Assessing and Enhancing Nutrition and Physical Activity Environments in Early Childhood Education and Care Centers: Scoping Review of eHealth Tools
Joyce Hayek, Kelsi Dickson, Lynne M Z Lafave

TL;DR
This review maps eHealth tools used in early childhood education to improve nutrition and physical activity, finding mostly web-based tools with a need for better testing.
Contribution
The study provides the first comprehensive scoping review of eHealth tools for nutrition and physical activity in early childhood education settings.
Findings
Most eHealth tools identified were web-based and focused on nutrition.
Few tools addressed both nutrition and physical activity simultaneously.
Psychometric testing and long-term effectiveness of these tools remain insufficiently evaluated.
Abstract
Early childhood is a critical period for shaping lifelong health behaviors, making early childhood education and care (ECEC) environments ideal for implementing nutrition and physical activity interventions. eHealth tools are increasingly utilized in ECEC settings due to their accessibility, scalability, and cost-effectiveness, demonstrating promise in enhancing educators’ practices. Despite the potential effectiveness of these eHealth approaches, a comprehensive collection of available evidence on eHealth tools designed to assess or support best practices for nutrition or physical activity in ECECs is currently lacking. The primary objective of this scoping review is to map the range of available eHealth tools designed to assess or deliver interventions aimed at improving nutrition or physical activity in ECEC settings, while evaluating their components, theoretical foundations, and…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
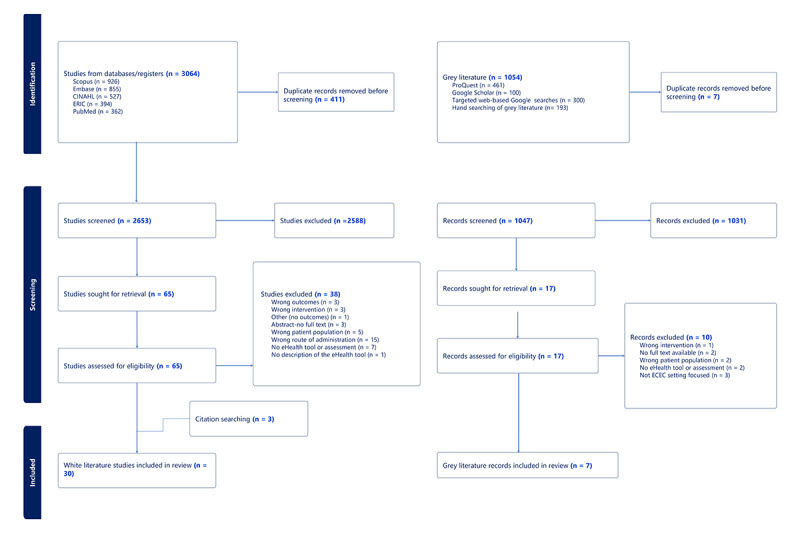 Figure 1
Figure 1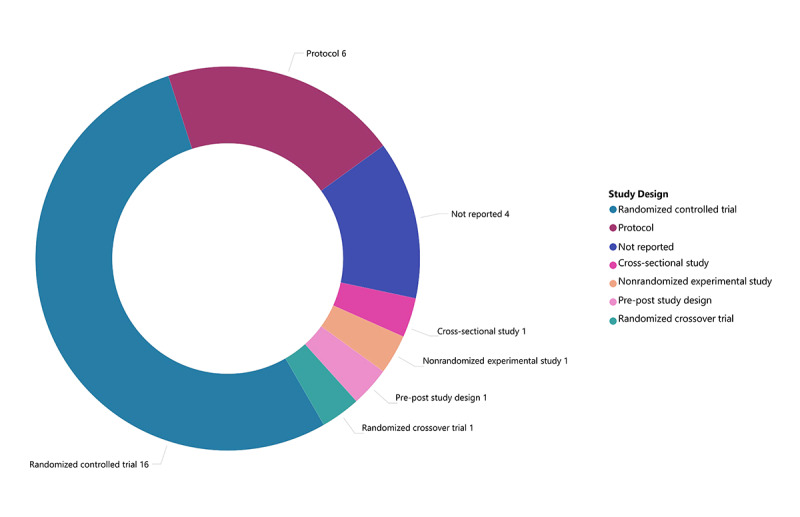 Figure 2
Figure 2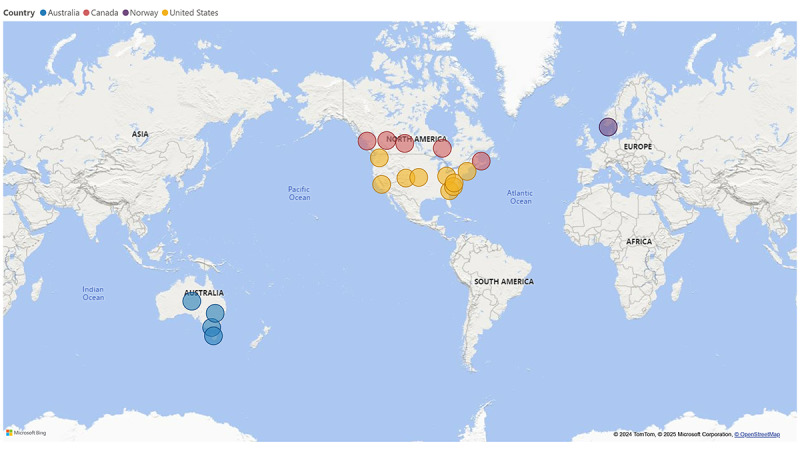 Figure 3
Figure 3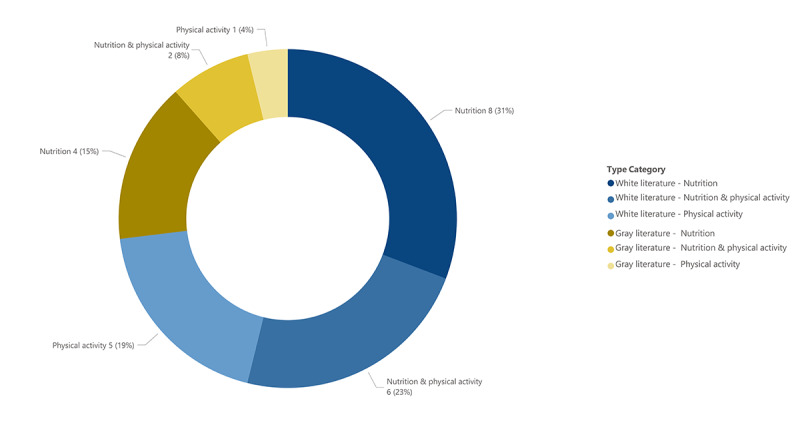 Figure 4
Figure 4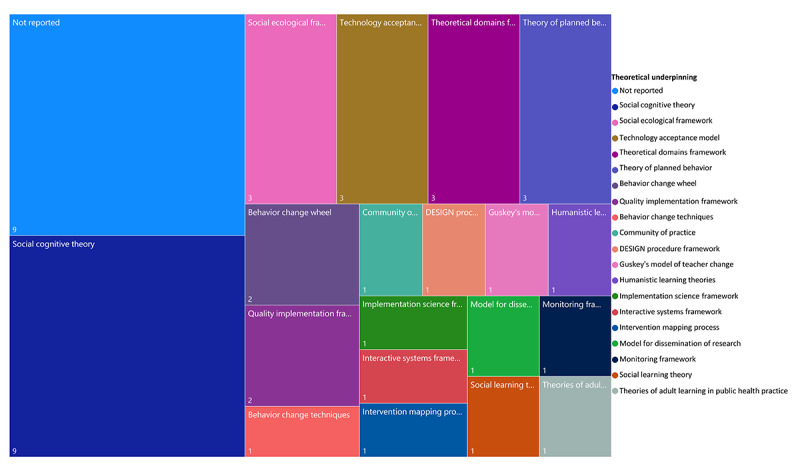 Figure 5
Figure 5| Reference: country | Study design | Study setting | Sample size (at baseline) | Sex of overall participants (% of females) | Participant age (years), mean (SD) | Nutrition or PAa outcome measures |
| Barnes et al [ | RCTb | Childcare centers | NRc | NR | NR | •Improving implementation of targeted healthy eating practices. |
| Barnes et al [ | RCT | Childcare centers | Total: 22 (intervention: 11; control: 11) | NR | Intervention group: supervisors 37.68 (5.92) and center champions 44.17 (6.40); control group: supervisors: 43.91 (10.57) | • Implementation of targeted healthy eating practices. |
| Blomkvist et al [ | Protocol for RCT | Kindergarten | Total: 46 kindergartens (intervention: 31; control: 15) | NR | NR | • Primary outcomes: (1) child vegetable intake; (2) children’s level of food neophobia; and (3) child dietary habits and food variety. |
| Blomkvist et al [ | RCT | Kindergarten | Total: 46 kindergartens (intervention: 31; control: 15) | NR | NR | •Child intake of intervention vegetables and all vegetables combined. |
| Bruijnsd,e et al [ | Pre-post study design | Center-based childcare, kindergarten, and preschool | Total: 110 early childhood educators | 99.2% | 37.1 (9.5) | •Knowledge of PA, outdoor/risky play, and sedentary behavior concepts. |
| Brussoni et al [ | Protocol for RCT | ELCCf | Total: 324 ECEsg and ELCC administrators | NR | NR | •The primary outcome is increased tolerance of risk in children’s play, as measured by the Teacher Tolerance of Risk in Play Scale. |
| Brussoni et al [ | RCT | ELCC | Total: 563 educators and administrators (intervention: 281; control: 282) | 96.6% | NR | •Primary outcome: change in the total score on the T-TRiPSh. |
| Chuang et al [ | RCT | ECE centers | Total: 111 ECE providers (intervention: 56; control: 55) | 97.3% | 43.55 (11.87) | • Psychosocial and behavioral measures: (1) nutrition knowledge, (2) mindful eating, (3) perceived barriers to eating fruits and vegetables, and (4) perceived barriers to promote healthy eating in classroom. |
| Clark et al [ | NR | Licensed childcare | Total: 38 childcare providers (intervention: 23; control: 15) | 100% | NR | • Knowledge of and attitudes and behaviors toward feeding breast milk, formula, and solid food to the infants in their care. |
| Clarke et al [ | Protocol | ECE programs | Total: 2932 ECE providers | N/Ai | N/A | • Uptake and perceived usefulness of on-demand online nutrition training. |
