Brainwave Activity Localization, Mood Symptoms, and Balance Impairment in a Male South African Rugby Player With Persisting Symptoms After Concussion: A Case Report
M. J. Lumb, N. Snegireva, A. M. Coetzee, K. E. Welman

TL;DR
This case report explores the use of mobile EEG and balance testing to monitor recovery in a rugby player with lingering concussion symptoms.
Contribution
The study introduces a clinical protocol integrating mobile EEG, balance testing, and mood screening for post-concussion recovery monitoring.
Findings
Mobile EEG and qEEG techniques can detect residual brainwave activity deficits after concussion.
Instrumental balance testing reveals impairments not captured in standard exams.
Mood symptom screening is essential for comprehensive post-concussion care.
Abstract
The case sets the foundation for clinical protocols to incorporate mobile EEG and qEEG techniques, instrumental balance testing, and mood symptom screening in athletes who have suffered a sports‐related concussion. The protocol provides a framework for clinicians to monitor a patient's recovery progress in terms of brainwave activity, general cognition, moods, and motor control. Objective data obtained through the protocol may assist in developing personalized treatment plans, improving follow‐up care, and identifying residual brain function deficits that may be missed in standardized clinical exams. Finally, this case highlights a need for more thorough communication and testing procedures that screen for mood symptoms and provide an opportunity for athletes to discuss their mental health after suffering from an SRC.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
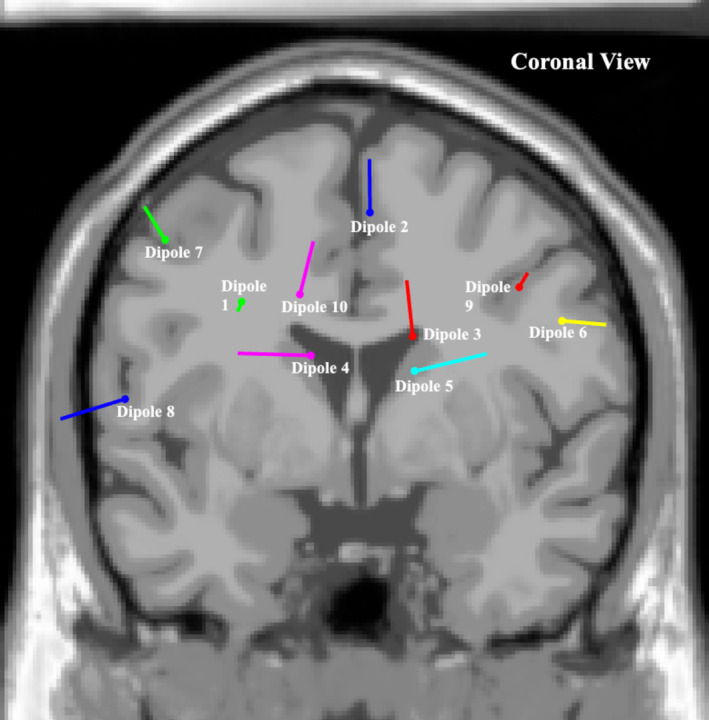 FIGURE 1
FIGURE 1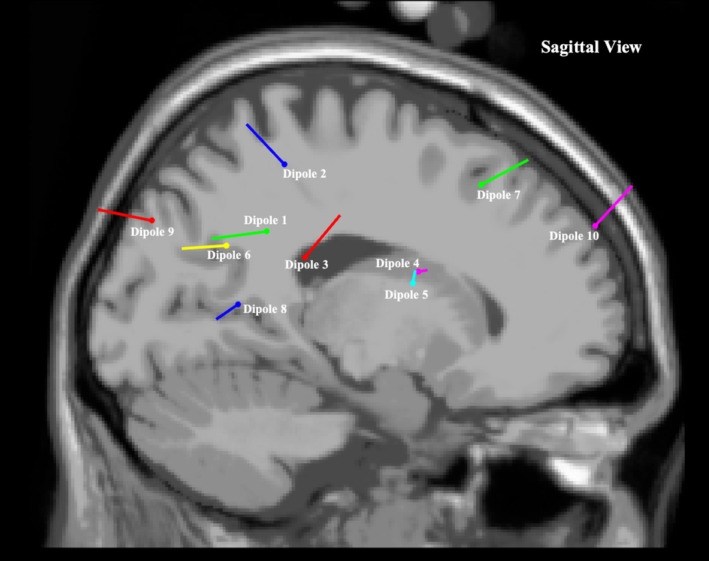 FIGURE 2
FIGURE 2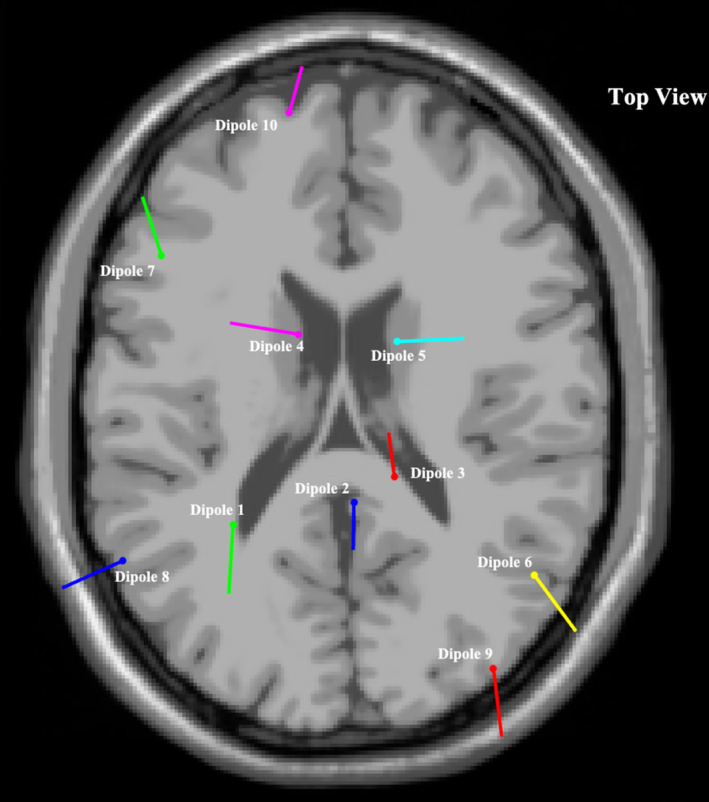 FIGURE 3
FIGURE 3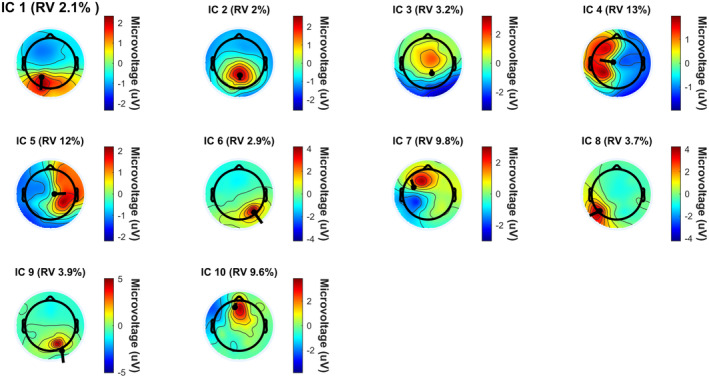 FIGURE 4
FIGURE 4| Participant medical history/screening tool | Score/descriptors | Interpretation |
|---|---|---|
| MoCA (A.U) | 26 | Typical cognitive function |
| ImPACT (A.U) | 5 | The participant scored on the following criteria: (1) Nervous/Anxious (1), (2) Difficulty concentrating (1), (3) Difficulty remembering (1), (4) Visual problems (2). The scale is scored on a 0–6 scale, with 0 being none and 6 being severe |
| PHQ‐9 (A.U) | 5 (Scored 0 on question 9) |
Mild depressive mood severity with no suicidal or self‐harm tendencies/thoughts. Question 9 refers to suicidal and self‐harm tendencies. If a patient scores on this question, it requires an immediate referral for further diagnosis The following was scored on: (1) Little interest or pleasure in doing things (several days), (2) Feeling down, depressed, or hopeless (several days), (3) Trouble falling asleep or staying asleep, or sleeping too much (several days), (4) Feeling tired or having little energy (several days), (6) Feeling bad about yourself‐or that you are a failure or have let yourself or your family down (several days) |
