Magnitude of sexual and reproductive health communication between parents and their adolescents: Evidence from Osun State, Nigeria
Olayinka Oluwabusola Bamidele, Agnes Aderinola Oyeniran, Olukemi Adedayo Sabageh, Esther Olufunmilayo Asekun-Olarinmoye

TL;DR
This study explores how often parents and teenagers in Nigeria talk about sexual and reproductive health, finding differences based on location and gender.
Contribution
The study provides new insights into SRHC disparities in urban and rural Nigeria, emphasizing the need for targeted interventions.
Findings
About 56% of parents and 69% of adolescents in Osun State reported ever having SRHC.
Urban parents had a significantly higher level of SRHC compared to rural parents.
Female rural adolescents and early urban adolescents had higher odds of good SRHC with their parents.
Abstract
This study evaluated sexual and reproductive health communication (SRHC) between dyads of parents and their in-school adolescents in urban and rural areas of Osun State, Nigeria. A descriptive cross-sectional design was used to determine and compare the prevalence, pattern, level, triggers, and methods of SRHC between 625 parents and their in-school adolescents. Respondents were recruited using the multistage sampling technique, and data was collected using the mixed-method approach. Quantitative data was collected using a semi-structured questionnaire and analysed using chi-square and logistic regression tests, while the qualitative data was collected using a focus group discussion guide and analysed thematically. About 56% of parents (53% rural, 58% urban) and 69% of adolescents (68% rural, 71% urban) reported ever having SRHC. The level of SRHC was 31% for adolescents, with no…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
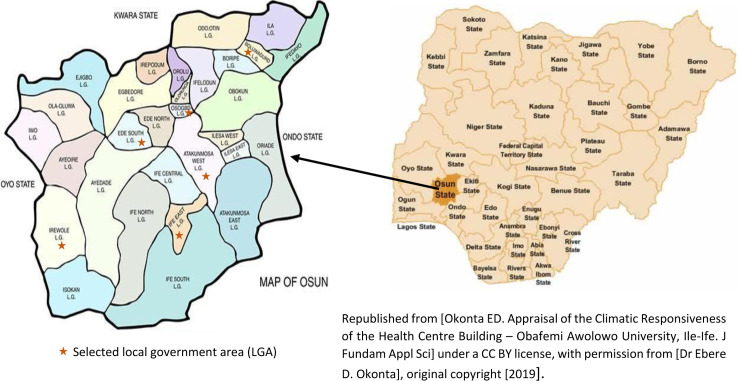 Fig 1
Fig 1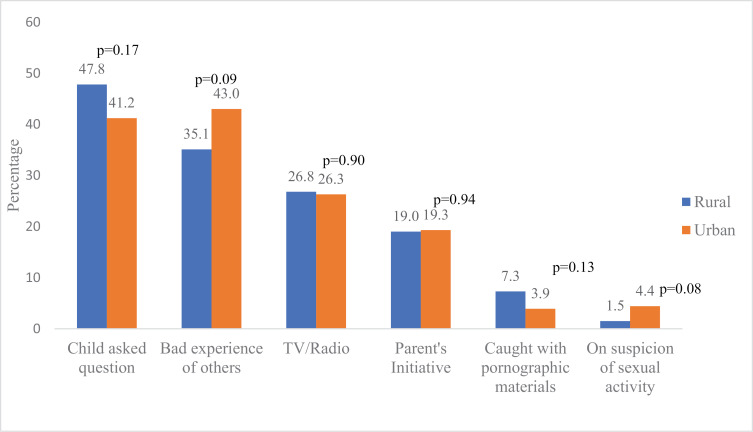 Fig 2
Fig 2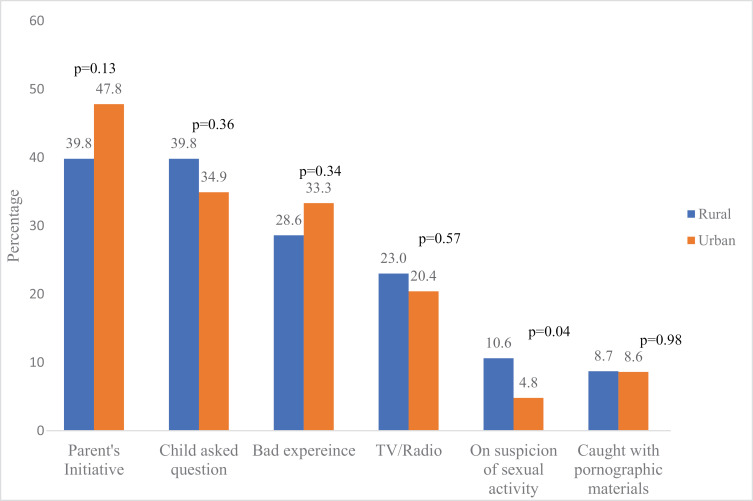 Fig 3
Fig 3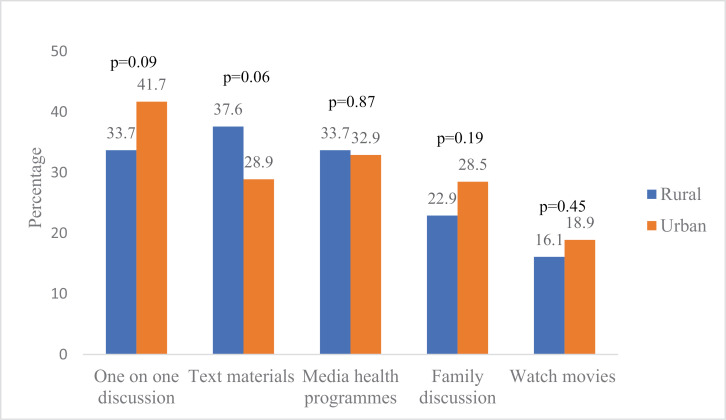 Fig 4
Fig 4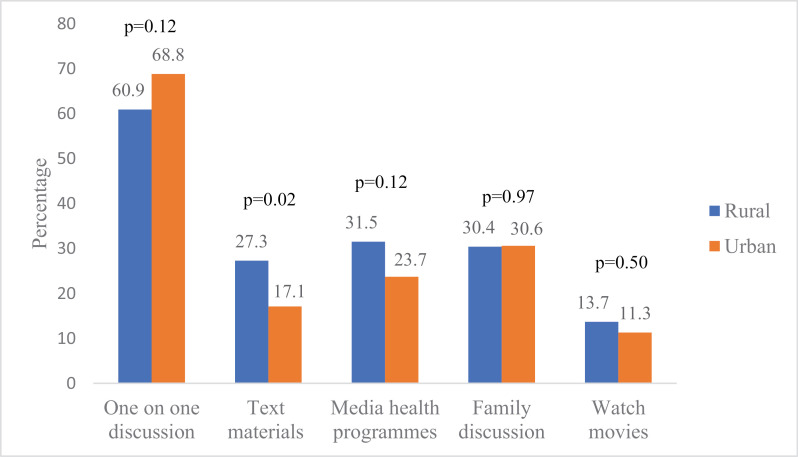 Fig 5
Fig 5Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAdolescent Sexual and Reproductive Health · HIV/AIDS Research and Interventions
Introduction
Adolescents are individuals aged 10-19 years in the adolescence stage of life, a transitional stage characterized by developmental, physiological, and behavioural changes during which an individual reaches sexual maturity [1–3]. Their curiosity about all areas of human undertaking is enhanced by physiological changes in their reproductive organs, which serve as a stimulus in their quest to experiment with sex and sexual relationships [4]. Thus, it is critical for them to be guided appropriately during this stage to make positive and informed decisions about their sexual and reproductive health (SRH). A practical approach to achieve this is through sexual and reproductive health communication (SRHC) [5].