| Grady et al [ | Nonrandomized experimental study | Long day care services | Total: 46 childcare services (intervention: 27; control: 19) | NR | Intervention group: 48.44 (10.36); control group: 43.74 (10.48) | • Uptake and use of the menu program: proportion of services adopting the program and proportion of services using the program as intended. |
| Grady et al [ | RCT | Long day care services | Total: 54 childcare services (intervention: 27; control: 27) | NR | Intervention group: 48.4 (10.4); control group 44.9 (10.5) | • Primary outcome: the mean number of food groups compliant with dietary guidelines |
| Green et al [ | NR | Long day care, preschool, and occasional care | NR | NR | NR | • Nutrition practice achievements such as (1) lunch boxes monitored daily and (2) fruits and vegetables on menu. |
| Hazard et al [ | RCT | Licensed childcare centers | Total: 20 childcare providers | 98% | NR | • Evaluation of accessibility, acceptability, and satisfaction of nutrition and online education courses. |
| Hoffman et al [ | RCT | Preschools | Total: 11 teachers and 2 site supervisors | NR | NR | • Implementation fidelity, acceptability, and feasibility of WE PLAYj. |
| Hoffman et al [ | RCT | Preschools | Total: 25 teachers (intervention: 11; control: 14) | 100% | Intervention group 40.7 (9.0); control group 45.9 (13.2) | • Children’s MVPAk (MVPA accelerometer). |
| Kempler et al [ | Cross-sectional study | Childcare services | Total: 64 participants | NR | NR | • Qualitative outcomes explored use and experience with the menu tool. |
| Kennedy et al [ | NR | Preschools | Total: 41 teachers | NR | NR | •The percentage of the 60-minute daily goal reached in each classroom. |
| Lafave [ | Randomized crossover trial design | ECECl centers | Total: 72 educators | 100% | NR | • Psychometric evaluation of nutrition and PA assessment—online inter- and intrarater reliability. |
| Lafave et al [ | Protocol for quasi-experimental study | ECEC centers | Total: 208 educators (intervention: 138; control: 50) | 96.2% | 40.05 (11.67) | •Food served in the center self-audit, eating environment/mealtime practices self-audit, nutrition education programming self-audit. |
| Lee et al [ | RCT | Licensed childcare centers | Total: 30 ECE or services (intervention: 19; control: 11) | NR | Intervention group 47.7 (10.8); control group 49.6 (12. | • Knowledge and awareness of and adherence to California’s 2010 Healthy Beverages in Child Care Act. |
| Peden et al [ | RCT | ECEC centers | Total: 104 educators | 85% | NR | • Qualitative educator comments on the experience of the HOPPELm program. |
| Peden et al [ | RCT | ECEC centers | Total: 112 educators | 85% | NR | •Changes in center-level healthy eating practices assessed using the EPAOn tool. |
| Reilly et al [ | RCT | ECEC services | Total: 1024 ECEC services (intervention: 684; control: 342) | NR | NR | •Intentions to adopt the guidelines. |
| Saunders et al [ | NR | Preschools | Total: 818 teachers | NR | NR | • Classroom implementation completeness (ie, provision of 300 minutes of PA opportunities) and fidelity (ie, achieving PA fidelity and social environment fidelity). |
| Ward et al [ | RCT | Full-time and part-time childcare center programs | Total: 33 ECE centers (intervention: 18; control: 15) | NR | NR | • Change in centers’ nutrition environments: (1) foods provided, (2) beverages provided, (3) feeding environment, (4) feeding practices, (5) menus, (6) education and professional development, and (7) nutrition policy. |
| Ward et al [ | RCT | Early childcare centers | Total: 191 (intervention: 102; control: 89) | NR | NR | •Healthy eating practices. |
| Willis et al [ | Protocol for RCT | ECE centers | Total: 168 teachers | N/A | N/A | •Children’s dietary intakes and Healthy Eating Index scores. |
| Yoong et al [ | Protocol for RCT | Childcare services | Total: 54 long-day-care services | N/A | N/A | •Mean number of food groups on childcare service menus that comply with dietary guidelines. |
| Yoong et al [ | RCT | Childcare centers | Total: 35 childcare centers | NR | NR | •Number of servings of the 5 core and discretionary food groups defined by the Australian Guide to Healthy Eating consumed in care. |
| eHealth tool | Country: References | Type of eHealth tool | eHealth modalitya | Target of eHealth tool | eHealth tool component | eHealth tool description | Length of the intervention | Theoretical underpinning |
| Create Healthy Futures Program | United States: [ | Intervention | Web based | Nutrition | Healthy eating practices | Self-paced web-based intervention on promoting healthy eating behaviors for ECEb providers | 6 weeks | •Social Cognitive Theory |