| GAD‐7 (A.U) | 5 |
Mild anxiety moods The following was scored on: (1) Feeling nervous, anxious, or on edge (several days), (2) Not being able to stop or control worrying (several days), (3) Worrying too much about different things (over half the days), (6) Becoming easily annoyed or irritable (several days) |
| FSS (A.U) | 44 | Suggests that fatigue has a high level of impact |
| ESS (A.U) | 5 | Suggests that the patient may not be suffering with excessive daytime sleepiness |
| Weekly alcohol consumption | ± 7 units a week | |
| Alcohol consumption 24 h before testing | 1.2 units | 10 mL/8 g of pure alcohol or 25 mL of whiskey or equivalent. The participant indicated he had a beer 24 h prior to testing. Low levels of alcohol consumption are generally metabolized within several hours after consumption [ |
| Learning disabilities/ADHD | No | |
| Hearing aids or pacemaker | No | |
| Previous neuromusculoskeletal injury | Grade 2 hamstring strain (unspecified), right. February 2023. | |
| Prescribed medication to assist with mood symptom management | Yes (unspecified) | The pharmacological prescription was for the continued mood symptoms experienced |
| Component/Dipole # | Closest brain region in Desikan–Killiany Atlas | Talairach co‐ordinates (X,Y,Z) | Residual variance (%) | General brain region's functions |
|---|---|---|---|---|
| 1 | Inferior parietal left | −29;−44;32 | 2.06% | Associated with spatial attention, sensory integration, and oculomotor control [ |
| 2 | Superior parietal right | 3;−37;52 | 1.95% | Integral to visual, motor, cognitive, sensory, higher order cognition, working memory and attention processes [ |
| 3 | Superior parietal right | 13;−32;23 | 3.22% | |
| 4 | Pre‐central left | −12;4;17 | 12.69% | Associated with voluntary motor control patterns [ |
| 5 | Post‐central right | 14;2;14 | 12.49% | Contains the primary somatosensory cortex and is responsible for the integration of proprioception [ |
| 6 | Inferior parietal right | 50;−57;28 | 2.92% | Associated with spatial attention, sensory integration, and oculomotor control [ |
| 7 | Caudal middle‐frontal left | −47;25;42 | 9.79% | Plays a significant role in the development of literacy, and the process of reorientation to unexpected stimuli [ |
| 8 | Lateral occipital left | −57;−54;10 | 3.66% | Contributes vastly to visual image processing and visual image communication with the cerebral cortex [ |
| 9 | Lateral occipital right | 39;−80;37 | 3.89% | |
