Case report: a rare case of diffusely metastatic BRAF V600E-mutated colorectal cancer with concomitant infiltration of the skin and parotid gland
Aristeidis E. Boukouris, Ioannis Kokkinakis, Elias Drakos, Maria Sfakianaki, Maria Tzardi, Dimitrios Mavroudis, John Souglakos

TL;DR
This case report describes a rare and aggressive form of colorectal cancer with BRAF V600E mutation that spread to the skin and parotid gland.
Contribution
The first documented case of BRAF V600E-mutated CRC with simultaneous skin and parotid gland metastases.
Findings
The patient had BRAF V600E-mutated CRC that metastasized to uncommon sites like the skin and parotid gland.
This case highlights the aggressive and unpredictable nature of BRAF V600E-mutated CRC in the metastatic setting.
It is the second reported case of CRC with concomitant skin and parotid gland infiltration.
Abstract
Metastastic disease affects up to 50% of colorectal cancer (CRC) patients and is associated with particularly poor outcomes in the presence of the BRAF V600E mutation. Herein, we report a patient with initial diagnosis of stage IIIc CRC, who presented during follow-up (adjuvant phase) with dysphagia, left-sided lagophthalmos and multiple skin nodules. The ensuing work-up revealed disseminated metastatic disease from the primary CRC, which was BRAF V600E-mutated (retrospective tissue analysis), affecting, besides the lungs, multiple uncommon sites, such as the skin and parotid gland. The patient’s rapid disease progression did not allow for any therapeutic interventions. This is only the second report of concomitant metastatic infiltration of the skin and parotid gland by CRC, and the first with a documented molecular background of BRAF V600E mutation. BRAF V600E-mutated CRC can follow…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
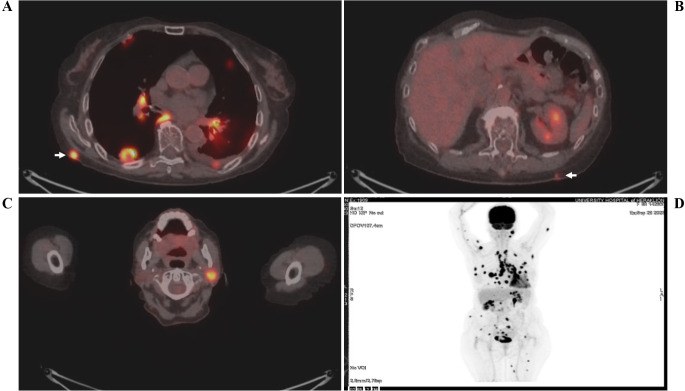 Figure 1
Figure 1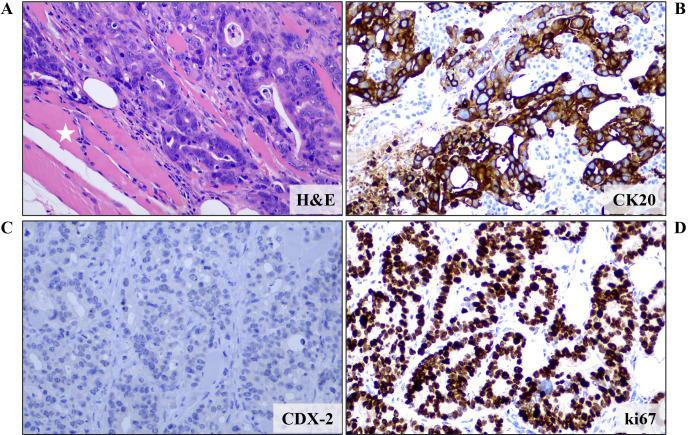 Figure 2
Figure 2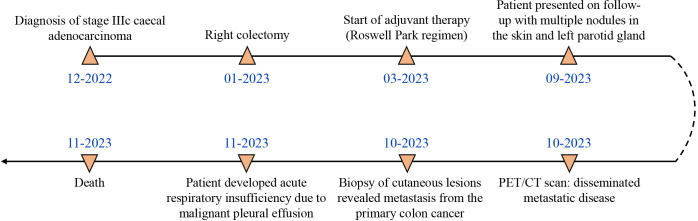 Figure 3
Figure 3- —University of Crete 10.13039/501100004429
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCancer Diagnosis and Treatment · Colorectal Cancer Treatments and Studies · Colorectal and Anal Carcinomas
Introduction
1
Colorectal cancer is the 4^th^ most common cancer worldwide and represents the 2^nd^ leading cause of cancer-related mortality (1). As many as 50% of CRC patients eventually go on to develop metastatic disease (de novo or secondary), predominantly affecting the liver, lung and peritoneum (in order of frequency). The BRAF V600E mutation (representing 95% of all CRC-related BRAF mutations) is only encountered in about 8% of metastatic CRC (mCRC) patients (2, 3), however it is associated with poor prognosis and a highly aggressive behavior, including resistance to currently available therapies and predilection for metastasis to distant lymph nodes and the peritoneum (4, 5). In this report, we describe a rare case of BRAF V600E-mutated CRC with secondary metastatic disease concomitantly affecting the skin and parotid gland.
