary rehabilitation) are presented in Table 7. The graphical presentation of the clinical benefits of inhaled pharmacological treatment (with or without pulmonary rehabilitation) for patients of different cohorts is presented in Fig. 2.Table 7. Clinical benefits for inhaled pharmacological treatment (with or without pulmonary rehabilitation).Table 7. ParametersCohortsPI cohortCE cohortME cohortPulmonary rehabilitationHealthcare-professional at institutesSelf-driven at homeNoneTotal number of patients115127155Patients with ≥ −10 % BODE index score differences115109106Patients with<−10 % BODE index score differences01849BODE index scoreBeneficial scores for patients0.011−140.73−315.1311−0.42−2.16210.29−0.58310.53−0.05410.650.21510.720.37610.760.47710.80.55810.820.60910.840.651010.860.68Clinical benefits (beneficial score)0–10.29–0.80–0.55Working area for the current study population2–7 BODE index score2–7 BODE index score3.14–7 BODE index scoreRisk of under-treatment< 0.01 BODE index score< 1.32 BODE index score< 3.14 BODE index scoreBODE index, Body-mass index, airflow obstruction, dyspnea, and exercise capacity index (range 0–10, the higher the score worse the condition).Fig. 2. The graphical presentation of clinical benefits of inhaled pharmacological treatment (with or without pulmonary rehabilitation) for patients of different cohorts. BODE index, Body-mass index, airflow obstruction, dyspnea, and exercise capacity index (range 0–10, the higher the score worse the condition).Fig 2
Adverse effects
Patients mainly suffered from headaches, nausea, skin rash, and shortness of breath during six months of inhaled pharmacological treatment for COPD with or without pulmonary rehabilitation. Adverse effects during 6 months of inhaled pharmacological treatment for COPD with or without pulmonary rehabilitations were comparable across all cohorts (p > 0.05 for all, Table 8). Beyond these adverse events, a few events were not noticed, for example, high heart rate, and body aches (because patients did not notice such adverse effects strongly; adverse effects were subjective).Table 8. Adverse effects during 6 months of inhaled pharmacological treatment for COPD with or without pulmonary rehabilitation.Table 8. EventCohortsComparisons between PI and CEMEPICEPulmonary rehabilitationNoneHealthcare-professional at institutesSelf-driven at homeNumbers of patients155115ap-valueTest value95 % CI127ap-valueTest value95 % CIp-valueTest value95 % CIHeadache5 (3)7 (5)0.37130.71670.364–1.4118 (6)0.26120.68970.3439–1.3830.99990.98090.5613–1.714Dizziness3 (2)5 (4)0.29170.64640.2626–1.5915 (4)0.47410.6760.2745–1.6640.99991.0550.5591–1.989Sore throat9 (6)7 (6)0.99990.97860.6271–1.5277 (6)0.99991.0250.6562–1.6000.99991.0560.6142–1.814Nausea10 (6)8 (7)0.99990.96550.6302–1.4798 (6)0.99991.0110.6596–1.5510.99991.0560.6348–1.757Upper respiratory infections4 (3)2 (2)0.99991.1660.6556–2.0721 (1)0.3831.4680.9345–2.3050.60561.410.6263–3.174Urinary tract infection2 (1)1 (1)0.99991.1630.5191–2.6071 (1)0.99991.2160.5422–2.7260.99991.0530.2615–4.237Cramps25 (16)20 (17)0.74230.94650.7132–1.25622 (17)0.74920.94560.7072–1.2640.99991.0030.7071–1.421Skin rash12 (8)10 (9)0.82420.9460.6365–1.4068 (6)0.81631.0990.7558–1.5990.62491.1850.7662–1.833Shortness of breath8 (5)6 (5)0.99990.99510.6245–1.5867 (6)0.99990.96870.5960–1.5750.99990.96970.5307–1.772Patients had one or more adverse events during the study period.Variables are depicted as frequencies with percentages in parentheses.aConcerning ME cohort.Fischer's exact test was used for statistical analysis.All results were considered significant if the p-value was <0.05.CI, Confidence interval (using the approximation of Katz.).Test value (relative risk for Fisher's exact test).