SRHC is the process of sending and receiving messages about SRH issues from one entity or group to another through verbal or nonverbal means using mutually understood signs, signals, and behaviour. Providing SRH education to adolescents is known to play a vital role in preventing risky sexual behaviour and its untoward consequences among this target group [5]. Evidence has shown that communication between adolescents and their parents during this crucial period protects adolescents from engaging in risky sexual practices and associated adverse health consequences [6–9].
Despite these documented benefits, providing SRH information to adolescents is quite challenging because it is a culturally sensitive issue, particularly in Africa [10]. Many African societies have well-established traditions about accepted norms concerning sexual activities and reproduction among the young, as well as specific ways through which relevant SRH information and values are communicated [10].
Premarital sexual activities are prevalent among adolescents in Nigeria and have remained so [11–13]. Studies have reported a high level of sexual activity among unmarried adolescents of both sexes with progressively decreasing ages of sexual debut [11–13]. The problem is not that adolescents are sexually active; instead, they are inadequately prepared and guided in developing responsible sexual behaviours [7]. Adolescents form a more significant percentage of the Nigerian population and are a critical asset to the country’s future; hence, they must be protected and safeguarded. The preceding underscores the role of significant others, including parents, in providing SRHC to adolescents.
Whereas previous studies have focused on SRHC among either parents or adolescents, there is a dearth of information on SRHC between parents and their adolescents from the perspective of dyads of parents (fathers and mothers) and adolescents (sons and daughters) and with a rural/urban comparison. In our extensive literature search, the only few available studies found on SRHC among dyads of parents and adolescents were a mixed-method study conducted in Ghana [14], a qualitative survey of mother-daughter dyads conducted in Northern Nigeria (Kano State) [15], and another mother-daughter dyad study carried out in Uganda but without rural/urban comparison [16].
Exploring SRHC within the context of parent-adolescent dyads goes beyond merely assessing the strength of communication but also delving into the accuracy of information shared within a family unit [15]. Therefore, examining SRHC through the framework of parent-adolescent dyads offers a holistic and balanced evaluation of the content, accuracy, and congruence of information exchanged between parents (fathers and mothers) and their adolescents (sons and daughters). Previous research on SRHC between parents and adolescents has been constrained by the limited inclusion of both members of the parent-adolescent dyad. This restricted approach has hindered a comprehensive understanding of the intricate family dynamics involved in SRHC. However, dyadic analyses of SRHC have demonstrated an ability to unveil between and within variations in communication patterns among members of the parent-adolescent dyad [17].