| 10 | Superior frontal left | −14;61;28 | 9.64% | Key component in the neural network of working memory and spatial processing [ |
| Subjective Score, Mean ± SD (A.U) [ | ||||
|---|---|---|---|---|
| Stance/Measure | Firm surface error norm (A.U) | Foam error surface norm (A.U) | Participant average error firm (A.U) | Participant average error foam (A.U) |
| Double leg stance feet together | 0.03 ± 0.26 | 0.13 ± 0.56 | 0 | 0 |
| Single leg stance non‐dominant foot | 2.50 ± 2.21 | 6.24 ± 2.36 | 0.33 ± 0.58 | 3.33 ± 0.58 |
| Tandem stance | 0.72 ± 1.15 | 2.90 ± 2.40 | 0 | 0 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsTraumatic Brain Injury Research · Cardiac Arrest and Resuscitation · Psychosomatic Disorders and Their Treatments
Introduction
1
Persisting symptoms after concussion (PSaC) is a complex pathophysiological process that refers to individuals who do not recover within the typical time frame after concussion [1]. Most concussive symptoms tend to peak hours after injury and gradually improve over days [1]. However, it has been suggested that clinical symptoms contradict physiological recovery and pathological developments may persist [1, 2, 3, 4, 5]. This can be in the form of irregular electrical brainwave activity, metabolic imbalance, reduced oxygen consumption, and reduced cerebral blood flow, resulting in the potential increase in the risk of re‐injury, psychological disorders, musculoskeletal injuries, or the development of chronic traumatic encephalopathy (CTE) [6, 7]. Such persisting symptoms have been suggested to present in 10%–30% of people, depending on the specific population cohort and the time frames used to define it [8, 9, 10].
Currently, mental health outcomes in athletes who experience PSaC are unclear and require further detailed investigation [11]. The prevalence of anxiety and depression in elite male athletes participating in team sports is nearly 45% [12]. Repetitive sports‐related concussions (SRC) are thought to increase the risk of the development of mental health problems, cognitive impairment, and sensorimotor disruption [13]. Persisting symptoms after concussion have been associated with higher levels of disability and psychological distress [10]. In addition to this, associations between persisting symptoms and depressive moods have been established; however, the causal directionality of the association is still up for debate [10]. Further focus on mental health screening and identifying replicable biomarkers associated with PSaC may lead to better athlete care and management, reducing the risk of re‐injury and further pathological developments, especially in the form of mental health degradation [10].