Case presentation
2
An 83-year-old female patient (birthplace and residence: Crete, Greece) and former smoker (50 pack-years) with a past medical history of arterial hypertension and a family history of a first-degree relative with CRC at an advanced age, was recently diagnosed with stage IIIc (pT3N1b) caecal adenocarcinoma. Following right colectomy, the patient was placed on adjuvant therapy based on the Roswell Park regimen. After uneventful completion of the first cycle, the second cycle was interrupted midway due to GI disturbances and the patient feeling unwell. She presented to the outpatient clinic two months later due to intractable fatigue, along with dysphagia and left-sided lagophthalmos of recent onset. Clinical examination confirmed the dysphagia and revealed left-sided Bell’s palsy. Intriguingly, multiple firm nodules were noted on the trunk and extremities, along with a palpable firm nodule at the anatomic position of the left parotid gland. Routine complete blood count and basic metabolic panel did not reveal any abnormalities. However, the tumor marker CEA was significantly increased since it was last measured (8,1 ng/ml vs. < 1,73 ng/ml), raising suspicion of disease progression. Further investigation with ^18^F-FDG-PET/CT scan revealed hypermetabolic foci in the skin and left parotid gland (potentially accounting for the observed Bell’s palsy) (Figure 1), as well as multiple other sites (lung, bones, muscles, peritoneum and multiple lymph nodes (cervical, mediastinal, portal)). Molecular analysis of the archival primary tumor tissue revealed the presence of the BRAF V600E mutation. Biopsies of the skin lesions revealed infiltration by a low-grade enteric type adenocarcinoma, consistent with the morphologic characteristics of the primary tumor (Figure 2A-C). The metastatic origin of the lesions was further confirmed by detection of the BRAF V600E mutation via genetic testing. Notably, metastatic cancer cells exhibited an extremely high proliferation rate (ki67 positivity: 95%) (Figure 2D).
18F-FDG-PET/CT scan showing hypermetabolic uptake in the (A, B) skin (white arrows) and (C) left parotid gland. A whole-body scan (D) is also shown. The patient’s name and date of birth have been omitted for confidentiality reasons.
Microscopic examination of a biopsy from a skin lesion revealed infiltration of fat and striated muscle tissue (white asterisk) from an enteric type adenocarcinoma (tubular and cribriform pattern) (A) (H&E staining). Immunohistochemical analysis showed that the neoplastic cells expressed (B) CK20 but not (C) CDX-2, CK7 and TTF-1 (data not shown for CK7 and TTF-1). These features, combined with the patient’s history, were more compatible with a metastatic colorectal carcinoma. (D) Proliferation rate, as expressed by ki67 positivity, was almost 100%. Images are shown at 200x magnification. DAB as chromogen and hematoxylin as counterstain. CK, Cytokeratin; H&E, Hematoxylin and Eosin.