Furthermore, SRHC, from the perspective of the parent-adolescent dyad, provides an opportunity to effectively capture the reciprocity required in the communication process, particularly within the family unit, which is significantly influenced by the area (rural or urban). As a fundamental unit of society, the family plays a pivotal role in shaping adolescents’ sexual health and behaviours [18]. Understanding the communication dynamics within this unit is imperative for tailoring appropriate public health interventions. While communication is a two-way reciprocal process, the sensitivities associated with SRHC within the African context underscore an increased need for mutuality between dyad members. Therefore, this study centered on dyads of parents and adolescents to contribute nuanced insights into the reciprocal nature of SRHC and identify potential areas for intervention within family structures in both rural and urban areas. Specifically, the study evaluated SRHC by determining and comparing the prevalence, pattern, level, triggers, and methods of SRHC between dyads of parents and their in-school adolescents in urban and rural areas of Osun state.
Materials and methods
Study design and setting
A mixed-method design was used for this study involving a cross-sectional survey for the quantitative aspect and focus group discussions (FGDs) for the qualitative aspect. The study was conducted between1st April and 30th June 2018 among parents and their in-school adolescents in six (Atakumosa West, Boluwaduro, Ede South, Ife East, Irewole and Osogbo) local government areas (LGAs) of Osun State, in southwest Nigeria (Fig 1). Osun State has 30 LGAs, distributed equally among its three senatorial districts (10 LGAs per district). The LGAs are further divided into rural and urban areas [S1 Table]. The State has an estimated population of 4,340,565, of which 23.7% are adolescents, and 55.5% live in rural areas [19,20].
Map of Osun State, Nigeria, showing the selected local government areas [21,22].
Participants
The study population was in-school adolescents aged 10–19 years and their parents (biological parents or guardians>18 years) residing in the study sites. A total of 660 parent-adolescent pairs across six LGAs were selected for the quantitative part of the study. The adolescents served as the index participants and were used to recruit their parents into the study with the help of the school authority. The inclusion criteria were adolescents aged 10-19 years attending public or private secondary schools in the State and primarily living with their parents in the past twelve months before the study. Married adolescents and those whose parents were unavailable were excluded from the study. For the qualitative component, eight FGDs were conducted in two LGAs (one rural and urban) among adolescent boys, adolescent girls, male parents, and female parents. Participants for the FGD were chosen by convenience (a non-probability) sampling technique.
Adolescent participants
A multistage sampling technique was used to select the adolescents, which included a proportionate allocation to determine the number of participants in each of the selected schools and arms (JSS1-SSS3). First, simple random sampling was used to select two LGAs (one rural and one urban) from the three senatorial districts by utilizing the ballot technique. This yielded a total of six LGAs. Second, two secondary schools (one public and one private) were selected from each of the LGAs using simple random sampling by the ballot method. These schools (12) were selected from a list of all registered secondary schools in the six LGAs, as obtained from the state Ministry of Education. Third, simple random sampling was used to select one class from each of the arms in the junior (levels 1-3) and senior (levels 1-3) secondary categories of the respective schools resulting in six classes per school. Proportionate allocation was used to determine the total number of students to be interviewed in each of the selected schools. This was calculated as below:
The total number of students calculated for each school was allocated proportionately across the six classes selected from the junior and senior secondary categories. This allocation was used in determining the number of students to be interviewed in each of the selected classes. It was calculated using the number of eligible students in each class, the total number of eligible students in all the selected classes in each school, and the sample size for each school.
The last stage adopted systematic random sampling to select participants in each of the chosen classes using the class register as the sampling frame. The first participant was selected by simple random sampling using the ballot method. Subsequent participants were selected based on the sampling interval in each class until the sample size was achieved. The adolescents participated in the study at their respective schools.
Parent participants
The parents participated in the study within the household settings. Both parents were eligible to participate in the survey, but only one was allowed. Where both parents were willing to participate, a simple ballot was used to select the participating parent randomly.
Sample size
The sample size was determined using the formula to compare two proportions [23]. The prevalence of SRHC among adolescents in the urban area was 63.4% [24], and an assumed prevalence of 50% was used for the rural area to obtain a minimum sample size of 287. After adjusting for a 10% non-response rate, a sample size of 660 parent-adolescent pairs was finally used.
Instrument and variables
The data was collected via pre-tested, semi-structured questionnaires (adapted from previous studies [7,14] with separate questionnaires for adolescents and their parents) and an FGD guide. The questionnaire was modified without obtaining permission from its original owner. Both tools were translated into the local language, Yoruba, for ease of comprehension. Content validity of the tools was ensured through translation-back translation (English-Yoruba-English) by separate translators. The reliability test, which measured the internal consistency of the adolescents’ and parents’ questionnaires, yielded an overall Cronbach’s alpha of 0.98 for each group of participants.
