Changes in hormone receptor when breast cancer metastasizes to the colon: case report and literature review
Huimeng Li, Liying Yang, Xiqiang Sun, Zhuquan Wang, Shuangwei Qin, Chengcheng Li, Gongwu Liu, Fengming Xie, Weiwei Gao

TL;DR
This paper reports a rare case of breast cancer metastasizing to the colon with changes in hormone receptors and reviews similar cases in the literature.
Contribution
The report adds a new case to the limited literature on breast cancer metastasis to the colon with hormone receptor changes.
Findings
A 65-year-old woman with breast cancer history was diagnosed with metastasis to the colon with altered hormone receptors.
The patient developed liver and systemic metastases within 19 months after initial treatment.
Only a few cases of breast cancer metastasis to the colon with receptor changes have been previously documented.
Abstract
The metastasis of breast cancer to the colon is a rare occurrence, especially in the presence of changes in estrogen and progesterone receptors. To date, literature has only reported two cases of invasive ductal carcinoma and two cases of invasive lobular carcinoma metastasizing to the colon with concurrent changes in hormone receptors. This report describes a 65-year-old woman with a history of left breast cancer, who presented with symptoms of bloody stools and abdominal pain. CT and colonoscopy results revealed a malignant tumor in the ascending colon, and the patient underwent surgery. Pathological results post-surgery indicated changes in hormone receptors, differing from the previous breast cancer pathology, ultimately leading to the diagnosis of breast cancer metastasis to the colon. The patient was found to have liver metastasis 14 months after right hemicolectomy, and systemic…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
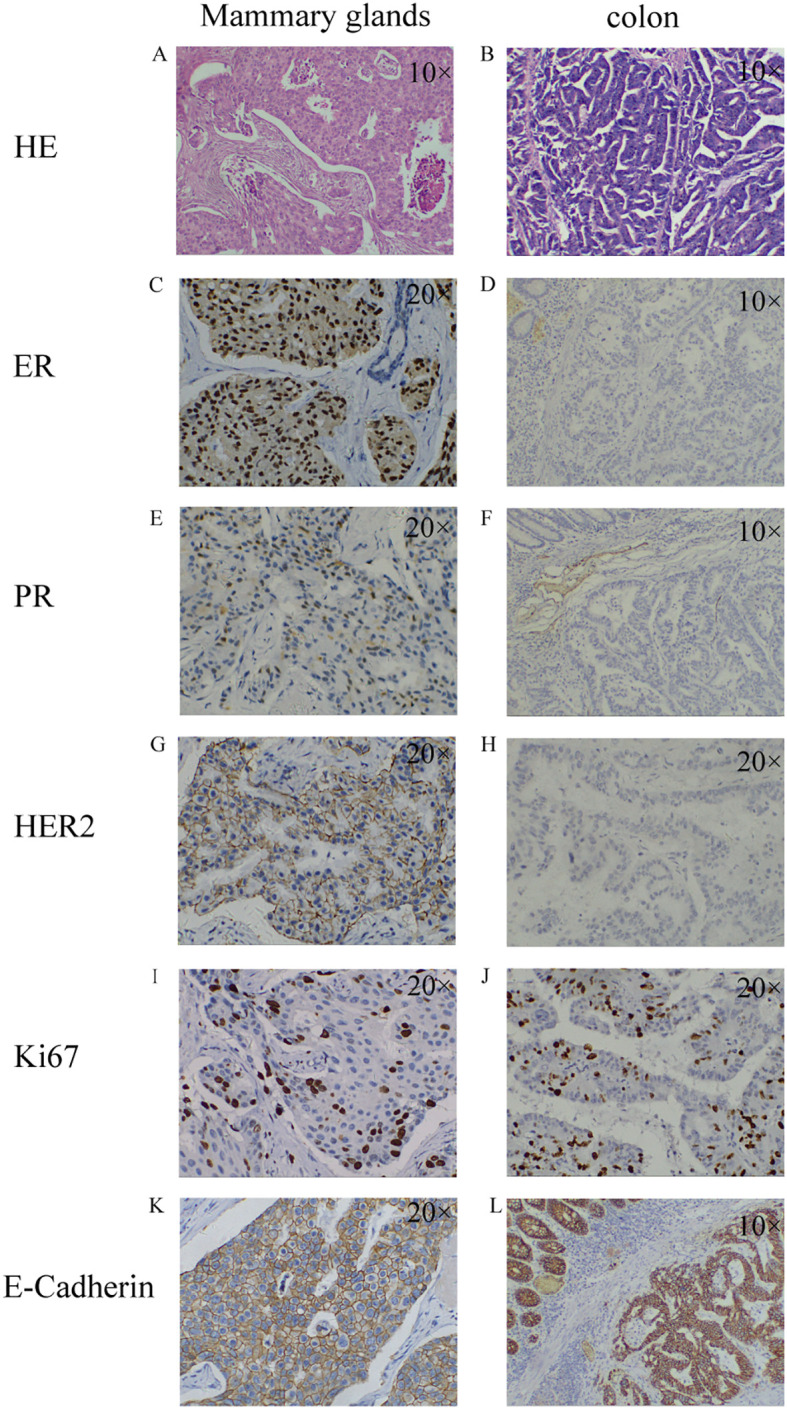 Figure 1
Figure 1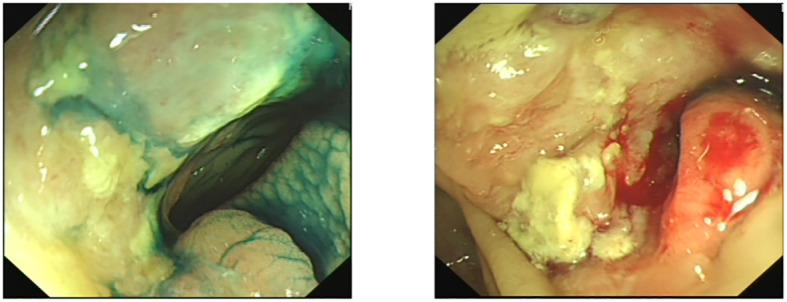 Figure 2
Figure 2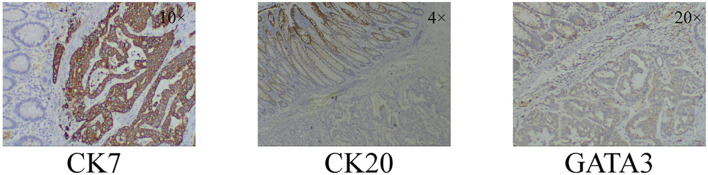 Figure 3
Figure 3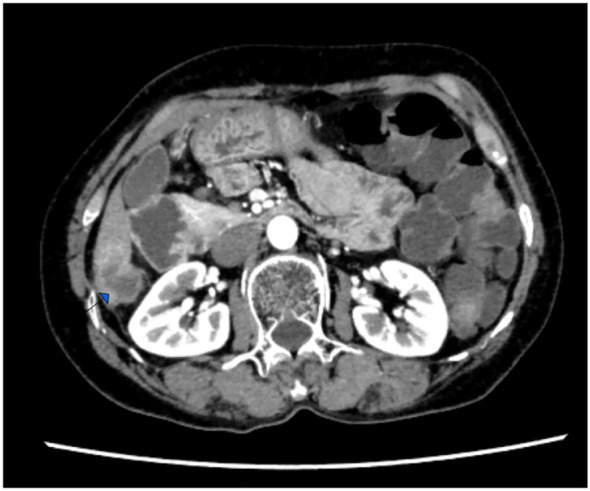 Figure 4
Figure 4 Figure 5
Figure 5| Author | Year | Age | Primary(breast) | Treatment | Time since first diagnosis (years) | Metastasis | |||
|---|---|---|---|---|---|---|---|---|---|
| Site | Pathological types | Biomarkers | Site | Biomarkers | |||||
