Star Can Vac Capsulorhexis in White Total Cataracts - A Retrospective Interventional Analysis
Kodavoor Shreesha Kumar, Raju Sumithra, S. Tamilarasi, Dandapani Ramamurthy

TL;DR
This study introduces a new technique called Star CanVac capsulorhexis to safely create a circular opening in white cataracts, reducing the risk of tears during surgery.
Contribution
The novel Star CanVac technique uses vacuum and accessible tools to safely perform capsulorhexis in challenging white cataract cases.
Findings
The Star CanVac technique was successfully performed in 564 out of 570 cases.
Six eyes experienced anterior capsular tears, with two extending into the posterior capsule.
The method effectively balances pressure and removes liquefied cortex during the procedure.
Abstract
Completing circular uniform anterior capsulorhexis in intumescent white cataracts is challenging for all cataract surgeons. Numerous techniques have been described to get a circular capsulorhexis and prevent perpendicular linear tears in the anterior capsule. 570 cases of white total cataracts were selected for this retrospective clinical study. In this technique of Star CanVac rhexis, the anterior lens capsule was nicked using a 26 G cystotome, and multiple centripetal tears were made in the center to create a small star-shaped opening. A vacuum was used to develop capsulorhexis, and a 25 G flat tip cannula attached to a 5 ml syringe half filled with balanced salt solution (BSS) was used to build capsulorhexis. The piston of the 5 ml syringe was withdrawn to create a vacuum to hold the free capsular flap. It was then directed circularly to get a round capsulorhexis. Oozing liquefied…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
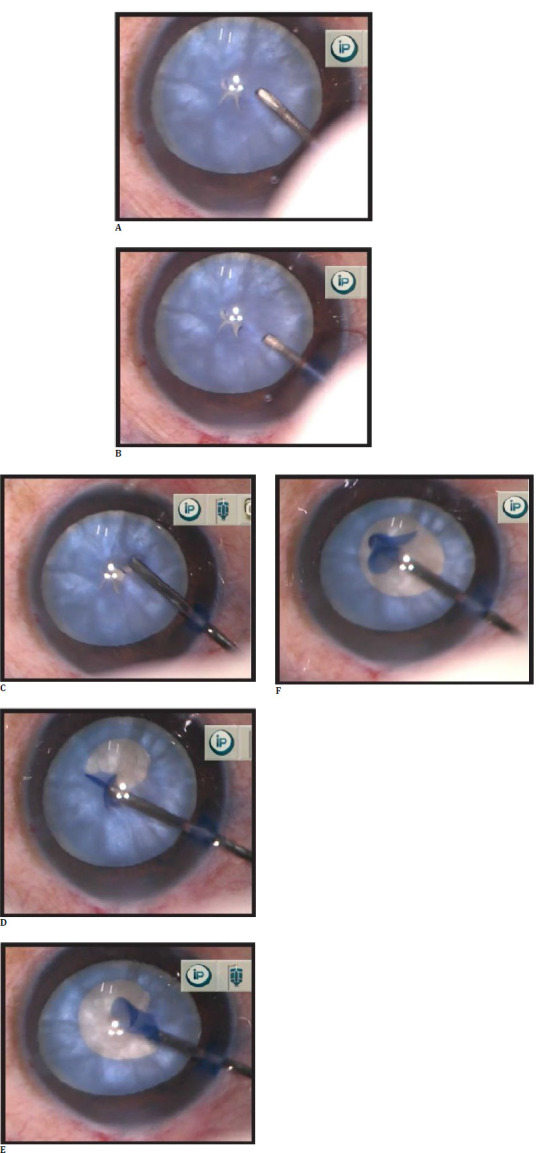 Fig. 1
Fig. 1| Demographic data | Number of patients with mean age and Duration of study |
|---|---|
| Number of patients | 545 |
| Total number of cases | 570 |
| Unilateral: bilateral | 520:25 |
| Male: female | 301:244 |
| Mean age | 51 years (range: 27-76 years) |
| Average follow-up period | 6 months |
| Results | Number of eyes (%) |
|---|---|
|
| |
|
Intumescent cataract Non-intumescent cataract |
442 (77.54%) |
|
| |
|
Phacoemulsification MICS (conversion due to rhexis extension) | 567 (99.47%) |
|
| |
|
Anterior capsular tear Posterior capsular tear Anterior vitrectomy Cystoid macular edema | 6 (1.05%) |
|
| |
|
In capsular bag Sulcus Iris clip IOL | 567 (99.47%) |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsIntraocular Surgery and Lenses · Connexins and lens biology · Ophthalmology and Visual Impairment Studies
Introduction
Cataract surgery has progressed from a vision restorative procedure to refractive surgery. Well-centered capsulorhexis and in-the-bag intraocular lens placement (IOL) are imperative to have good visual outcomes and stabilize the capsular bag during hydro procedures and nucleus and cortex removal. Intumescent cataracts have high intralenticular pressure due to fluid accumulation in a liquefied cortex or viscous cortex, making the anterior capsule tenser. Standard capsulorhexis with 26 G cystotome in such cataracts increases the risk of capsular flap extension to the equator and subsequently to the posterior capsule, resulting in poor outcomes due to complications like vitreous loss, nucleus drop, and aphakia. Any surgical technique that decompresses