The questionnaires were used to elicit information on participants’ demographic characteristics, prevalence and pattern of SRHC, and SRH topics discussed. Sociodemographic characteristics include the following:
Age- Adolescents (10-14 years, 15 -19 years): Parents (40 and below; 41 – 60, Above 60)Gender – Male, femaleReligion – Christianity, Islam, TraditionalClass – (for adolescents) JSS 1-3, SSS 1-3Birth Order - 1st, 2nd-5th, 6^th^ -9^th^living with - (for adolescents) Both parents, mother only, female guardian, male guardian, father onlyEducational Level (for parents) – Primary and below, Secondary, TertiaryOccupation (for parents) – Business/trader, Civil servants, farmer, artisansIncome (for parents) - < N20,000, N 20,000 – N 50,000, > N 50,000Marital status (for parents) – single, married, divorced, widowedMarriage type (for parents) – monogamy, polygamyPlanned marriage (for parents) – yes, no.
Prevalence was measured based on the singular question of “have you ever discussed SRH issues with your child or have your parents discussed SRH issues with you”. The SRH topics were measured through 20 distinct items and categorized into three domains. The biological/developmental domain had five items (physical development, menstruation/ wet dreams, puberty, masturbation, and reproduction/having babies), sexual risk prevention or safety domain had eight items (prevention of STI, prevention of HIV/AIDS, condom & other contraceptives use, abstaining from sex till marriage, pregnancy, abortion, consequences of premarital sex, and substance use), and experiencing sex domain had seven items (sexual feeling, when to commence sexual intercourse, choosing sexual partners, how to handle sexual pressure, homosexuality, pornography, and rape) [14]. Discussion of SRH topics was measured on a 4-point Likert scale (0 = never, 1 = once, 2 = a few times, and 3 = often) and was used to rate the level of communication, which was scored and graded as poor (≤ 30) and good (>30). For the adolescents, the mean SRHC score for father and mother communication was used to rate the level of communication. The main purpose of the FGD as a qualitative tool was to aid the quantitative aspect to further explore in depth knowledge and also to triangulate findings from the quantitative aspect.
Data collection procedure
The data was collected by trained research assistants (RAs) who administered the questionnaire to the adolescents at their school. In-school adolescents served as leads for selecting parents with the help of the school authority. After that, the RAs contacted the parents and administered the questionnaire to the parents in their homes. The qualitative part of the study was facilitated by the researcher, who was assisted by the trained RAs as note-takers. Eight FGDs were conducted in two LGAs (one rural and one urban), separately among adolescent boys, adolescent girls, male parents, and female parents in each LGA to ensure homogeneity. The FGDs were double audio-recorded, and each lasted 45 minutes to one hour.
Statistical analysis
Of the 660 parent-adolescent pairs responses received, 35 pairs were excluded due to incomplete information. Hence, data from 625 parent-adolescent pairs were included in this analysis. Statistical analysis was performed using Statistical Product and Service Solutions (SPSS) version 21, with the significance level set at p ≤0.05. Univariate analysis was done to generate frequencies and percentages, and Chi-square (χ2) test statistics was utilized to assess association and compare differences between two categorical variables. Continuous variables were presented as mean ± standard deviation. Logistic regression was used to estimate the odds ratio at 95% confidence intervals for significant variables at Chi-square to estimate the magnitude and direction of the relationship. e.g., SRHC level of adolescents/parents with sociodemographic factors that are significant at chi-square. The audio-recorded FGD sessions were transcribed verbatim, and a report of each was computed. These reports were analysed thematically through group coding of similar responses, and quotes that buttressed the quantitative component of the study were integrated into the findings.
Ethical considerations
The study was conducted in accordance with the Declaration of Helsinki. It was approved by the Ethics Review Committee of the Osun State Ministry of Health on August 6, 2017 (Approval no. OSHREC/PRS/569T/143). Official permission to carry out the study was obtained from the Osun State Ministry of Education and the principals of the selected schools. Informed written consent was obtained from participants ≥ 18 years and assent from those < 18 years after obtaining written consent from parents/guardian; parents also signed consent forms before completing the questionnaires. Anonymity and confidentiality of responses were assured, and participants had the right to refuse or withdraw participation at any time during the study.
Results
Comparison of socio-demographic characteristics by type of residence
Table 1 shows the socio-demographic characteristics of the participants. Adolescents’ mean age was 14.23 ± 2.0 years, 14.19 ± 2.1 years in the rural area, and 14.40 ± 2.0 in the urban area. There were more females (58.4%) than males (41.6%), and this was comparable for the type of residence. More than half (54.9%; 52.5% rural; 57.1% urban) were in junior secondary school. Most adolescents live with both parents (62.4%; 61.1% rural; 63.7% urban). There were significant differences in religion and birth order. (p<0.001). A more substantial percentage of the parents were between 41 and 60 years (54.6%). However, more parents in the rural area were 40 years and below (48.5%), with a significantly lower percentage of urban parents (33.9%) in this age category (p=<0.001). More female parents (68%) participated in the study than male parents (32%) in rural and urban residences. There were significant differences in parental age p=<0.001, income p=<0.001, religion p=0.001 marital status p=<0.001, type of marriage p=0.030, and whether the marriage was planned p=0.020 across the type of residence.
Table 1: Socio-demographic characteristics of respondents according to their residence.
Comparison of the prevalence and pattern of SRHC by type of residence
The prevalence of SRHC was measured using a single dichotomous variable. Have you ever discussed SRH issues with your adolescent/parents (Yes/No)? About 70% of adolescents and 55.5% of parents responded affirmatively (Table 2). In urban areas, 70.8% of adolescents and 57.8% of parents reported discussing SRH issues, compared to 67.7% of adolescents and 53.1% of parents in rural areas. In the FGDs, 67.0% (20 out of 29) of adolescents and 58.6% (17 out of 29) of parents answered yes to the same question.