| Takeuchi H ( | 2012 | 38 | left | ILC | ER+,PR-,HER2- | Surgery, Chemotherapy, Radiation therapy, Endocrine Therapy | 3 | Stomach and Colon | ER+,PR-, HER2- |
| Jansen van Rensburg A ( | 2021 | 74 | left | DC | ER+,PR- | Surgery, Radiation therapy, Endocrine Therapy | 27 | Bone,ovary, sigmoid colon | ER +, PR+ |
| Sheen-Chen SM ( | 2008 | 41 | right | IDC | – | – | Simultaneous | ovary and omentum | - |
| Higley C ( | 2020 | 74 | right | – | – | breast-conserving surgery and radiation therapy, Endocrine Therapy | 40 | transverse colon. | ER-、PR-、HER2- |
| Khan I ( | 2017 | 56 | right | ring cell adenocarcinoma | – | – | Simultaneous | stomach, small intestine, and | – |
| Noor A ( | 2020 | 68 | – | ILC | ER+,PR+,HER2- | Surgery, Radiation therapy, Endocrine Therapy | 30 | Bone、sigmoid colon | ER+、PR+、HER2-,CK7+, CK20-,CDX2-,CA19-9- |
| Bering J ( | 2020 | 67 | left | ILC | ER+,PR+,HER2- | Endocrine Therapy | Simultaneous | transverse colon | ER-,PR-,HER2+ |
| Abid A ( | 2013 | 59 | left | LC | ER+,PR+,HER2- | – | Simultaneous | stomach, duodenum, and colon | ER+、PR+ |
| Takedomi H ( | 2019 | 76 | right | ILC | – | Chemotherapy | Simultaneous | descending colon | - |
| Abu Zaanona MI ( | 2020 | 73 | – | – | – | Endocrine Therapy | – | colon | ER+,PR-,HER2-,Pancytokeratin+, GATA3 +, E-cadherin-, CDX2-, |
| Inoue H ( | 2022 | 63 | right | Chemotherapy,Endocrine Therapy | 15 | ER+,PR-,HER2+,CK7+, GATA3+, ER+, HER2+, CK20-, PR-, E-cadherin-, GCDFP15- ,caudal-related homeobox 2 | |||
| Mostafa A ( | 2002 | 56 | – | IDC | ER+,PR+ | Surgery, Radiation therapy, Endocrine Therapy | 5 | descending colon | ER-,PR-- |
| Tsujimura K ( | 2017 | 51 | left | ILC | ER+,PR+ | – | Simultaneous | ileocecal | ER+,PR+,HER2- |
| Feng CL ( | 2009 | 49 | right | IDC | – | – | 2 | Colon | CK7+, CK20- |
| Kobayashi M ( | 2020 | 74 | – | ILC | – | surgery | 23 | stomach | CAM5.2+,ER+, E-cadherin- |
| Théraux J ( | 2008 | 69 | bilateral | IDC | – | Surgery, Endocrine Therapy | 28 | transverse colon | ER+,PR+, HER2-, CK7+, CK20- |
| Malhotra A ( | 2009 | 71 | – | – | – | – | – | bone, transverse colon | – |
| Villa Guzmán JC ( | 2017 | 58 | – | ILC | ER+,PR+,HER2- | Surgery, Chemotherapy, Radiation therapy, Endocrine Therapy | 3 | stomach | cytokeratin-19+,ER+ |
| Gerova VA ( | 2012 | 56 | left | ILC | PR+ | Surgery, Chemotherapy, Radiation therapy, Endocrine Therapy | 5 | stenotic, stomach | – |