Postural stability is a complex motor skill that incorporates the integration and processing of dynamic sensorimotor information, and sports‐related concussions are believed to result in the dysfunction of sensorimotor integration caused by disrupted neural connections and axonal shearing [14]. Due to this neural trauma, PSaC may present, resulting in impaired motor outputs and an increased risk of suffering further concussions and other injuries, potentially also resulting in increased mood‐related symptoms [14].
It has also been found that emotions can affect motor behavior and that they are important indicators of mental illness [15]. Postural stability reflects multiple levels of the nervous system functioning together [15, 16]. These systems develop simultaneously with the development of higher‐level brain structures, including the prefrontal cortex, basal ganglia, and cerebellum [15]. It is thought that gait and postural discrepancies reflect impaired function of the cortical and subcortical regions [15]. Since psychiatric variables, gait, and postural stability function within these higher‐level brain structures, one can suspect that mood disorders such as depression and anxiety may have a direct impact on the capacity of the musculoskeletal system to adjust to stimuli; therefore, potentially justifying further research to establish if correlations exist between all three variables [15, 16].
A noteworthy consideration for practitioners treating in a sporting environment is to consider that multiple concussions may cause cumulative impact on balance, mood disorders, and long‐term cognition due to the direct physical neuronal trauma sustained during high‐impact head collisions. This trauma can result in the impairment of the sensorimotor integration process, leading to prolonged symptomology such as mood disorders and motor control dysregulation. Studies have shown that more than one concussion increases the risk of the individual experiencing PSaC, including balance impairment, mood disorders, cognitive decline, and a higher risk of the development of chronic traumatic encephalopathy (CTE) [17, 18].
Strides are being made to identify a replicable biomarker through the use of electroencephalography (EEG) data in combination with advanced mathematical software‐assisted analysis (qEEG) to determine sources of irregular brainwave functionality as well as provide evidence of brain injury in athletes with PSaC [19, 20, 21, 22, 23]. In addition to this, instrumented postural sway techniques are being explored to potentially detect more subtle deviations in postural stability within the population. These subtle deviations generally go missed in subjectively scored tests such as the standard Balance Error Scoring System (BESS) [24, 25].
This article describes the case of an active 21‐year‐old male professional rugby player who had suffered multiple concussions and was presenting with PSaC along with mood symptoms (depressive moods and anxiety‐like symptom) and fatigue symptoms. He underwent neurological and mood disorder screening as well as EEG testing while performing instrumented postural tasks. The case highlights a potential need for detailed and continued screening of mood symptoms in the population. Furthermore, it highlights the potential need to discover a replicable biomarker to determine regions of the brain that are most impacted as well as to determine a cost‐effective replicable instrumental balance test to detect subtle deviations in postural stability.
Case History
2
The participant was a 21‐year‐old male professional rugby player who played in the position of flank. He weighed 104.5 kg and was 190 cm tall. At the time of testing, he had been involved with professional rugby for 3 years and had suffered four confirmed diagnosed concussions, with the last one occurring approximately 13 months prior to the date of testing. The mechanism of injury involved direct contact to the right side of the head just above the ear (i.e., temporal bone). The participant was on the defending side when the injury occurred. Initial impact occurred when the participant launched himself in for a tackle and the ball carrier stepped into him, catching his head with his knee. The mechanism of injury was detailed from the participant's perspective. After the latest concussion, the participant was advised not to partake in contact sport for ± 6 months while he underwent cognitive and physical rehabilitation in the form of memory and balance training. Rehabilitation was completed, and at the time of testing, he was actively partaking in competition. The participant expressed concerns for his future health and indicated that it was unlikely that he would continue rugby after the completion of his studies due to the fear that further injury may occur.
Further descriptive and medical history details can be found in Table 1.
Case Examination Procedure and Results
2.1
Descriptive data were collected using a variety of questionnaires (Table 1). Additionally, a 64‐lead mobile EEG recording was conducted simultaneously with an instrumented BESS test [2, 27]. The case report was written using the Consensus‐based Clinical Case Reporting (CARE) guidelines checklist where applicable [28].