the intralenticular pressure before propagating the tear decreases the risk of anterior capsular tear. Kodavoor et al. [1] published a new manual technique of Star CanVac continuous curvilinear capsulorhexis (CCC) in the year 2022 for doing capsulorhexis in intumescent cataract using a 26 G cystotome bent at the tip, a 25 G flat-tipped fine cannula connected to a 5 mL syringe half filled with balanced salt solution (BSS). In this study, we analyzed the success of the same technique in an extensive series of total white cataracts.
Methods
Ethics committee approval was obtained, and the study adhered to the tenets of the Declaration of Helsinki. Informed consent was obtained from the patients. The study period was between 2017 and 2023. Patients with mature white cataracts were included in the study. Traumatic cataracts, uveitic cataracts, and eyes with capsular fibrosis or zonular weakness were excluded from the study.
Preoperative cataract workup included complete refraction, intraocular pressure measurement by Goldmann applanation tonometry, comprehensive slit lamp examination (presence of fluid aperture within the lens fibers of the white cataract with corresponding shallow anterior chamber was noted, and white cataracts were classified as intumescent or non-intumescent white total cataract) and B Scan ultrasonography for posterior segment examination. Biometry was performed using IOL Master 700 (Zeiss, Germany) or ultrasound-guided immersion A-scan (Occuscan, RxP, Alcon Laboratories, Inc.) whenever the IOL master could not calculate axial length. IOL power calculation was done using the Barrett Universal II formula.
Preoperatively, the operating eye was dilated with Tropicamide 1.0% and phenylephrine 2.5% eyedrops. A single surgeon performed all the surgeries. Phacoemulsification was performed through a temporal 2.2 mm precise corneal incision under peribulbar anesthesia (using 2.0% Xylocaine and 0.75% Bupivacaine). Two side ports were created using an MVR blade. Under an air bubble, anterior capsular staining was done with trypan blue 0.06% (Auroblue, Aurolabs, India). An ophthalmic viscoelastic device (OVD) was (Appavisc, Appasamy, India) injected to form and deepen the anterior chamber. Sodium hyaluronate 1.4% (Aurogel, Aurolabs, India) flattened the anterior lens capsule wherever required. 26 G bent cystotome needle was used to create five to six small tears over the center of the anterior lens capsule (trim star-shaped configuration) in a centripetal direction. These small star-shaped multiple capsular tears decompress the capsular bag and equally distribute the forces into torn capsular margins to prevent spontaneous, unidirectional, or bidirectional, peripheral extension of capsular tears.
Subsequently, a 25 G flat-tipped cannula attached to a 5 ml syringe half filled with BSS was used to hold free capsular flaps by suction pressure, and a vacuum was created by withdrawing the syringe’s piston. It was maneuvered in a circular motion to get a round capsulorhexis (Fig. 1 A-F). To achieve reasonable control during capsulorhexis, the capsular flap can be grasped and re-grasped several times by releasing the vacuum, which was done by pushing the piston gently. Simultaneously, the loosened and liquified cortex can be aspirated with the same cannula, which aids in better visualization and reduces intracapsular pressure.