| 42 | left | – | ER+,PR+ | Surgery, Chemotherapy, Radiation therapy, Endocrine Therapy | 7 | stomach | ER+,PR+,CK7+, E-cadherin+,S-100+, GCFP15-,CDX2- | ||
| Wang G ( | 2014 | 70 | left | IDC | E-cadherin+、34βE12-、ER+、PR+、CK19+、CK20+ | Surgery, Radiation therapy, Endocrine Therapy | 10 | ascending colon | CK7+、E-cadherin+、34βE12-、ER+、GCDFP-15+、CK19+、CK20+ |
| Cho DH ( | 2011 | 46 | bilateral | IDC | ER+,PR+,HER2- | Surgery, Chemotherapy, Radiation therapy, Endocrine Therapy | 2 | terminal | ER+,PR-,HER2+, |
| Algethami NE ( | 2022 | 47 | bilateral | ILC | ER+,PR+,HER2- | Surgery, Radiation therapy, Endocrine Therapy | 4 | rectum | ER+、HER2+、Pan-cytokeratin + |
| Zhou XC ( | 2012 | 54 | right | IDC | ER+,PR+,P53+, | Surgery, Chemotherapy, Radiation therapy, Endocrine Therapy | 8 | sigmoid colon | CDX2-, Villin-, TTF-1-, -CK20-, HER2-, ER- ,PR-, |
| Andriola V ( | 2014 | 63 | left | IDC,LC | – | Surgery, Chemotherapy, Radiation therapy, Endocrine Therapy | 23 | colon and terminal | CK19+, GCFDP-15+,HER2+ |
| Motos-Micó J ( | 2014 | 69 | right | ILC | – | Surgery, Chemotherapy | 18 | sigmoid colon | ER-,PR-,HER2-,CK7+ |
| Abdallah H ( | 2020 | 59 | right | ILC | ER+,PR+,HER2- | – | Simultaneous | endometrium, myometrium, fibroid and cervix | CK7+,GATA3+,ER+,PR+, desmin-, CD10-, actin- ,Caldesmon- |
| 66 | right | ILC | CK+,ER+,PR+,HER2- | – | Simultaneous | Colon | CK7+,GATA-3+,ER+,CK20-,CDX2- | ||
| 53 | right | ILC | – | – | Simultaneous | intestine, omentum, and peritoneal wall, bilateral ovarian, stomach | CK7+、GATA-3+,ER+,E-cadherin+,CK20-,CDX2- | ||
| Michalopoulos A ( | 2004 | 55 | left | IDC | – | Surgery, Chemotherapy | 4 | transverse | CK7+,milk-fat globule protein+, |
| 57 | left | ILC | – | Surgery, Chemotherapy, Radiation therapy | 10 | transverse | CK7+,milk-fat globule protein+, CEA+,ER+, weakly positive for cytokeratin 20 and Breast II. | ||
| Schellenberg AE ( | 2018 | 69 | left | IDC | E-cadherin+,ER+,PR+,HER2+ | Surgery, Chemotherapy, Radiation therapy, Endocrine Therapy | 2 | rectosigmoid | CK-7+, E-cadherin+, GCDFP+, mammoglobin+,ER+,PR+,CK-20-,CDX-2-- |
| Matsuda I ( | 2012 | 62 | left | ILC | – | Surgery | 24 | ascending colon and rectum | CK7+,ER+,CK20-,E-cadherin- |
| Koleilat I ( | 2010 | 54 | right | IDC | – | Surgery, Chemotherapy, Radiation therapy, Endocrine Therapy | 13 | colon | ER+,PR+,HER2- |