Discussions
Before commencing inhaled pharmacological treatment with or without pulmonary rehabilitation for COPD patients had 5 (5–4) / patient BODE index score and 12 (13–12)/ patient exacerbations (in 6 months) reported. In China, general practitioners are unable to understand COPD,16 and do not prescribe treatment as per GOLD guidelines.17 The lack of adequate knowledge and guidelines for treatments for COPD in China makes conditions worse for COPD patients. Chinese patients with COPD have worse clinical conditions.
The six-minute walking test, BODE index score, exacerbations during 6 months, clinical benefits for patients, and risk of undertreatment were better in the PI cohort than those of the CE and ME cohorts after 6 months of inhaled treatment. The results of outcome measures of the current study are consistent with those of randomized trials.3^,^10^,^12 Pulmonary rehabilitation at institutes improves lung capacity and six-minute walking test.3 Pulmonary rehabilitation at institutes improves the strength and force of the respiratory muscles.18 This leads to improved other outcome measures after 6 months of inhaled treatment with pulmonary rehabilitation. After 6 months of inhaled pharmacological treatment for COPD with pulmonary rehabilitations at institutes improves the clinical conditions of patients.
After 6 months of inhaled pharmacological treatment for COPD with or without pulmonary rehabilitation, a 6-minute walking test was improved and the BODE index score and exacerbations during 6 months were decreased across all the cohort. These results are consistent with those of a trial.3 This effect was due to inhaled pharmacological treatment as per GOLD 2019 guidelines. Chinese COPD patients are required to be treated as per proper guidelines.
The details of the comparative studies on pulmonary rehabilitation in COPD patients in different settings are presented in Table 9.Table 9. Comparative studies on pulmonary rehabilitation in COPD patients in different settings.Table 9. StudyPublished yearStudy populationSample size (n; patients)Age (years)Follow-upRandomized controlled trial, Cameron-Tucker, et al.32014Australian8465.8 ± 9.356-weeksMulticenter prospective observational study, Zeng, et al.72020Chinese479664.5 ± 8.91-yearSingle-blinded, randomized, controlled trial He, et al.102019Chinese21765.3 ± 6.220 weeksProspective study, Huivaniuk et al.122022Ukraine4064.86 ± 9.816-monthsObservational study, Kerti et al.182018Hungarian32764 ± 84-weeksMulticenter study, Sandoz et al.192017Austria141> 1812-year
The study shows novel advantages of pulmonary rehabilitation in COPD patients. The control group consists of the patients treated with traditional Chinese methods. Part of the conclusion is related to the results of the study. However, there are so many limitations of the study, for example, the conclusion is strictly related to Chinese populations. Retrospective medical records analyses only and lack of trial. Anxiety and depression are important parameters of patients with COPD who received treatment in follow-up.19 However, the current study has not evaluated the psychological aspects of patients.
Conclusions
Chinese patients with COPD have worse clinical conditions. After 6 months of inhaled pharmacological treatment for COPD with pulmonary rehabilitations at institutes improves the clinical conditions of patients. Chinese COPD patients are required to be treated as per proper guidelines.
List of submission
COPD, Chronic obstructive pulmonary disease; GOLD, Global Initiative for Chronic Obstructive Lung Disease; BODE index, Body-mass index, airflow obstruction, dyspnea, and exercise capacity index; mMRC, The modified Medical Research Council, SD, Standard deviation; ꭓ^2^-test, Chi-Square test; PI cohort, Patients of COPD received pulmonary rehabilitation under supervision of health-professional at institute + inhaled pharmacological treatment for COPD according to GOLD 2019; CE cohort, Patients of COPD received self-driven conventional exercise-based pulmonary rehabilitation at home + inhaled pharmacological treatment for COPD according to GOLD 2019; ME cohort, Patients of COPD did not receive any type of pulmonary rehabilitation at institute or at home except follow-up visits of consultants at 45 days + inhaled pharmacological treatment for COPD according to GOLD 2019; ANOVA, Analysis of variance; BT, Before commence inhaled pharmacological treatment with or without pulmonary rehabilitations; AT, After 6 months of inhaled pharmacological treatment for COPD with or without pulmonary rehabilitation.