Table 2: Prevalence of SRHC according to respondents by their residence.
Table 3 gives an overview of parents’ reasons for not discussing SRH issues with their adolescents. Overall, 44% of parents never discussed SRH with their adolescents. Reasons adduced by parents who had never had SRHC with their adolescents (278/625, 44%) were mainly that their adolescents were not mature enough for such discussion (74.1%). However, more urban parents (83.8%) significantly proffered this reason than the rural parents (64.8%), p=<0.001. Other reasons were the perception that it makes the child promiscuous (rural, 12.7%; urban, 7.4%), p=0.146, initiating the discussion is embarrassing (rural, 9.9%; urban, 13.2%), p=0.378, and the child will learn as he/she grows (rural, 11.2%; urban, 13.3%), p=0.617. Furthermore, some fathers stated that it is the mother’s duty (7.9%), and this perception was statistically significant by the type of residence (rural, 2.8%; urban, 13.2%) (p=0.001) [Table 3].
Table 3: Parents’ reasons for not discussing SRH issues with their adolescents.
The FGD discussants stated that the reasons for the lack of SRHC is because their work schedule does not permit it, and they never benefitted from such discussions as young people. One of the discussants emphasized this perception about SRHC, which is indicative of an authoritarian parenting style:
R: I don’t know the meaning, I don’t understand (all laughed). The reason why I don’t understand is that no parent ever discussed such with me before about sex and reproduction. The only thing I used to tell my children is to make sure they pursue their academics to the peak, and if you will learn a trade and make sure you have good work, I tell both males and females. That is what I do tell them most of the time. _ Male parent, rural area.
The majority of the adolescents had reached the stage of adolescence before SRHC was initiated. There was no significant difference in the reported age of SRHC initiation by adolescents (72.2%, 77.2%, p = 0.232) and their parents (85.1%, 81.2%, p = 0.334) in the rural and urban areas, respectively. Among the adolescents, the frequency (p=0.088) and duration of SRHC (p= 0.190) were not significantly different by the type of residence. However, this difference (frequency (p = 0.002) and duration of SRHC (p = < 0.001) was statistically significant among the parents [Table 4]. A similar view on SRHC initiation was shared by the FGD discussants, with 15 of the 27 adolescents and 20 out of 23 parents in both areas reporting SRHC between 10 and 19 years. However, some of the parents stated that SRHC should begin before age ten due to early puberty onset:
Table 4: Pattern of SRHC according to adolescents and parents by their residence.
R: Because the world has changed. In those days, before a girl could reach puberty, it would be up to 14 years and above, but nowadays, a girl can reach puberty at ten years of age, even, I can say, nine years. Hence, let’s say ten years of age for both males and females. _ Male parent, rural area.
R: …About five years, because nowadays, a child of 2, 3 years of age has started school already and whatever he has been taught he would not forget. _ Female parent, rural area
Comparison of triggers and methods of SRHC by type of residence
The triggers of SRHC among adolescents were comparable in rural and urban areas (Fig 2). Asking questions by adolescents (47.8%) ranked highest among respondents from rural areas, while bad experiences of other people (43.0%) ranked highest among urban adolescents. Parental initiative was the most reported trigger of SRHC for parents in both rural (39.8%) and urban (47.8%) (Fig 3). There was no significant difference in the reported triggers of SRHC except for that on suspicion of sexual activity: more parents (17, 10.6%) in the rural areas significantly had SRHC based on suspicion of sexual activity compared to their urban (9, 4.8%) counterparts (p=0.04) (Fig 3).
Triggers of SRHC among adolescents according to their residence.
Triggers of SRHC among parents according to their residence.
Similar methods of SRHC were adopted in the two study areas. The primary method reported by adolescents in the rural area was the giving of text materials by parents (37.6%), while one-on-one discussion ranked highest among their urban counterparts (41.7%) (Fig 4). One-on-one discussion ranked highest among methods adopted for SRHC among parents in rural (60.9%) and urban (68.8%) areas. There was no significant difference in the reported methods of SRHC adopted except for the use of text materials: more parents in the rural regions significantly adopted the use of text materials for SRHC compared to their urban counterparts (p=0.02) (Fig 5).
Comparison of methods adopted for SRHC among adolescents by type of residence.
Comparison of methods adopted for SRHC among parents by type of residence.
Comparison of SRH topic discussed by type of residence
SRH topics discussed by parents and their adolescents were measured using 20 topics, categorized into three domains: biological/developmental, sexual risk prevention, and experiencing sex. In addition, adolescents were asked to specify which of their parents, mother/father, discussed any of the topics with them. Overall, more parents in the urban areas reported discussing SRH topics with their adolescents than those in the rural areas. There was a statistically significant difference in the proportion of parents in the urban and rural who discussed 11 of the 20 SRH topics (Reproduction/having babies (80.6%,67.7%, p-0.006; prevention of STIs (88.7%,74.5%,p-0.001; prevention of HIV/AIDS (88.2%,78.3%, p-0.013; abstaining from sex till marriage (91.4%,83.9%, p-0.032; pregnancy (81.7%,70.2%, p-0.012; abortion (70.0%,59.0%,p-0.019); consequences of premarital sex (86.0%,71.4%,p-0.001); sexual feeling (69.4%,46.4%,p-0.044); when to start sexual intercourse (73.7%,61.5%, p-0.015); choosing sexual partners (72.6%,62.1%,p-0.038); rape (72.6%,59.6%, p-0.011) [Table 5].