| Mistrangelo M ( | 2011 | 80 | left | ILC | – | Surgery, Endocrine Therapy | 25 | sigmoid colon | – |
| Razzetta F ( | 2011 | 77 | bilateral | ILC(left),IDC(right) | – | – | Simultaneous | right, transverse and left colon | ER+,PR- |
| Cervi G ( | 2001 | 59 | – | ILC | – | Surgery | 8 | rectum | ER+,PR+ |
| Amin AA ( | 2011 | 61 | right | ILC | – | Surgery, Endocrine Therapy | 17 | rectum | CK 20-,ER+,CK7+,PR+ |
| López Deogracias M ( | 2009 | 67 | left | ILC | ER+,PR+ | Surgery | 15 | rectum | ER-,PR-,CK20-,CDX2- |
| Law WL ( | 2003 | 49 | left | IDC | ER+ | Surgery, Endocrine Therapy | 5 | descending | ER+ |
| Samra B ( | 2019 | 64 | – | – | – | – | – | colon,right sacral iliac | CK-7+,GATA-3+,ER+,MOC31+,CK-20-,CD-X2-,PR-,PAX-8-,SOX-10-,CD4-5,chromogranin-, synaptophysin-, TTF-1- |
| Kim HW ( | 2014 | 46 | right | metaplastic | ER-,PR-,HER2- | Surgery, Chemotherapy, Radiation therapy | 2 | sigmoid colon | CK20-,CK5/6-,ER-,PR-,HER2-,CK7+ |
| Signorelli C ( | 2005 | 62 | right | ILC | – | Surgery | 12 | right chest wall, colon | ER+,PR+,P53-,HER2- |
| Gizzi G ( | 2015 | 72 | – | – | ER+,PR+ | Surgery, Chemotherapy, Radiation therapy, Endocrine Therapy | 11 | sigmoid colon | CK7+,GATA3+, ER+,PR+,HER2- |
| Dhar S ( | 2003 | 75 | left | – | ER+ | Surgery | 6 | sigmoid colon | ER+,CK7+,CK20- |
| Maekawa H ( | 2012 | 52 | right | IDC | ER+,PR+ | Surgery, Chemotherapy, Radiation therapy, Endocrine Therapy | 16 | ascending colon | – |
| Koufopoulos N ( | 2018 | 87 | – | – | – | – | – | Colonic serosa | CK-20-,CDX-2-,CK7-,r GATA-3+, mammaglogin+,ER+,PR+, E-cadherin-, Chromogranin-,synaptophysin- |
| Critchley AC ( | 2011 | 62 | – | IDC | – | Surgery, Chemotherapy, Radiation therapy, Endocrine Therapy | 8 | stomach, ascending colon | ER+,PR+,HER2-,CK7+,CK20- |
| Kachi A ( | 2019 | 58 | left | ILC | – | Surgery, Chemotherapy, Radiation therapy, Endocrine Therapy | 6 | sigmoid colon, appendix, and ovaries. | ER+,PR+ |
| Blachman-Braun R ( | 2018 | 73 | bilateral | – | – | Surgery, Chemotherapy, | 15 | colon | ER+,PR-,HER2- |
| Jia J ( | 2023 | 67 | right | IDC | ER+,PR+,HER2- | Surgery, Chemotherapy, Endocrine Therapy | 10 | Appendix, colon | GATA-3+,GCDFP-15+,ER+,PR+,HER2+, E-cadherin+,p120+,CK7+,CK20-,SATB-2-,Villin-,syn-,CgA-,CD56- |