| CHEERSc | Canada: [ | Assessment and intervention | Web based | Nutrition and physical activity | Nutrition and physical activity practices | Online educational modules and communities of practice to improve the nutrition and physical activity environment in ECECsd | 10 months | •Social Cognitive Theory |
| EATSe | Australia: [ | Assessment and intervention | Web based | Nutrition | Healthy eating practices | The web-based program supports center implementation of targeted healthy eating practices through self-assessment, feedback, and the development of an action plan | 6 months | •Social Ecological Framework |
| FoodChecker | Australia: Kempler et al [ | Assessment and intervention | Web based | Nutrition | Online menu planning | Web-based menu planning tool to support childcare services in planning healthy menus | NRf | NR |
| feedAustralia | Australia: [ | Assessment and intervention | Web based | Nutrition | Online menu planning | Web-based menu planning program offering automated real-time assessment of childcare menu with feedback to support the planning of healthier menus | 12 months | •Technology Acceptance Model |
| GO NAPSACCg | United States: [ | Assessment and intervention | Web based | Nutrition and physical activity | Nutrition and physical activity practices | Suite of online tools to guide ECE programs through a 5-step process to improve their nutrition and physical activity-related practices, including (1) self-assessment, (2) goal setting and action planning, (3) implementation, (4) education and training, and (5) reassessment | 4 months | •Social Cognitive Theory |
| GO NAPSACC Cares | United States: [ | Assessment and intervention | Web based | Nutrition and physical activity | Nutrition and physical activity practices (center level) + educator’s personal diet and physical activity | The traditional GO NAPSACC program and embedded Staff Wellness website that focus on ECE personal healthy behavior change strategies including healthy eating, increased physical activity, and weight management | 6 months | •Social Cognitive Theory |
| HOPPELi | Australia: [ | Intervention | Web based | Nutrition and physical activity | Nutrition and physical activity practices | Synchronous and asynchronous online professional development to promote physical activity and healthy eating | 12 weeks | •Community of Practice |
| Healthy Start-Départ Santé | Canada: [ | Intervention | Web based | Nutrition and physical activity | Nutrition and physical activity practices | Online modules to improve healthy eating and physical activity practices | 4 hours | NR |
| InfaNET | United States: [ | Intervention | Web based | Nutrition | Infant feeding practices | Bilingual (English and Spanish) website with childcare-specific infant feeding information | 3 months | •Social Learning Theory |
| Munch & Move | Australia: [ | Intervention | Web based | Nutrition and physical activity | Nutrition and physical activity practices | Professional development training for early childhood educators to support healthy eating and physical activity habits in young children | NR | •The Monitoring Framework |
| OutsidePlay-ECE risk-reframing intervention | Canada: [ | Intervention | Web based | Physical activity | Outdoor/risky play | Fully automated web-based intervention to reframe ECEs’ perception of the importance of outdoor play and its inherent risks and promote a change in their practice in supporting children’s outdoor play in ELCCj settings | Up to 100 minutes | •Intervention mapping process |
| Online training on healthy beverage best practices | United States: [ | Intervention | Web based | Nutrition | Healthy beverage practices | Self-paced online modules (English and Spanish) on healthy beverage best practices for childcare providers | English (29-minutes); Spanish (37-minutes) | NR |
| Online training on healthy beverage policy | United States: [ | Intervention | Web based | Nutrition | Healthy beverage practices | Bilingual (English or Spanish) self-paced on-demand online training to increase knowledge and adherence of childcare providers to healthy beverage practices | 30-minutes for the online training (+ with or without 6 months of online technical assistance) | •Implementation Science Framework |
| Online training to disseminate outdoor free-play information in relation to COVID-19 guidelines | Australia: [ | Intervention | Web based | Physical activity | Outdoor/risky play | e-newsletter or animated video to increase ECEC service intentions to adopt an indoor-outdoor program for the full day and offer more time outdoors | e-newsletter (3 minutes); video (3.5 minutes) | •Model for Dissemination of Research |