A few days after admission, the patient developed acute, severe respiratory insufficiency requiring high oxygen supply (Venturi mask). Besides signs of aspiration pneumonia, repeat chest X-ray revealed a diffuse opacification of the left hemithorax, consistent with a new, massive left-sided pleural effusion. Cytologic analysis of the fluid was positive for the presence of malignant epithelial cells. Despite fluid drainage and other supportive measures, the patient rapidly deteriorated, eventually succumbing to her disease.
The timeline of events and case progression with relevant data are presented in Figure 3.
Timeline of events and case progression.
Discussion
3
We present a patient with recently diagnosed stage IIIc CRC who relapsed with fulminant metastatic disease affecting many organs, among others the skin and parotid gland. Molecular analysis of the archival tumor tissue revealed the presence of the BRAF V600E mutation. No HER2 amplification and KRAS (exon 2, 3 and 4) mutations were detected. Testing of the MSI status, using PCR-based fragment analysis, was negative for microsatellite instability (20-30% of BRAF V600E-mutated CRCs are dMMR (6)). Presence of the BRAF V600E mutation represented the dominant oncogenic driver, accounting for the aggressive behavior of the disease. Consistent with the very high proliferation rate of the metastatic cancer cells and the multi-organ involvement, our patient’s condition and performance status rapidly deteriorated, precluding any therapeutic manipulations.
Our group has previously described the clinical aspects of the BRAF V600E mutation in CRC, which has been correlated with rapidly progressive multimetastatic disease, poor performance status, advanced age, peritoneal disease and low probability of secondary metastasectomy (7). Furthermore, a later Danish population-based study in 448 CRC patients (of which 30 carried the BRAF V600E mutation), associated the presence of the BRAF V600E mutation with increased risk of skin metastases (8). Our case confirms these observations and is the first to describe concomitant malignant infiltration of both the skin and parotid gland from CRC with documented BRAF V600E mutation. The rarity of similar cases, together with the lack of complete molecular characterization of the (primary or metastatic) tumor specimens (9) preclude potential identification of more specific clinical features of patients with BRAF V600E-mutated CRC who eventually develop metastatic infiltration of the skin and parotid gland.
The molecular basis behind the predilection of BRAF V600E-mutated CRC cells for invasion of the skin (and other unusual sites, such as the parotid gland), remains elusive. Of note, enrichment of the BRAF V600E mutation in cutaneous metastatic disease has also been documented for other types of cancer (lung cancer, papillary thyroid carcinoma), which only rarely affect the skin (10, 11). This suggests the possibility of a common underlying mechanism in BRAF V600E-mutated cells, perhaps related to downstream activation of hypoxia-inducible factors (HIFs) (12–14), which allows survival of metastatic cells in the mildly hypoxic skin microenvironment (15).
We also propose that assessment of the BRAF V600E mutation should be considered at the time of diagnosis, regardless of disease stage, since it may modify the treatment intent (palliative or curative) and influence the treatment strategy. Our approach is supported by a recent Italian expert opinion statement, which supports BRAF mutation testing not only in the metastatic setting but also in high-risk stage III CRC patients (16). This is because knowledge of the BRAF status and the prognostic significance of BRAF mutations could inform physicians about the strong possibility of early (adjuvant) treatment failure, as previously demonstrated in several cohorts (17, 18). Moreover, in case of disease recurrence, it could facilitate rapid-decision making and initiation of the appropriate treatment modality. As a matter of fact, targeted anti-BRAF agents have now largely replaced chemotherapy-based regimens for the treatment of BRAF V600E-mutated mCRC. Very recently, encorafenib (a BRAF V600 inhibitor) and cetuximab (an anti-EGFR monoclonal antibody), in combination with mFOLFOX6, received accelerated FDA approval in the 1^st^ line treatment of BRAF V600E-mutated mCRC based on the phase III BREAKWATER trial. Updated results of this trial are expected within the next few weeks, and they may change the standard of care in the 1^st^ line treatment. In the 2^nd^ line, mCRC patients with the BRAF V600E mutation can be effectively treated with the combination of encorafenib and cetuximab (19). Real-world data have confirmed the efficacy of this regimen (objective response rate, ORR: 32%) (20). Other combination regimens, such as dabrafenib (a selective BRAF inhibitor) and trametinib (a selective MEK inhibitor) have also been formerly tested, however with poorer outcomes (ORR: 12%).