| Arif FZ ( | 2023 | 65 | bilateral | IDC | triple-negative (left), HER2+(right) | – | – | descending colon | – |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMetastasis and carcinoma case studies · Cancer Diagnosis and Treatment · Cancer and Skin Lesions
Introduction
Breast cancer is the most common malignant tumor in women. Recurrence and distant metastasis often pose challenges in treatment. Common sites of metastasis include bones, liver, and lungs, while gastrointestinal metastases are extremely rare. Previous reports have shown that the pattern of metastasis differs between lobular carcinoma and ductal carcinoma of the breast. Gastrointestinal, gynecologic, and peritoneal metastases are more common in lobular carcinoma (1, 2). ILC (invasive lobular carcinoma) has an increased tendency to metastasize to the GI (gastrointestinal) tract compared with breast carcinomas of NST (non-special type) (40% vs. 2%) (3). We report a case of infiltrating ductal carcinoma that metastasized to the ascending colon, with changes in estrogen receptor (ER), progesterone receptor (PR), and human epidermal growth factor receptor-2 (HER2) status. To our knowledge, there have been only two similar cases reported previously.
Case presentation
A 65-year-old woman presented to our center with intermittent abdominal pain and hematochezia for several months. She had a previous diagnosis of ER- and PR-positive (Figure 1), HER2 ++ (no further testing was done) invasive ductal carcinoma of the left breast 5 years before. She underwent modified radical mastectomy for breast cancer. The pathological examination did not indicate the presence of axillary lymph node metastasis and received chemotherapy with anthracycline and cyclophosphamide, followed by taxanes. Subsequently, she received 5 years of endocrine therapy with letrozole until she presented to our center. The patient denied having smoked or consumed alcohol in the past.
Pathological findings of breast malignancy and colon malignancy. breast malignancy: HE staining (A); ER+ (C); PR+ (E); HER2+ (G); Ki67 15%+ (I); E-Cadherin+ (K); colon malignancy: HE staining (B); ER- (D); PR- (F); HER2- (H); Ki67 50%+ (J); E-Cadherin+ (L). HE staining: Hematoxylin-Eosin staining; ER: estrogen receptor; PR: progesterone receptor; HER2: human epidermal growth factor receptor-2; Ki67: nuclear-associated antigen Ki67.