| SHAPES-Dk | United States: [ | Assessment and intervention | Web based | Physical activity | Physical activity practices | Self-assessment and online training modules to improve instructional physical activity practices and classroom social environment | 12 weeks | NR |
| Tool to increase children’s vegetable intake and reduce food neophobia | Norway: [ | Intervention | Web based | Nutrition | Online menu planning and feeding practices | Access to online menu recipes to include vegetables each week, with or without pedagogical tools (sensory lessons, meal practice, and feeding practices recommendations) | 3 months | NR |
| TEACHl e‐learning course | Canada: [ | Intervention | Web based | Physical activity | Physical activity and sedentary behavior | e-Learning course in physical activity and sedentary behavior comprising 4 modules | 2 weeks | •Social Cognitive Theory |
| WE PLAYm | United States: [ | Intervention | Web based | Physical activity | Physical activity practices | Online asynchronous modules to promote physical activity | 4 weeks | Social Cognitive Theory |
| Online training on healthy beverage policy | United States: [ | Intervention | Web based | Nutrition | Healthy beverage practices | Bilingual (English or Spanish) self-paced on-demand online training to increase knowledge and adherence of childcare providers to healthy beverage practices | 30 minutes for the online training (+ with or without 6 months of online technical assistance) | Implementation Science Framework |
| eHealth tool | Author/organization | Country: year | Participant information | Type of eHealth tool | eHealth modalitya | Target of eHealth tool | eHealth tool description | Length of intervention |
| A Balanced Day: Tips and Guideline for Child Care Providers | Hastings Prince Edward Public Health | Canada: NRb | Childcare providers | Intervention | Web based | Physical activity | Online interactive modules (videos) on physical activity, sedentary behavior, sleep, and health messages for caregivers. | 15 minutes |
| Boston Healthy Childcare Initiative | The Boston Public Health Commission | United States: NR | Early childhood educators | Intervention | Web based | Nutrition and physical Activity | Online training on evidence-based nutrition and physical activity best practices in early learning environments. | NR |
| Child Care Healthy Eating and Active Living Guidelines Training | Ottawa Public Health | Canada: 2015 | Supervisors, childcare providers, and municipal cooks | Intervention | Web based | Nutrition and physical activity | Online training modules on healthy eating practices, environments, and physical literacy. | Part 1: Nutrition: 60 minutes; part 2: Active living: 30 minutes |
| Fostering Healthy Eating Habits | BC Provincial Health Services Authority—Interior Health | Canada: 2016 | Childcare providers | Intervention | Web based | Nutrition | e-Learning course on healthy practices and environment. | 1 hour |
| MyPlate on Alexa | United States Department of Agriculture | United States: 2020-2025 | Everyone from parents and caregivers of babies starting at 4 months old through older adults (includes early learning professionals) | Intervention | App | Nutrition | An app that provides food and nutrition tips based on the Dietary Guidelines for Americans. | N/Ac |
| Nourished and Active in Early Learning | University of Washington’s Center for Public Health Nutrition and Washington State Department of Health | United States: NR | Early learning professionals | Intervention | Web based | Nutrition | Online course on healthy eating and beverages comprising 6 modules, strategies to support healthy eating, and common challenges. | NR |
| Nourishing Beginnings | Dairy Farmers of Canada | Canada: NR | ELCCd educators and directors as well as ELCC professors or program directors at colleges or universities. | Intervention | Web based | Nutrition | Online modules on healthy feeding practices | Module 1: 80 minutes; module 2: 70 minutes |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMobile Health and mHealth Applications · Obesity, Physical Activity, Diet · Child and Adolescent Health
Introduction
Background
Unhealthy lifestyle factors, such as physical inactivity and unhealthy diets, are primary contributors to the rising incidence of chronic diseases [1-5]. These conditions are recognized as growing global public health problems, leading to significant treatment costs and imposing an economic burden on health systems, individuals, and society as a whole [6,7]. Health behaviors often originate in early childhood and can persist into young adulthood [8]. Research indicates that health behaviors, such as eating habits and physical activity levels, are modifiable risk factors for obesity and chronic diseases [9]. These behaviors often co-occur or cluster together [10,11]. An integrated approach to health promotion, addressing both dietary intake and physical activity simultaneously [10], is therefore essential during early childhood to improve population health across the lifespan.