A medical history questionnaire was implemented to build a comprehensive background of the participant. This was followed by the Epworth Sleepiness Scale (ESS), the Fatigue Severity Scale (FSS), The Patient Health 9‐item Questionnaire (PHQ‐9), the Generalized Anxiety Disorder 7‐item Questionnaire (GAD‐7), the ImPACT Post‐Concussion Symptom Scale, and the Montreal Cognitive Assessment (MoCA) version 8.3.
Quantitative balance readings were collected utilizing the APDM Mobility Lab System (Opal, APDM Inc. Portland, OR) with a wearable body sensor attached around the participants lumbar region, L5 vertebrae as reference [25, 29].
The EEG reading was conducted using a compact wireless EEG amplifier and recorder (LiveAmp 64, Brain Products GmbH, Gilching, Germany) combined with a 64‐channel spandex (ActiCAP) active fitted electrode cap (ActiCAP, Brain Products GmbH, Gilching, Germany). The electrodes were positioned using the international 10–20 system [30, 31]. Recording was conducted at a sampling rate of 500 Hz with impedance set at 25 k‐Ω (kΩ) [32]. Electroencephalogram (EEG) data were obtained using the BrainVision Recorder (Brainvision Recorder, Vers. 1.23.001, Brain Products GmbH, Gilching, Germany).
Baseline EEG measurements were collected prior to testing to identify how specific movement artifacts may emerge. These baselines included: (1) 60 s natural stance, relaxed state, eyes closed, no counting or rhythmic activity, (2) 60 s natural stance, relaxed state, eyes open, no counting or rhythmic activity, (3) 30 s jaw clench, (4) 30 s continuously blinking, (5) 30 s head nodding, (6) 30 s head turning, (7) 30 s single leg balance with non‐dominant foot tapping, (8) 30 s lifting hands on and off iliac crests, (9) 30 s rocking back and forth on feet (i.e., between forefoot and heel).
The two 60 s standing still with eyes closed and eyes open baselines were performed and utilized as reference for the balance tasks in the BESS during data analysis. The 30‐s tasks were used to identify similar deviations in the recording during the BESS which may present as artifacts.
The BESS test was performed three times. Each test consisted of six trials taking place on a firm surface and on a medium‐density balance pad. Each trial was 20 s in duration, with rest periods between each stance. All stances were performed eyes closed. Subjective errors and objective center of pressure (CoP) measurements were also recorded and compared to normative data (Table 3) [29, 33]. Each BESS trial was completed in a systematic order: i.e., (1) double stance firm, (2) single stance firm (non‐dominant leg), (3) tandem stance firm (non‐dominant leg behind), (4) double stance foam surface, (5) single stance foam (non‐dominant leg), (6) tandem stance foam (non‐dominant leg behind). EEG data was collected continuously throughout the 3 testing trials, with time between stances and trials removed during the analysis to create a continuous EEG recording.
The BESS was chosen as it is a valid, reliable, cost‐effective and commonly used tool in concussion management, and it forms part of the SCAT6 assessment protocol [4]. However, several limitations exist namely the subjective scoring, learning effects and reduced sensitivity in detecting long‐term balance issues in persisting symptoms after concussion [24, 27]. Additional quantitative measurements in the form of a lumbar spine accelerometer to assess postural sway and potentially capture more subtle deviations in postural stability. Studies have shown that instrumented assessments of balance can detect subtle impairment and imbalances that persist beyond what can be seen visually [24]. The combination of the already established BESS and portable accelerometer used may provide a cost‐effective testing protocol for the use in PSaC in sports outside of relying on laboratory‐based procedures which are often costly. Other alternatives include computerized dynamic pictography, tandem gait testing with dual tasking and sensory organization testing.
The EEG data obtained from BrainVision Recorder were analyzed using MATLAB Version R2023b and the EEGLAB toolbox v2023.1.
A processing pipeline was developed by consulting previous studies that shared similarities and through tutorial presentations provided by the Swartz Centre for Computational Neuroscience, Institute for Neural Computation, University of California San Diego [19, 21, 23, 34] (Appendix A).
The most significant dipole locations that met inclusion criteria are depicted in Figures 1, 2, 3, with corresponding brain locations and coordinates presented in Table 2. Figure 4 displays the topographical scalp maps of each individual component analyzed, with the corresponding dipole location. Table 3 details subjective and objective BESS results.
Coronal view of most significant dipole locations superimposed on an averaged referenced MRI.
Sagittal view of most significant dipole locations superimposed on an averaged referenced MRI.