Availability of data and materials
The datasets used and analyzed during the current study are available from the corresponding author upon reasonable request.
Authors’ contributions
All the authors have read and approved the manuscript for publication. GZ was the project administrator, and contributed to the supervision, resources, validation, and literature review of the study. JY contributed to the software, methodology, conceptualization, supervision, and literature review of the study. ZP contributed to the investigation, methodology, literature review, supervision, and software of the study. FX contributed to the methodology, resources, validation, supervision, and literature review of the study. RD contributed to the methodology, formal analysis, data curation, supervision, and literature review of the study. LB contributed to the methodology, literature review, resources, software, and data curation of the study. AL contributed to resources, methodology, formal analysis, methodology, software, visualization, and literature review of the study and drafted and edited the manuscript for intellectual content. All authors agree to be accountable for all aspects of the work, ensuring its integrity and accuracy.
Conflicts of interest
The authors declare that they have no conflicts of interest or any other competing interests regarding the results and/or discussion reported in the research.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Dong J Li Z Luo L Xie H Efficacy of pulmonary rehabilitation in improving the quality of life for patients with chronic obstructive pulmonary disease: evidence based on nineteen randomized controlled trials Int J Surg 73202078863184367710.1016/j.ijsu.2019.11.033 · doi ↗ · pubmed ↗
- 2Wouters EFM Wouters BBREF Augustin IML Houben-Wilke S Vanfleteren LEGW Franssen FME Personalised pulmonary rehabilitation in COPD Eur Respir Rev 2714720181810.1183/16000617.0125-2017 PMC 948856929592864 · doi ↗ · pubmed ↗
- 3Cameron-Tucker HL Wood-Baker R Owen C Joseph L Walters EH Chronic disease self-management and exercise in COPD as pulmonary rehabilitation: a randomized controlled trial Int J Chron Obstruct Pulmon Dis 920145135232487677110.2147/COPD.S 58478 PMC 4037329 · doi ↗ · pubmed ↗
- 4Troosters T Janssens W Demeyer H Rabinovich RA Pulmonary rehabilitation and physical interventions Eur Respir Rev 32168202311410.1183/16000617.0222-2022 PMC 1024514237286219 · doi ↗ · pubmed ↗
- 5Sun YC Chronic obstructive pulmonary disease in primary healthcare institutions in China: challenges and solutions Chronic Dis Transl Med 6420202192233333616710.1016/j.cdtm.2020.05.007PMC 7729120 · doi ↗ · pubmed ↗
- 6Pan F Lu AT Mao X Hu F Zhang H Han B Physicians' knowledge of pulmonary rehabilitation in China: a cross-sectional study Int J Chron Obstruct Pulmon Dis 1920241211313824982110.2147/COPD.S 429517 PMC 10799615 · doi ↗ · pubmed ↗
- 7Zeng Y Cai S Chen Y Duan J Zhao Y Li X Current status of the treatment of COPD in China: a multicenter prospective observational study Int J Chron Obstruct Pulmon Dis 152020322732373332404610.2147/COPD.S 274024 PMC 7732160 · doi ↗ · pubmed ↗
- 8Jenkins AR Cox NS Tappan RS Holland AE Rochester CL Alison JA Summary for clinicians: clinical practice guideline on pulmonary rehabilitation for adults with chronic respiratory disease Ann Am Thorac Soc 21420245335373824101610.1513/Annals ATS.202310-909CME · doi ↗ · pubmed ↗