A. Intumescent white cataract with anterior lens capsule stained with trypan blue - Multiple small tears are created in the capsule's center in a star-shaped configuration with seepage of milky fluid; B. Anterior chamber filled with OVD; C. One of the flaps is vacuumed with a 25 G flat-tipped cannula; STAR CanVac rhexis is initiated; D. Propagation of star CanVac rhexis in a circular fashion; E. Flap re-grasped whenever needed to continue rhexis; F. Completed STAR CanVac rhexis.
Results
Star CanVac capsulorhexis was carried out in 570 eyes of 545 patients with total white cataracts. Demographic details of study participants and study period are mentioned in Table 1. Among 570 eyes, 442 (77.54%) had an intumescent type, and 128 (22.45%) had nonintumescent mature white cataracts. Of these, unilateral cataract was noted in 520 patients and bilateral in 25 patients, with a male-to-female ratio of 301: 244. The follow-up period was 6 months. Double and triple rhexis were done using utrata/microrhexis forceps in 91 (15.96%) and 12 (2.10%) eyes, respectively. Rhexis enlargement (for irregular, asymmetric rhexis) was required in 44 (7.71%) eyes after IOL implantation to prevent postoperative capsular phimosis.
Table 2 represents the results of the Star Can Vac technique. Except for 6 (1.05%) eyes, all eyes had successful capsulorhexis with this technique. Inadvertent anterior capsular tear happened in these 6 cases with an intumescent type of white cataract. Phacoemulsification was continued and completed carefully with due precautions (slow motion phaco while maintaining chamber stability) in 3 eyes with anterior lens capsule tear. In 3 eyes, we converted it into manual minor incision cataract surgery (SICS), of which 2 (0.35%) eyes had posterior capsular tear with vitreous prolapse. Anterior vitrectomy was done to remove the prolapsed vitreous. A multipiece hydrophobic intraocular lens was placed in the sulcus in two eyes, which had adequate sulcus support, and an iris clip IOL was placed in one eye, which lacked sulcus support. One eye developed cystoid macular edema (CME) in the third month of the postoperative visit, for which an intravitreal dexamethasone implant (cross consultation with Vitreoretinal colleague taken) was given, and CME resolved.
Discussion
Jacobs, Agarwal, et al. [2] reported an incidence of incomplete capsulorhexis in white cataracts, which ranged from 3.85% to 28.3%. Gimbel and associates discovered the shearing and tearing concept in circular curvilinear capsulorhexis in cataract surgery, which became the traditional method in immature cataracts.
Vitreous upthrust was believed to be one of the causes of capsulorhexis extension in intumescent cataracts. Preoperative use of intravenous mannitol was thought to counteract the positive vitreous pressure, even with its use of rhexis extension was reported in many patients. Thus, this hypothesis has no corroboration to support its definitive role in intumescent cataracts. Figueiredo CG et al. [3] postulated the presence of anterior and posterior intralenticular pressure in intumescent cataracts. More fluid accumulated between the posterior capsule and nucleus, which led to high posterior intralenticular pressure and provoked the capsular tear extension during the initiation of rhexis.
Multiple techniques have evolved to tackle the pressure gradient between the anterior chamber and the intralenticular compartment. Cohesive OVD helps to flatten the anterior lens capsule and helps to propagate rhexis in intumescent white cataracts. Nabil KM [4] suggested a lens decompression technique using a 25 G needle to aspirate the liquified cortex by puncturing the center of the anterior lens capsule. Kara-Junior N et al. [5] and Ucar F [6] et al. devised mini rhexis and spiral capsulorhexis in intumescent cataracts. In both these methods, a smaller-sized rhexis was done initially, after which lens decompression was done by removing the cortex. This was followed by enlarging the previously made Mini rhexis for nucleus management. Teng C et al. [7] propounded a phaco capsulotomy technique using a phaco probe to create anterior capsulotomy and lens decompression. Irregular capsular margin, radial extension, wound burn, and zonular weakness were the expected complications from that procedure. In Prasad et al.’s sewing needle capsulotomy technique [8], a unique micro capsulotomy needle produced a smooth round opening instead of a linear cut by a hypodermic needle to prevent the Argentinian flag sign. More advanced technologies like Femtosecond laser-assisted capsulotomy and Zepto precision pulse capsulotomy can be used in intumescent cataracts to achieve precise-sized capsulotomy. Ununiform laser delivery due to leaked fluid, high cost, and limited availability were limitations of those technologies.