Top view of most significant dipole superimposed on an averaged referenced MRI.
Topographical scalp maps of each identified individual component (IC) and Their corresponding dipole. The following topographical scalp maps visualize the distribution of electrical activity across the skull. The accompanying dipole represents the source localization of where suspected brainwave activity originated and the direction it traveled. Residual variance percentages (RV%) are also provided, indicating the error between the model's predicted brain activity and the actual recorded brain activity. A low RV% indicates that the model implemented explains the observed brainwave activity with a high level of confidence.
Discussion, and Conclusion
3
Discussion
3.1
The current case set out to highlight the potential long‐term presentations of mood disorders that may present in rugby players with PSaC and have a history of SRC. Furthermore, it reports on areas of neuronal activity in the brain of the patient while performing balance tasks that were subjectively and objectively measured. Additionally, it presents a template that can be further developed to screen for mood‐related symptoms for the athlete as well as provide a safe opportunity for the athlete to communicate freely on how they feel.
This study incorporated screening for mood disorders in assessing PSaC, since trauma to the brain may have longer lasting effects in the form of anxiety and depressive symptoms, which in return may cause increased disruptions to postural stability and neuronal activity bidirectionally [15, 16].
Therefore, it was hypothesized that a complex multidirectional relationship exists between these variables, and it is believed that the findings from such a protocol would add to a better understanding of the brain–body connection related to balance and mood. These results may lead to the development of brain activity biomarkers, a detailed screening protocol for mood‐related disorders, and a quantitative postural stability test for diagnostic and prognostic purposes in a clinical environment for this population and possibly for others.
It is also worth noting that in this case the participant suffered multiple concussions that may have resulted in cumulative damage to the brain impacting balance, mood disorders, and long‐term cognition. This continuous trauma can result in the impairment of the sensorimotor integration process leading to prolonged symptomology such as mood disorders and motor control dysregulation [17, 18]. Studies have shown that more than one concussion increases the risk of the individual experiencing persisting symptoms including balance impairment, mood disorders, cognitive decline, and a higher risk of the development of chronic traumatic encephalopathy (CTE) [17, 18].
The novelty of this case lies in the fact that the EEG recording was collected during instrumented balance tasks and not during resting states [21]. Athletes require a complex brain–body connection to perform optimally at the highest level; therefore, ideally, the testing should mimic the systems that are involved during complex motor control tasks performed while playing sports. Postural sway testing is also used as a diagnostic course prediction tool for individuals with mood disorders and as a return‐toto‐play test in SRC, most noticeably in the SCAT6 [2].
Brain Regions Associated With Sport‐Related Concussions and Persisting Symptoms
3.1.1
Sports‐related concussion research has indicated that the frontal lobes, anterior cingulate, cerebellum, and the parietal lobes are the most affected brain regions, similarly presenting in the current case (dipole 1, 2, 3, 6, 7, 10) (Table 2) [20, 43]. Furthermore, it has been suggested that diffuse axonal injury may occur in the hippocampus, resulting in long‐range communication deficits between it and other brain regions such as the prefrontal cortex and the amygdala [44]. These long‐range communication deficits have been found to persist after clinical symptoms have subsided, displaying abnormalities within central and primary white matter structures [45].
The current case displayed similar regions of neuronal activity when compared to previous studies, most noticeably in the left superior frontal cortical region (i.e., dipole 10) (Table 2) [21]. This brain region is thought to contribute most to higher cognitive functions such as working memory [46]. A previous study that utilized a form of ICA decomposition processing to clean EEG data and transform scalp sensory readings into brain sources found increased beta band power and decreased delta and theta band power in the frontal cortex in the concussed group [21]. This mirrors findings in previous fMRI studies showing changes in functional connectivity within frontal regions of the brain as well as findings in this case study where significant neuronal activity was found in the pre‐central left region (i.e., dipole 4), left superior frontal region (i.e., dipole 7) and the left middle frontal region (i.e., dipole10) [45].
It has been theorized that the above‐mentioned affected region, cognitive impairment, and slower neuronal processing speeds of stimuli in the brain are consequences of axonal injury, changes in neurotransmission, and irregularity in glycolysis homeostasis [44]. This may be due to the mechanism of injury associated with SRCs, namely, direct biomechanical contact forces or inertial forces leading to significant acceleration, deceleration, and/or rotational forces applied to these brain regions [4, 22, 44, 47].