Table 5: Topics discussed as reported by adolescents and parents according to their residence.
From the adolescents’ perspective, urban mothers discussed 15 SRH topics more than their rural counterparts, while rural mothers discussed five SRH topics more than their urban counterparts. These five topics were choosing sexual partners, handling sexual pressure, consequences of premarital sex, homosexuality, and pornography. However, only discussion on menstruation/wet dreams (82.0%,72.7%, p-0.020), puberty (81.6%,73.2%, p-0.036), prevention of STI (73.7%,63.9%,p-0.028)and abstaining from sex till marriage (74.6%,65.9%, p-0.047), differed significantly between urban and rural mothers. By contrast, the adolescents reported more SRH discussion across all 20 topics by rural fathers compared to their urban counterparts. This difference was statistically significant across 13 topics [physical development (64.0%, 75.6%, p-0.009); puberty (64.0%, 75.1%, p-0.013); masturbation (30.7%, 42.0%, p-0.015); prevention of HIV/AIDS (59.2%, 71.7%, p-0.006); abstaining from sex till marriage (62.3%, 76.6%, p-0.001); pregnancy (44.3%, 54.1%, p-0.041); consequences of premarital sex (48.2%, 65.4%, p-<0.001); substance abuse (39.9%, 58.0%, p-<0.001); sexual feeling (39.9%, 52.2%, p-0.010); when to start sexual intercourse (43.4%, 55.1%, p-0.013); choosing sexual partners (37.3%, 52.7%,p-0.001); how to handle sexual pressure (39.5%, 53.7%, p-0.003); pornography (33.3%,47.8%, p-0.002) except for seven topics (masturbation, reproduction/having babies, prevention of STIs, condom and other contraceptive use, abortion, homosexuality, and rape) [Table 5].
In the FGD sessions, both adolescents and parents in rural and urban areas stated that menstruation is a commonly discussed SRH topic between them. Parents and urban adolescents also mentioned puberty, while parents and rural adolescents said prevention of STI and HIV/AIDS. One of the parents described the topics she has discussed with her adolescents, which cuts across the three domains:
R: I called my children, my firstborn, that with your level of maturity, if you are not careful and face your studies, if you have a secret girlfriend and you are having sex secretly, and she gets pregnant, that shows that you can take care of the responsibility by yourself, don’t do that, and the one that is female I told her, you have started menstruating, if you allow a man to have sex with you and you get pregnant that means you are ripe and ready for family life. _ Female parent, urban area.
R: My mom told me that I should not move close to boys, that the boy should not touch my private parts, and I should not have any sex with boys, and when a woman gets pregnant and engages in abortion, that woman can either die or her womb may be destroyed. Also, she said when it’s time for menstruation, they will be telling me everything about when menstruation will come. _Adolescent girl, urban area
Comparison of the level of SRHC by type of residence
The level of SRHC based on the perspectives of the adolescents and their parents by the type of residence is shown in Table 6. Participants’ level of SRHC was measured by recoding and scoring the 4-point Likert scale (0 = never, 1 = once, 2 = a few times, and 3 = often) used to measure discussion of SRH topics. After scoring, this was graded as poor (≤ 30) and good (>30). For the adolescents, the mean SRHC score for father and mother communication was used to rate the level of SRHC. From the adolescents’ perspective, the level of SRHC between them and their parents was poor (66.7%), with no significant difference between the rural and urban adolescent respondents. Based on the parents’ responses, however, about 60% achieved a good level of SRHC, with statistically significant differences (p-0.006) by type of residence: more parents in the urban areas (66.1%) had a good level of SRHC compared to those in the rural areas (51.6%).
Table 6: Respondents’ level of SRHC according to their residence.
Comparison of socio-demographic characteristics by level of SRHC
We evaluated the association between participants’ socio-demographic characteristics and level of SRHC by the type of residence [Table 7]. Female adolescents (41.4%) in the rural areas had a significantly higher level of SRHC with their parents than their male counterparts (27.0) (p=0.032). Early adolescents (36.5%) reported a substantially higher SRHC level than late adolescents (20.6%) (p=0.009) in the urban area Among rural parents, income, planned marriage, and type of marriage were significantly associated with the level of SRHC. In contrast, among urban parents, there was a significant relationship between the level of SRHC and age, sex, education, occupation, income, and planned marriage.
Table 7: Association of socio-demographic characteristics and level of SRHC by their residence.
Logistic regression analysis of the level of SRHC by independent variables
On regression analysis [Table 8], planned marriage (rural parents) and age, education, occupation (urban parents) did not remain significantly associated with the level of SRHC. Female rural adolescents were 1.9 times more likely to have good SRHC compared to their male counterparts while early adolescents in the urban area were 2.2 times more likely to have good SRHC compared to late adolescents in the same area.