Star CanVac capsulotomy is the upgraded version of our technique of CanVac capsulorhexis [9], with the added step of making a star-shaped capsular tear to achieve equal pressure between the anterior chamber and lenticular compartment, which further minimizes the chance of accidental capsular tears. Selecting an appropriate cannula size is essential. A small-sized bore can cause inadequate suction, while a more significant size can cause flap amputation and anterior chamber collapse by removing a large amount of OVD. Considering this, we used a 25 G cannula.
Complete capsulorhexis can be done as a single-staged procedure without coming out of the anterior chamber (this prevents collapse of the anterior chamber and hence rhexis extension). Using the same cannula to visualize the rhexis margin, we can also aspirate the liquefied cortex. Our technique’s advantage is using a readily available instrument like a 25 G cannula, which gives reasonable control during capsulorhexis.
Conclusion
STAR CanVac can be considered a better alternative to conventional capsulorhexis in white cataracts. It takes a few cases to learn, and it can be mastered by every surgeon in any circumstance, both in phacoemulsification and manual SICS.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Kodavoor SK Tamilarasi S Ramamurthy D Ramamurthy C Sachdev GS Star Can Vac-continuous curvilinear capsulorhexis-A novel, safe rhexis technique in intumescent total cataracts Indian Journal of Ophthalmology 2022 May 705180918113550207910.4103/ijo.IJO_2712_21PMC 9333038 · doi ↗ · pubmed ↗
- 2Jacob S Agarwal A Agarwal S Chowdhary S Chowdhary R Bagmar AA Trypan blue as an adjunct for safe phacoemulsification in eyes with white cataract J Cataract Refract Surg 2002281819251238803510.1016/s 0886-3350(01)01316-5 · doi ↗ · pubmed ↗
- 3Figueiredo CG Figueiredo J Figueiredo GB Brazilian technique for prevention of the Argentinean flag sign in white cataract J Cataract Refract Surg 201238153162290644010.1016/j.jcrs.2012.07.002 · doi ↗ · pubmed ↗
- 4Nabil KM Lens decompression technique for prevention of intraoperative complications during phacoemulsification of intumescent cataract Indian J Ophthalmol 2017 Dec 6512143614392920883010.4103/ijo.IJO_352_17PMC 5742978 · doi ↗ · pubmed ↗
- 5Kara-Junior Nde Santhiago MR Kawakami A Carricondo P Hida WT Mini-rhexis for white intumescent cataracts Clinics (Sao Paulo)2009644309121948858710.1590/S 1807-59322009000400007 PMC 2694457 · doi ↗ · pubmed ↗
- 6Ucar F Spiral capsulorhexis technique with anterior chamber maintainer under continuous fluid pressure in intumescent cataracts and its clinical outcomes J Fr Ophtalmol 2022 Nov 459102410303613786610.1016/j.jfo.2022.04.013 · doi ↗ · pubmed ↗
- 7Teng CC Phaco capsulotomy: a technique to prevent the Argentinean Flag Sign Clin Ophthalmol 2017 Nov 611193719402918438210.2147/OPTH.S 138676 PMC 5685091 · doi ↗ · pubmed ↗
- 8Prasad R Badhani A Dogra G Morya A Sewing needle microcapsulotomy to avert Argentinian flag sign J Cataract Refract Surg 2021 Nov 14711 e 24e 283327823310.1097/j.jcrs.0000000000000531 · doi ↗ · pubmed ↗