The early years are a critical period for shaping health behaviors and outcomes [12], with early interventions regarded as an essential component of preventive health [13]. Early childhood education and care (ECEC) settings provide a unique opportunity to reach a large number of children during this pivotal developmental period, making them an ideal setting for behavioral interventions [12,14]. Moreover, early childhood educators, as part of the ECEC environment, are well-positioned to successfully implement nutrition and physical activity behavior interventions [15,16]. Evidence from prior research shows that professional training of early childhood educators in best practices for nutrition and physical activity is associated with improved dietary intake and increased physical activity levels in young children [17-20].
With the widespread use of the internet, online or eHealth interventions have experienced significant growth. eHealth refers to the use of digital technologies, such as the internet, digital gaming, virtual reality, and robotics, for promoting, preventing, treating, and maintaining health [21]. Examples of eHealth technologies include smartphone apps, websites, computer programs, SMS text messaging, and social media platforms [22]. Digital technologies offer several advantages, including lower costs, reduced participant burden, enhanced accessibility, and increased scalability, thereby extending the reach of behavioral interventions [23,24]. Prior research indicates that eHealth interventions within ECEC settings are highly acceptable and effective in improving early childhood educators’ knowledge and practices related to nutrition and physical activity [25-27].
Behavior change theories can guide the selection of intrapersonal constructs to target in intervention development, as well as the choice of behavior change techniques to achieve desired behavioral outcomes [28]. Evidence suggests that behavior change interventions, whether internet-based or not, are more effective when guided by a theoretical framework [29]. A meta-analysis [29] found that interventions extensively informed by theory demonstrated larger effects compared with those lacking theoretical underpinnings. The use of theory not only enhances the efficacy of interventions but also facilitates their replication and future development [30]. Consequently, it is crucial to determine whether theory has been applied in the development of eHealth tools.
Recognizing the importance of early learning settings and educators in fostering healthy behavior development in children, researchers have developed, implemented, and evaluated health promotion interventions within childcare settings [31-33]. A preliminary search of PROSPERO, PubMed, the Cochrane Database of Systematic Reviews, and JBI Evidence Synthesis identified several relevant reviews. However, these reviews primarily focused on evaluating the effectiveness of in-person nutrition and physical activity interventions [34,35], interventions conducted in family-based centers [36,37], or those targeting older children and adolescents [33]. No current or in-progress systematic or scoping reviews address eHealth tools for promoting the best nutrition and physical activity practices in ECEC settings.
Objectives
To address this gap in the literature, we conducted a scoping review. This method is used to identify the types of available evidence in a field, explore key characteristics related to a concept, and analyze knowledge gaps [38]. This review aimed to achieve the following objectives: (1) identify existing eHealth tools used to assess or deliver interventions that improve nutrition or physical activity environments in ECEC centers; (2) describe the components of the eHealth tools, including technology type (eg, websites, smartphone apps, social media) and health purposes (eg, nutrition evaluation, physical activity promotion); (3) outline the psychometric properties of the eHealth tools, when applicable; (4) report the theoretical foundations used in developing the eHealth tools; and (5) identify any evidence gaps. The purpose of this study was to map the available evidence on eHealth tools currently used to assess and support best practices for nutrition or physical activity in ECEC centers.