Mood Disorders Such as Depression and Anxiety in Persisting Symptoms After Concussion as Well as Brain Regions Associated With Mood Disorders
3.1.2
Although associations between mental health variables such as depression and anxiety have been suggested, the findings remain inconclusive, requiring further investigation possibly due to limited understanding [11, 48]. The importance of athlete mental health is rising due to the generic and sport‐specific stressors athletes are exposed to as well as the potential commonality between damaged regions of the brain due to the SRC and those associated with mood‐related symptoms [49, 50]. Experts have indicated that it is necessary for practitioners to recognize these symptoms early through thorough screening and implement graded exercise as well as education and counseling for the athlete [48].
The participants scores on the PHQ‐9, GAD‐7, and ImPACT (Table 1) align with current literature that indicates a bidirectional association between mood symptoms and individuals experiencing PSaC exist with those presenting with PSaC being at a higher risk of experiencing depressive and anxiety‐based symptoms, up to 10 years' post‐injury [10]. It is also worth noting that several other variables have been associated with the risk of developing PSaC, such as age (adolescents to young adults have been suggested to be at higher risk), the female sex, the mental health history of the athlete, and the number of SRCs suffered [10]. These are future areas that should be focused on by researchers in the context of SRCs and PSaC.
With regards to qEEG findings, the participant also presented with similar regions of neuronal activity when compared to previous studies that explored abnormalities in task‐related brain activation in patients with mood and anxiety disorders (i.e., dipole 1, 4, 6, and 10) (Table 2) [41, 51].
These studies had found hypoactivity in the frontal regions of the cortex, more specifically in the inferior prefrontal cortex/insula, the inferior parietal lobules, and the putamen, reducing engagement in inhibitory control and salience processing which could potentially impact motor control through the impairment of attention, awareness, sensory information integration, and executive functioning processes [51]. Hyperactivity had also been detected in the cingulate, amygdala, parahippocampal, and thalamus cortical regions suggesting over‐engagement of the regions of the brain associated with emotional regulation. Over‐allocation of neural resources to these may impact an individual's neural capacity to communicate and process stimuli impacting the bottom‐up (sensory‐driven) and top‐down (cognitive‐driven) neural communication mechanisms [51, 52].
Individuals with depressive moods have also displayed reduced function in the occipital lobes due to possible reductions and imbalances of neurotransmitters [41]. Similar brain regions in the participants were observed to be active, including dipole 8 and 9 (Table 2). Thus, this is a region of interest to compare to a group presenting with minimal to no mood disorders.
Postural Control and Persisting Symptoms After Concussion as Well as Brain Regions Associated With Balance
3.1.3
This case did not present with subjective or objective balance scores outside of identified normative data (Table 3) [29, 33]. This may be due to greater motor control capacity in professional athletes resulting in fewer subjective errors and lower sway variations presenting during the BESS protocol. In addition, the results may have been impacted due to the participant having undergone physical rehabilitation treatment for the persisting symptoms and having already returned to play, potentially resulting in above‐average motor control capacity.
The current case did, however, present similarly to previous neural imaging studies that explored brain regions associated with balance and postural control, with regions of activity presenting in the frontal, parietal, and occipital brain regions (i.e., dipole 1–10) (Table 2) [53]. Nearly every region in the brain is thought to be involved in balance, with the cerebellum playing a pivotal role [53]. Previous studies also pointed to subcortical regions, namely the basal ganglia and thalamus, as important role‐players in balance [53].
It is therefore not surprising that neuronal activity was detected in these cortical brain regions due to the complex task of postural stability and motor control, especially when performed on an unstable surface, in unstable stances, and with a sensory (visual feedback) input removed [53]. In addition, neuronal activity in these regions may have been caused by a suboptimal decision‐making process due to disturbance of the neuronal capacity by depressive moods, anxiety‐like symptoms, and suspected long‐term axonal micro‐trauma [51].
The inferior parietal cortex has been associated with the planning and interpretation of sensory information. The current case displayed neuronal activity in this region (i.e., dipole 1 and 6) (Table 2) [53]. While not directly linked to motor execution, this region has been suggested to play a role in balance through higher‐order integration of information [53]. Findings in the parietal regions were also more common in studies that measured dynamic balance [53]. These findings were reflected in the current case report (i.e., dipole 1 and 6) (Table 2).
Frontal lobe, temporal, and occipital regions also displayed signs of activity in the current case report (dipole 4, 7, 8, 9, and 10) (Table 2); however, the variability across multiple structures within them indicates a need for further studies to explore their specific role in balance regulation [53].