Table 8: Predictors of SRHC level among respondents by their residence.
Rural parents in monogamous marriage and those who earn above ₦50,000 were 2.3 times and about 5 times more likely to have good level of SRHC with their adolescents than those in polygamous marriage and who earn less than ₦20,000, respectively. Urban parents in unplanned marriage were nearly 5 times more likely to have good SRHC than those whose marriages were planned, and mothers were 3.4 times more likely than fathers to have good SRHC with their adolescents. SRH discussions with urban parents that lasted more than 30 minutes were twice as likely to be more beneficial than those that lasted less than or equal to 30 minutes. Additionally, those who earn between ₦20,000 and ₦50,000 were five times more likely to have good SRHC than those who earn less than ₦20,000.
Discussion
This study evaluated SRHC between parents and their in-school adolescents in rural and urban areas of Osun State to identify key similarities, disparities, and factors influencing SRHC. Unlike many previous studies that concentrated on either parents or adolescents, our research adopts a dyadic approach, exploring the interactions between parents (fathers and mothers) and adolescents (sons and daughters). Additionally, we provide a rural/urban comparison, offering insights into how the dynamics of SRHC vary between these distinct settings.
Adolescents reported a higher SRHC prevalence than parents (69.3% vs 55.5%) based on a single question (Ever discussed issues about SRH). This prevalence is lower than SRHC reported by parents in studies conducted in Ghana and northern Nigeria but comparable to adolescent SRHC prevalence in studies conducted in Osun State [25], north Nigeria [15], and Ghana [14]. The reason for adolescents reported higher SRHC prevalence compared to their parents is unclear. Still, it may be due to more consciousness of SRHC on the part of the adolescents, with more parents being forgetful about such discussions.
Some parents in this study had never had SRH discussions with their adolescents, and the primary reason for this is that their children were still too young for SRH discussions. This finding is contrary to a study that reported that the majority of respondents cited a lack of knowledge about RH issues and difficulties bringing up the topic because of fear [7]. This perception by parents in our study could have severe consequences for their adolescents, who may choose to rely on their peers, social media, and strangers for information and support for their SRH needs and consequently make poor SRH choices [26]. SRH information from peers and strangers could also be fraught with misinformation about SRH issues and changes in adolescence [27]. Surprisingly, more urban parents significantly reported this perception compared to rural parents. School attendance and length of stay in school are higher in urban areas than in Nigeria’s rural areas [28].
Consequently, urban populations are more likely to delay marriage and childbirth [29]. This might be the projection of these parents who believe that their adolescents are too young for SRH discussion. However, participation in risky sexual behaviour and early sexual debut cuts across adolescents in both urban and rural areas [30].
This study revealed that some fathers believed that SRH discussion is the responsibility of mothers. Our findings parallel a Uganda study that reported that fathers abdicate their roles of communicating about SRH to mothers [31]. This perspective was more strongly held in urban areas than rural areas. It may be linked to the fast-paced environment of the metropolitan regions where parents, particularly fathers, are tied up outside the home for extended periods due to work schedules and pressure [32]. This work-related stressor leaves little room for SRHC between parents and their adolescents, which exposes adolescents to reliance on incorrect or false SRH information through alternative sources [27]. Some parents in both our study locations, with a higher proportion among parents in rural areas, were hesitant to talk to their adolescents about sexual matters out of concern that it could facilitate indulging in sexual practices. This finding is consistent with a study in Harar, Eastern Ethiopia [7].
SRHC was generally higher among females than males and with early adolescents (10-14 years) than late adolescents in both locations. This difference was significantly higher for females in the rural area and early adolescents in the urban area. This agrees with earlier studies done in the USA, West Ethiopia, and Zambia in which parents tend to communicate less with their adolescents as they advance in age [33–35]. Furthermore, mothers talked to their children more than the fathers in both study locations, comparable to studies conducted in Nigeria, Ghana, and Tanzania [14,25,36] but contrary to an Ethiopian survey that found that fathers communicated more with their teenage children [7]. However, our findings on higher levels of SRHC by fathers in rural areas compared to their urban counterparts are consistent with the Ethiopian study. A possible explanation is that living in rural communities is associated with less work pressure and stress, allowing for more family time, cohesion, and discussion.
Though several respondents, especially the adolescents, reported a regular schedule and length of SRHC in the rural and urban areas, assessment of the level of SRHC, as determined by the 20 sexual topics, showed that the majority of the adolescents reported a poor level of SRHC. In contrast, the majority of the parents rated their level of SRHC as good. The level of SRHC was significantly higher among urban parents compared to their rural counterparts. This suggests that discussions around these topics held between parents and their adolescents were perceived as sufficient by the parents, while their adolescents perceived them as inadequate. The reasons for this disparity might be the need for more depth whenever the topics are discussed and different perceptions of SRHC such that adolescents cannot recognize and acknowledge such discussions as they are often devoid of meaningful dialogues. This is in line with previous studies where parents were adjudged to speak in parables when communicating about sexuality [15,37]. Their messages need to be delivered more transparently and understandably.