Methods
Overview
This scoping review followed established methods for such studies [39] and adhered to the PRISMA-ScR (Preferred Reporting Items for Systematic Reviews and Meta-Analyses Extension for Scoping Reviews) guidelines [40]. Methodological quality or risk of bias was not assessed, as the goal of this review was to provide a broad overview of existing evidence, regardless of methodological approach, to map the available evidence. This is consistent with guidance on scoping review methods [39]. Full details of the methods can be found in our published protocol [41]. The PRISMA-ScR checklist is included in Multimedia Appendix 1 [40].
Selection Criteria
Participants
This review considered studies involving early childhood educators within licensed ECEC programs, whether public or privately operated, providing full-day care for children aged 0-5 years. Studies focusing on educators in family-based settings, preschool programs where children attend for less than 4 hours per day, or before- and after-school care were excluded.
Concept
This review considered studies that explored eHealth tools designed to support nutrition or physical activity environments in the ECEC setting. eHealth tools were defined as digital technologies that (1) assessed or (2) delivered interventions to improve nutrition or physical activity environments and practices. eHealth tools that assessed the ECEC environment were included only if they provided feedback to the ECECs. Additionally, we included only studies where the eHealth tool was the primary component for assessment or intervention.
Context
This review focused on nutrition and physical activity environments in the ECEC setting, considering both the physical and social environments.
Types of Sources
For this scoping review, we considered all study designs, including quantitative, qualitative, mixed methods, protocols, experimental, quasi-experimental, and cross-sectional studies. Systematic reviews and meta-analyses were also included if relevant to the topic, with a primary focus on ECEC settings. Unpublished studies and gray literature were also considered as sources of information.
Search Strategy
Overview
The search strategy was developed in collaboration with 2 research librarians and aimed to capture both white and gray literature to encompass the full range of available eHealth tools.
White Literature
A preliminary limited search of PubMed and Scopus was conducted to identify articles on the topic. The text words in the title and abstract, along with the index terms used to describe the articles, were analyzed to develop a full search strategy for PubMed. This search strategy, incorporating all identified keywords and index terms, was then adapted for each included information source (see Multimedia Appendix 2). The databases searched included PubMed, Scopus, CINAHL Plus (EBSCOhost), ERIC (EBSCOhost), and Embase (OVID). The reference lists of all included sources of evidence were screened for additional white literature. The final search was conducted on October 4, 2023. For each database, a search alert was set up using its alert functions to track any new relevant publications for potential inclusion in the review. The final search alert was reviewed on May 5, 2024, and only 1 additional study was identified. All retrieved white literature was exported into Covidence software (Veritas Health Innovation) for screening and data extraction.
Gray Literature
Following the guidelines outlined by Godin et al [100], we conducted a thorough search of the gray literature to identify nonindexed sources such as dissertation abstracts, government documents, conference proceedings, educational materials, and reports. This was done through searches in (1) the ProQuest Database, (2) Google Scholar, (3) targeted web-based Google searches, and (4) hand searches of the reference lists of all included gray literature to identify additional relevant sources. The final gray literature search was conducted on April 30, 2024. All retrieved documents were exported into Microsoft Excel and assigned a unique identifier for screening and data extraction. Because of the potential volume of gray literature, we limited our review to the first 10 pages from Google Scholar and targeted web-based Google searches, based on title. Additionally, eHealth tools that required payment for access were excluded.
This review included studies and records published in English or French, with no date limitations.
Study Selection
Following the search, all identified records were uploaded into Covidence (for white literature) or Microsoft Excel (for gray literature). Title and abstract screening, full-text screening, and data extraction were performed by 2 independent reviewers (JH and LMZL) according to the inclusion criteria. Reasons for excluding full texts that did not meet the inclusion criteria were recorded and reported in the scoping review. Any disagreements between the 2 reviewers were resolved through discussion, and if consensus could not be reached, a third reviewer (KD) was consulted. The results of the search are reported and presented in a PRISMA-ScR flow diagram (Figure 1 in Results section).
Data Extraction
Separate data extraction charting tools for white and gray literature were developed by the reviewers (Multimedia Appendix 3), as outlined in our published protocol [41]. The extraction tools, used to capture relevant study and eHealth tool characteristics, were piloted before the review to ensure consistency in information collection. Any disagreements between reviewers were resolved through discussion.
Data Analysis and Presentation
The extracted data were summarized using descriptive statistics (ie, frequency counts). The results were organized by each review question, highlighting study characteristics, eHealth tool characteristics, and the use of a theoretical framework. The findings are presented in a narrative summary, complemented by tables, charts, and illustrations.
Results
Literature Search and Selection Process
The white literature search yielded 3064 results, of which 411 were removed as duplicates. Titles and abstracts for 2653 records were screened for eligibility, and 2588 were excluded. Of the remaining records, 65 full-text articles were reviewed against the eligibility criteria. A total of 30 articles were included for data extraction (Figure 1). The gray literature search yielded 1054 results, of which 7 were removed as duplicates. Titles and abstracts of 1047 records were assessed against the eligibility criteria, and 17 were moved to full-text screening. Of these, 7 met the inclusion criteria and were included in the analysis. The PRISMA flowchart shows the selection process.
PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) flowchart.
Included Records
A total of 30 research studies identified in the white literature were included in this review (Figure 1). Of these, 16 were randomized controlled trials, 6 were protocol studies, 1 was a cross-sectional study, 1 was a nonrandomized experimental study, and 1 was a randomized crossover control trial (Figure 2). Specific characteristics of the included studies are presented in Table 1, which reflects the study design, setting, and outcome measures. The study aims along with additional study details are provided in Multimedia Appendix 4. The largest proportion of studies were conducted in the United States (n=11, 37%) and Australia (n=11, 37%), followed by Canada (n=6, 20%) and Norway (n=2, 7%; Figure 3). The studies were conducted between 2016 and 2022. The baseline sample size ranged from n=13 to 2932. Of the 10 studies reporting participant sex, females comprised the largest proportion of participants ranging from 85% to 100%, with an average of 96% (Table 1). The mean age of participants ranged from 37.1 to 49.6 years.
A total of 7 records were identified in the gray literature and included in this review (Figure 1). These records represented community-based eHealth outreach initiatives related to nutrition or physical activity support for the ECEC community. Four of these initiatives originated from Canada and 3 from the United States.
Study designs of research articles identified in the white literature.
Country of study from eHealth research identified in the white literature and gray literature.
eHealth Tool Characteristics
The 30 research articles included in the review identified 19 unique eHealth tools, with 12 categorized as intervention-based and 7 as both assessment and intervention tools. The characteristics of these eHealth tools identified in the white literature are summarized in Table 2, with additional details available in Multimedia Appendix 4. Among the 7 eHealth tools incorporating an assessment component, only 1 underwent evaluation of its psychometric properties. All eHealth tools were delivered via a web-based modality (7/7, 100%).
The characteristics of the eHealth tools identified in the gray literature are summarized in Table 3, with additional details provided in Multimedia Appendix 5. Of the 7 eHealth tools identified, all were intervention-only tools (7/7, 100%). Of these, 6 (86%) were delivered via a web-based modality, while 1 (14%) was delivered as a mobile phone app.
Practices Targeted
The majority of eHealth tools identified in the white literature (8/19, 42%) targeted nutrition practices, 6 of 19 (32%) targeted both nutrition and physical activity, and 5 of 19 (26%) exclusively addressed physical activity (Figure 4). The duration of intervention implementation ranged from 3 minutes to 12 months. The majority of eHealth tools identified in the gray literature targeted nutrition (4/7, 57%), followed by tools targeting both nutrition and physical activity (2/7, 29%), and 1 focused solely on physical activity (Figure 4). For both the white (Table 2) and gray literature (Table 3), eHealth intervention tools targeting nutrition primarily addressed best nutrition and feeding practices, healthy eating or beverage practices, and menu planning. eHealth tools targeting physical activity mainly focused on best physical activity practices, outdoor play, and the reduction of sedentary behaviors.
Target of eHealth tool for white and grey literature.
Theoretical Framework of the eHealth Tools
Of the 30 research studies identified in the white literature, 21 reported the use of theoretical models (Multimedia Appendix 4). The most commonly cited theories include Social Cognitive Theory, Social Ecological Model, Theoretical Domain Framework, Theory of Planned Behavior, Behavior Change Wheel, and Quality Implementation Framework (Figure 5). None of the eHealth tools identified in the gray literature reported a theoretical underpinning (see Multimedia Appendix 5).
Theoretical underpinning from studies identified in the white literature search. DESIGN: decide target behavior, explore determinants, select theory-based model, indicate objectives, generate education plans, and nail down the evaluation.
Discussion
Principal Findings
The purpose of this scoping review was to explore the available eHealth tools developed to assess or deliver interventions aimed at improving the nutrition or physical activity environments in ECEC settings. The results of this review provide insights into the digital tools available, outlining their methodological approach and characteristics.
Mapping the included white and gray literature identified 26 eHealth tools, highlighting a growing interest in leveraging digital tools to enhance nutrition and physical environments in early learning settings. Notably, all tools were web based except for 1 delivered via a smart device application. This finding is striking, given the widespread adoption of mobile health apps in health promotion interventions [69,70]. A likely explanation is that the nature and timing of the intervention may influence the choice of eHealth modality. Mobile apps are typically utilized in interventions requiring rapidly changing data and real-time feedback, such as step tracking or patient self-care and symptom management [71,72]. By contrast, interventions targeting nutrition and physical activity practices in educational settings often focus on gradual changes implemented over extended periods. Additionally, mobile apps are generally more expensive to develop and maintain than web-based tools and require regular updates [73]. Furthermore, most educational settings rely on web-based systems and have access to computers and the internet, making web-based platforms a more convenient option for educators while facilitating the implementation of interventions. Lastly, mobile-based interventions are often more prevalent among youth populations (children and adolescents) due to their capacity to incorporate gamification—a popular and engaging approach for health promotion interventions within this demographic [74].