Another stand‐out region of brain activity in the current case was the occipital lobe region (dipole 8 and 9) (Table 2). Since this region of the brain is most associated with visual imagery processing, the activity might be due to the fact that tests included a 60‐s eyes‐open natural double stance baseline (used for reference in qEEG data processing) [41].
Conclusion
3.2
One cannot make an inference from one case and further data collection; longitudinal and comparative studies (i.e., pre‐ and post‐concussion) should be conducted to determine if significant changes are present. Study limitations and future research suggestions are discussed in Appendix B.
Author Contributions
M. J. Lumb: conceptualization, data curation, formal analysis, investigation, methodology, project administration, writing – original draft, writing – review and editing. N. Snegireva: conceptualization, supervision, writing – original draft, writing – review and editing. A. M. Coetzee: data curation, investigation, methodology, project administration, writing – review and editing. K. E. Welman: conceptualization, funding acquisition, resources, supervision, writing – review and editing.
Ethics Statement
The study was ethically approved by the Health Research and Ethics Committee (HREC) under the following project ID: 26062 and reference number: S22/08/145 (PhD). Written informed consent was provided by the participant, providing permission for his findings to be published in academic journals as long as all identifiable indicators were removed. Original written consent forms will be retained by the primary researcher and provided to the publisher if requested.
Conflicts of Interest
The authors declare no conflicts of interest.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1D. K. Broshek , J. E. Pardini , and S. A. Herring , “Persisting Symptoms After Concussion: Time for a Paradigm Shift,” PM & R: The Journal of Injury, Function, and Rehabilitation 14, no. 12 (2022): 1509–1513, 10.1002/pmrj.12884.PMC 1008767636152344 · doi ↗ · pubmed ↗
- 2S. Purkayastha , H. Adair , A. Woodruff , et al., “Balance Testing Following Concussion: Postural Sway Versus Complexity Index,” PM & R: The Journal of Injury, Function, and Rehabilitation 11, no. 11 (2019): 1184–1192, 10.1002/pmrj.12129.30729729 · doi ↗ · pubmed ↗
- 3T. Jennings and M. S. Islam , “Examining the Interdisciplinary Approach for Treatment of Persistent Post‐Concussion Symptoms in Adults: A Systematic Review,” Brain Impairment 1, no. 1 (2022): 1–19, 10.1017/Br Imp.2022.28.38167190 · doi ↗ · pubmed ↗
- 4J. S. Patricios , K. J. Schneider , J. Dvorak , et al., “Consensus Statement on Concussion in Sport: The 6th International Conference on Concussion in Sport–Amsterdam, October 2022,” British Journal of Sports Medicine 57, no. 11 (2023): 695–711, 10.1136/bjsports-2023-106898.37316210 · doi ↗ · pubmed ↗
- 5N. D. Silverberg , G. L. Iverson , A. Cogan , et al., “The American Congress of Rehabilitation Medicine Diagnostic Criteria for Mild Traumatic Brain Injury,” Archives of Physical Medicine and Rehabilitation 104, no. 8 (2023): 1343–1355, 10.1016/j.apmr.2023.03.036.37211140 · doi ↗ · pubmed ↗
- 6Ö. Kilic , P. Hopley , G. M. M. J. Kerkhoffs , et al., “Impact of Concussion and Severe Musculoskeletal Injuries on the Onset of Mental Health Symptoms in Male Professional Rugby Players: A 12‐Month Study,” BMJ Open Sport & Exercise Medicine 5, no. 1 (2019): e 000693, 10.1136/bmjsem-2019-000693.PMC 693705431908840 · doi ↗ · pubmed ↗
- 7A. L. Mc Pherson , T. Nagai , K. E. Webster , and T. E. Hewett , “Musculoskeletal Injury Risk After Sport‐Related Concussion: A Systematic Review and Meta‐Analysis,” American Journal of Sports Medicine 47, no. 7 (2019): 1754–1762, 10.1177/0363546518785901.30074832 · doi ↗ · pubmed ↗
- 8M. Makdissi , K. J. Schneider , N. Feddermann‐Demont , et al., “Approach to Investigation and Treatment of Persistent Symptoms Following Sport‐Related Concussion: A Systematic Review,” British Journal of Sports Medicine 51, no. 12 (2017): 958–968, 10.1136/bjsports-2016-097470.28483928 · doi ↗ · pubmed ↗