Our findings also showed that more parents shied away from discussing topics around experiencing sex compared to other SRH topic domains. This is not surprising because it has been documented that explicit discussion of sex with their children is often problematic for parents, and more often, they resort to the use of euphemisms that further confuse their adolescents [26,27,31]. Whereas there are available and accessible factual print and online materials on the biological and sexual risk prevention domains, materials on experiencing sex are scarce [38,39]. Expanding the scope of parent-adolescent SRHC to include the topic domain on experiencing sex is pertinent because it will assist and reinforce the adolescents in making guided and informed SRH decisions. SRHC materials specific to SRH topics such as sexual feelings, choice of sexual partners, rape, pornography, and sexual debut should be developed and accessible to both parents and adolescents.
Our study has some limitations. First, it was a cross-sectional survey; hence, a cause-effect relationship could not be established. Second, it was conducted among only in-school adolescents and their parents in selected schools across only six LGAs and based on participants’ self-reports; hence, caution should be exercised in generalizing the results. However, we employed a mixed data collection method among dyads of parents and their adolescents in both rural and urban areas, which allowed an in-depth and comparable exploration of SRHC. Furthermore, we used a multistage sampling to select participants across diverse geo-political zones, LGAs, and locations. The findings highlight potential entry points for interventions in parents-adolescents SRHC.
Conclusion
Although many parents in this study engage in SRHC with their adolescents, such discussions were inadequate and sometimes reactive and sporadic, triggered by suspicion of sexual activity. Fathers were still less involved in SRHC, and the male adolescents were less communicated with than the females. Reasons for non-discussion by some parents highlighted their perception and attitude towards SRHC. In addition, essential topics relating to experiencing sex are often not discussed, and the style of SRHC was ambiguous. These might be inadequate to protect and facilitate healthy SRH choices among adolescents. Hence, parents need to be enlightened about the importance, depth, and practical approaches toward SRHC. Knowledge and self-efficacy building activities will equip parents and adolescents with the skills required for early, effective, and sustained engagement on SRH issues, allowing for a “talk-the-talk” before the adolescents “walk the walk,” thereby ensuring adolescents live up to their most significant SRH potential and right. Health policymakers and program planners should ensure the inclusion of detailed and accurate SRH information covering all three domains of sexual topics (biological/developmental, sexual risk prevention, and experiencing sex) in the promotion of SRHC in school curricula and general public health enlightenment programmes. Bridging the resource and knowledge gap surrounding the underexplored SRH topic domain of experiencing sex requires dedicated efforts. Educational initiatives, research, and community outreach programs should be designed to provide accurate information, dispel myths, and create a supportive environment for discussing and understanding the complexities of sexual experiences between parents and their adolescents.
Supporting information
S1 TableLGAs in Osun State with categorization into rural and urban.(PDF)
S1 QuestionnaireStudy questionnaire for parents and adolescents.(DOCX)
S1 DataStudy data on adolescents.(SAV)
S2 DataStudy data on parents.(SAV)
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1World Health Organization (WHO). 2015. Available from: http://www.who.int/maternal_childadolescent/topics/adolescence/development/en/.”
- 2Nwankwo BO, Nwoke EA. Risky sexual behaviours among adolescents in Owerri Municipal: predictors of unmet family health needs. Afr J Reprod Health. 2009;13(1):135–45. 20687271 · pubmed ↗
- 3Doyle AM, Mavedzenge SN, Plummer ML, Ross DA. The sexual behaviour of adolescents in sub-Saharan Africa: patterns and trends from national surveys. Trop Med Int Health. 2012;17(7):796–807. doi: 10.1111/j.1365-3156.2012.03005.x 22594660 · doi ↗ · pubmed ↗
- 4Imaledo J, Opirite Peter-Kio O, Asuquo E. Pattern of risky sexual behavior and associated factors among undergraduate students of the university of port Harcourt, Rivers State, Nigeria. Pan Afr Med J. 2012;9:97.PMC 348939823133697 · pubmed ↗
- 5Saskatchewan Prevention Institute. Parents as Sexual Health Educators. 2011. [Cited 2016 Nov 21]. Available from www.Skprevention.ca/shop/parents-as-sexual-health-educators-executive-summary//
- 6Dessie Y, Berhane Y, Worku A. Parent-adolescent sexual and reproductive health communication is very limited and associated with adolescent poor behavioral beliefs and subjective norms: evidence from a community based cross-sectional study in eastern Ethiopia. P Lo S One. 2015;10(7):e 0129941. doi: 10.1371/journal.pone.0129941 26167860 PMC 4500400 · doi ↗ · pubmed ↗
- 7Yadeta TA, Bedane HK, Tura AK. Factors affecting parent-adolescent discussion on reproductive health issues in Harar, eastern Ethiopia: a cross-sectional study. J Environ Public Health. 2014;2014:102579. doi: 10.1155/2014/102579 24987424 PMC 4060393 · doi ↗ · pubmed ↗
- 8Di Iorio C, Kelley M, Hockenberry-Eaton M. Communication about sexual issues: mothers, fathers, and friends. J Adolesc Health. 1999;24(3):181–9. doi: 10.1016/s 1054-139x(98)00115-3 10195801 · doi ↗ · pubmed ↗