During colonoscopy, a mass was found in the ascending colon (Figure 2). Biopsy results confirmed metastasis of breast cancer to the colon, which was negative for ER, PR, and HER2. However, no local lesions or enlarged lymph nodes were detected in the contralateral breast, chest wall, or axilla through ultrasound, magnetic resonance imaging, and clinical palpation.
Colonoscopy revealed a mass of ascending colon.
After receiving a transfusion of six units of red blood cells to correct anemia, the patient underwent a right hemicolectomy. Intraoperatively, it was observed that the tumor had invaded the right renal fascia. Two lymph node metastases were found on pathological examination after palliative surgery for colonic malignancy. The postoperative pathological examination confirmed the colonoscopy biopsy findings. Further immunohistochemical staining revealed positive results for Cytokeratin 7 (CK7), negative results for Cytokeratin 20 (CK20), and positive results for GATA 3 binding protein (GATA3) and E-Cadherin (Figure 3).
Immunohistochemical staining results of colonic malignancies. CK7+, CK20-, GATA3+. CK7: Cytokeratin 7; CK20: Cytokeratin 20; GATA3: GATA 3 binding protein.
Considering the rarity of this case, we sought opinions from pathologists in different centers to confirm the diagnosis. After considering the majority of expert opinions, it was confirmed as breast cancer metastasis to the colon. The patient was prescribed oral capecitabine at a dosage of 650-mg/m^2^ twice daily for chemotherapy treatment.
Follow-up imaging studies performed 6 months after the operation did not show any tumor metastasis or recurrence. However, the patient discontinued medication due to severe hand–foot syndrome. In a 14-month postoperative computed tomography (CT) scan, a solitary nodule was detected in the liver, indicating a metastatic lesion (Figure 4). The patient refused intravenous chemotherapy and opted for a second course of oral capecitabine treatment. Nineteen months after surgery, multiple metastases were discovered, including the liver, abdominal lymph nodes, adrenal glands, thoracolumbar spine, lungs, and mediastinal lymph nodes, accompanied by widespread cancer-related pain. The patient declined medication treatment. During the entire follow-up, no local recurrence of breast malignancy or new tumors of the opposite breast were found. The patient was lost to follow-up at 20 months after right hemicolectomy. Treatment and follow-up are organized into a timeline (Figure 5).
Computedtomography (CT) scan, a solitary nodule was detected in the liver, indicating a metastatic lesion.
Timeline depicting the treatment and follow-up of the patient.
Discussion
Breast cancer metastases to the gastrointestinal tract is extremely rare. Previous reports have shown that the most common sites of metastases in breast cancer are the bones, lungs, liver, and brain, while gastrointestinal metastases, especially to the colon, is very rare. The incidence of breast cancer metastases to the gastrointestinal tract, particularly to the colon, is estimated to be around 1%, with a rate of approximately 0.1% specifically for metastases to the colon (4). The patterns of metastases differ between lobular carcinoma and ductal carcinoma of the breast, with gastrointestinal metastases being more common in lobular carcinoma (1, 2). In this case, it was the ductal carcinoma of the breast that had colon metastases.
Due to the final diagnosis of breast cancer metastasis to the colon with receptor changes, this case presents significant challenges in terms of diagnosis and treatment. We performed a search in the PubMed database and gathered relevant literature, as detailed in Table 1. Our findings reveal the fourth documented case of ductal carcinoma of breast metastasizing to the colon, accompanied by changes in receptor status. Additionally, there have been two cases where receptor changes were observed when lobular carcinoma metastasized to the colon (5, 6).
In this case, there was a mismatch between the receptors in the primary breast lesion and the colon metastases. Incompatible receptors between the primary and secondary lesions of breast cancer have been reported, with frequencies of alterations in ER, PR, and HER2 being approximately 16.4%–32.4%, 30.9%–37.78%, and 10.2%–14.5%, respectively (7–10). Emilia Montagna reported in 2017 that approximately 82% of breast cancer metastases in the gastrointestinal tract have positive hormone receptor expression (11). In the dozens of case reports we have collected, the majority of patients were found to be hormone receptor positive. Among these patients, most did not exhibit any changes in the hormone receptor status. Previous reports have indicated that the instability of hormone receptors in breast cancer is associated with a poorer prognosis (12, 13), Women whose ER-positive primary tumors transform into ER-negative tumors experience a significant 48% increase in the risk of death (7). In this case report, liver metastases were found at 14 months after surgery, and multiple metastases throughout the body were found at 19 months with subsequent rapid disease progression.