In conclusion, our rare case confirms the aggressive phenotype conferred to CRC by the BRAF V600E mutation, and highlights the potential of this CRC subtype for concomitant metastatic infiltration of many non-classical target sites. Oncologists handling such patients should be aware of the unpredictable and potentially fulminant metastatic behavior of BRAF V600E-mutated CRCs, and that testing for BRAF V600E at the time of diagnosis may offer the opportunity for effective treatment earlier during the course of the disease, thus optimizing patients’ management.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Siegel RL Miller KD Wagle NS Jemal A . Cancer statistics, 2023. CA Cancer J Clin. (2023) 73:17–48. doi: 10.3322/caac.21763 36633525 · doi ↗ · pubmed ↗
- 2Saridaki Z Papadatos-Pastos D Tzardi M Mavroudis D Bairaktari E Arvanity H . BRAF mutations, microsatellite instability status and cyclin D 1 expression predict metastatic colorectal patients’ outcome. Br J Cancer. (2010) 102:1762–8. doi: 10.1038/sj.bjc.6605694 PMC 288369820485284 · doi ↗ · pubmed ↗
- 3Souglakos J Philips J Wang R Marwah S Silver M Tzardi M . Prognostic and predictive value of common mutations for treatment response and survival in patients with metastatic colorectal cancer. Br J Cancer. (2009) 101:465–72. doi: 10.1038/sj.bjc.6605164 PMC 272023219603024 · doi ↗ · pubmed ↗
- 4Tabernero J Ros J Élez E . The evolving treatment landscape in BRAF-V 600E–mutated metastatic colorectal cancer. Am Soc Clin Oncol Educ Book. (2022) 42):254–63. doi: 10.1200/EDBK_349561 35503983 · doi ↗ · pubmed ↗
- 5Zhi J Jia XJ Yan J Wang HC Feng B Xing HY . BRAF(V 600E) mutant colorectal cancer cells mediate local immunosuppressive microenvironment through exosomal long noncoding RN As. World J Gastrointest Oncol. (2021) 13:2129–48. doi: 10.4251/wjgo.v 13.i 12.2129 PMC 871333135070047 · doi ↗ · pubmed ↗
- 6Piercey O Tie J Hollande F Wong HL Mariadason J Desai J . BRAF(V 600E)-mutant metastatic colorectal cancer: current evidence, future directions, and research priorities. Clin Colorectal Cancer. (2024) 23:215–29. doi: 10.1016/j.clcc.2024.04.004 38816264 · doi ↗ · pubmed ↗
- 7Saridaki Z Tzardi M Sfakianaki M Papadaki C Voutsina A Kalykaki A . BRAFV 600E mutation analysis in patients with metastatic colorectal cancer (m CRC) in daily clinical practice: correlations with clinical characteristics, and its impact on patients’ outcome. Plo S One. (2013) 8:e 84604. doi: 10.1371/journal.pone.0084604 24367680 PMC 3867547 · doi ↗ · pubmed ↗
- 8Christensen TD Palshof JA Larsen FO Poulsen TS Hogdall E Pfeiffer P . Associations between primary tumor RAS, BRAF and PIK 3CA mutation status and metastatic site in patients with chemo-resistant metastatic colorectal cancer. Acta Oncol. (2018) 57:1057–62. doi: 10.1080/0284186 X.2018.1433322 29380640 · doi ↗ · pubmed ↗