CK7, CK20, and GATA3 are commonly used in pathology for tumor diagnosis and classification. These markers can provide information about the type and origin of the tumor. CK7 was expressed in 89%–98% of non-specified breast cancers (14). Most gastrointestinal, pancreaticobiliary, and ovarian mucinous adenocarcinomas are CK20 positivity, in adenocarcinoma, positivity of CK20 strongly indicates a non-breast origin, and CK7−/CK20+ immunoprofile strongly suggests colorectal origin (15). Based on previous research reports, CK7+/CK20 should be considered indicative of a tumor originating from the breast. GATA3 is also thought to be often positive in primary breast disease (16, 17). It was based on the immunohistochemical staining results of CK7 positive, CK20 negative, and GATA3 positive, combined with the opinions of multicenter pathologists, showing that the case was finally diagnosed as breast cancer with colon metastasis. Even though this case is very rare, we should still pay attention to the occurrence of colon metastasis in the diagnosis and treatment of breast cancer.
Conclusions
This case serves as a reminder to clinicians that they should consider rare sites of metastases and different receptor expression patterns in breast cancer patients in order to make more accurate treatment decisions. However, further research is needed to explore the mechanisms of this metastatic pattern and related treatment strategies.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Borst MJ Ingold JA. Metastatic patterns of invasive lobular versus invasive ductal carcinoma of the breast. Surgery. (1993) 114:637–41; discussion 641-2.8211676 · pubmed ↗
- 2Kennecke H Yerushalmi R Woods R Cheang MC Voduc D Speers CH. Metastatic behavior of breast cancer subtypes. J Clin Oncol. (2010) 28:3271–7. doi: 10.1200/JCO.2009.25.9820 20498394 · doi ↗ · pubmed ↗
- 3Kioleoglou Z Georgaki E Koufopoulos N Kostek O Volakakis N Dimitriadou A. Gastrointestinal metastases from lobular breast carcinoma: A literature review. Cureus. (2024) 16:e 65852. doi: 10.7759/cureus.65852 39219935 PMC 11364151 · doi ↗ · pubmed ↗
- 4Takedomi H Akutagawa T Sakata Y. Colon metastasis of breast cancer with a unique endoscopic finding. Clin Gastroenterol Hepatol. (2020) 18:e 74. doi: 10.1016/j.cgh.2019.04.014 30978537 · doi ↗ · pubmed ↗
- 5Bering J Ryan M Gurudu SR. Breast cancer metastasis presenting as colonic polyps. ACG Case Rep J. (2020) 7:e 00411. doi: 10.14309/crj.0000000000000411 33062785 PMC 7535760 · doi ↗ · pubmed ↗
- 6López Deogracias M Flores Jaime L Arias-Camisón I Zamacola I Murillo Guibert J Suescun García R. Rectal metastasis from lobular breast carcinoma 15 years after primary diagnosis. Clin Transl Oncol. (2010) 12:150–3. doi: 10.1007/S 12094-010-0481-0 20156785 · doi ↗ · pubmed ↗
- 7Lindström LS Karlsson E Wilking UM Johansson U Hartman J Lidbrink EK. Clinically used breast cancer markers such as estrogen receptor, progesterone receptor, and human epidermal growth factor receptor 2 are unstable throughout tumor progression. J Clin Oncol. (2012) 30:2601–8. doi: 10.1200/JCO.2011.37.2482 22711854 · doi ↗ · pubmed ↗
- 8Matsumoto A Jinno H Murata T Seki T Takahashi M Hayashida T. Prognostic implications of receptor discordance between primary and recurrent breast cancer. Int J Clin Oncol. (2015) 20:701–8. doi: 10.1007/s 10147-014-0759-2 25348193 · doi ↗ · pubmed ↗