The identified eHealth tools employed diverse approaches and strategies to enhance nutrition and physical activity practices. Most tools focused on professional development, offering online modules and self-paced training with both synchronous and asynchronous components to improve educators’ knowledge and behaviors related to best practices in nutrition and physical activity. Most of these tools (21/26, 81%) included educational videos to create engaging and interactive content, while just over half (15/26, 58%) incorporated quizzes or evaluation questions to reinforce learning and assess understanding. Additionally, a smaller proportion (10/26, 38%) provided technical support from experts or facilitators to offer guidance and enhance educator engagement. Research suggests that such human support can improve compliance and foster the adoption of new behaviors [75,76]. However, relying on human support may not be a sustainable approach due to the significant resources required and the challenges it poses for scalability [77]. A smaller proportion of tools (3/26, 12%) emphasized menu planning and provided tailored support to aid in the creation of healthier menus. Tools targeting physical activity primarily addressed best practices, highlighted the importance of outdoor and risky play, and aimed to reduce sedentary behaviors. Nutrition-focused tools concentrated on promoting best practices for nutrition and feeding while optimizing eating environments.
Less than one-third (8/26, 31%) of the identified eHealth tools addressed both nutrition and physical activity together. Evidence suggests that multibehavior interventions, which target multiple health behaviors simultaneously, are often more effective in driving meaningful change compared with interventions focused on a single behavior [78]. Given the interconnected nature of nutrition and physical activity, these behaviors play a crucial role in health and well-being [79,80] and are recognized as leading modifiable factors in the prevention of major chronic diseases [1,2]. Knowing that nutrition and physical activity tend to cluster together, addressing these behaviors collectively might enhance the effectiveness of interventions [11,81-84]. It has also been found that targeting both nutrition and physical activity behaviors can lead to synergistic effects on health outcomes [85-87]. Therefore, tools aimed at improving educators’ nutrition and physical activity practices or the nutrition and physical activity environments in early learning centers should target determinants of both behaviors simultaneously.
Another key finding is that, among the 7 eHealth tools incorporating an assessment component, only 1 reported psychometric properties testing. Psychometric evaluations, such as reliability and validity testing, are crucial as they indicate the quality of the tools, ensure their effectiveness for the intended purpose, and support their reproducibility and replicability [88]. The lack of reported psychometric testing may be due to some tools originally being developed in a pen-and-paper format before being adapted to an online format. In the original articles describing the pen-and-paper versions, psychometric testing was reported [89]. However, it is important to recognize that tool validity and reliability are not static characteristics; rather, they are assessments of the tool’s instrument scores within the context in which they have been evaluated [90]. It is therefore recommended to conduct and report updated psychometric testing when tools are adapted into digital formats to ensure that the validity and reliability of the results are maintained [91,92].
Among the 30 studies identified in the white literature, the majority (21/30, 70%) incorporated a theoretical framework in their design. The most frequently cited theory was the Social Cognitive Theory, which is commonly used in behavior change interventions, aligning with findings from other reviews [93-95]. A theoretical underpinning is a critical consideration when developing health promotion interventions. It serves as a blueprint for the study, structuring and guiding the intervention planning process, and also helps in understanding the factors that might influence behavior change and need to be targeted [96,97]. Previous reviews have indicated that health interventions grounded in theory are more effective [28] and are associated with positive significant outcomes, larger effect sizes [23,94,98], and the maintenance of behavior change [99]. Hence, future research designing eHealth tools should prioritize the use of theoretical underpinnings to increase effectiveness and ensure replicability. Regarding the gray literature findings, no reports on the theoretical underpinnings or reliability were identified for any of these tools. A possible reason for this could be that the gray literature often targets a general population audience, where the focus is on practical application, whereas in peer-reviewed literature, researchers look for evidence of theoretical grounding to evaluate and further refine or replicate these tools.
Implications/Recommendations
Future research involving the development and implementation of eHealth tools in ECEC settings should emphasize the integration of theoretical frameworks, consider comprehensive multibehavior intervention approaches, incorporate community perspectives in the development process, and prioritize long-term sustainability and scalability, with a focus on implementation and efficacy assessment. Theoretical frameworks provide essential guidance in identifying key determinants of behavior and mechanisms for promoting change. Incorporating theory can enhance the effectiveness of eHealth tools, ensure consistent implementation, and facilitate replicability across different contexts. Multipronged eHealth tools designed to target both nutrition and physical activity can lead to more beneficial outcomes, as these domains are interconnected. To enhance implementation and adoption, it is essential to involve a diverse range of stakeholders, such as educators, parents, and health professionals, in the development process. This ensures that the unique needs and cultural context of the targeted eHealth tool users are addressed. Additionally, researchers should prioritize long-term sustainability and scalability when designing these tools, ensuring that interventions can be maintained and expanded across various settings over time. Finally, the resulting eHealth tools should undergo rigorous testing, including pilot trials, to assess their usability, feasibility, and effectiveness in achieving the intended outcomes. This integrated approach provides a holistic strategy for fostering healthier environments in ECEC settings.
Strengths and Limitations
This review is the first to map and summarize the scope of available evidence on eHealth tools designed to assess or improve nutrition and physical activity environments in early learning settings. The findings from this review can guide future research on the use of eHealth technologies to promote healthy practices in childcare, ultimately contributing to improved children’s health behaviors and outcomes. Two librarians with expertise in scoping and systematic reviews assisted in developing and refining the search strategy. The methodology employed facilitated a systematic search of both white and gray literature, ensuring a comprehensive review of available evidence. However, there are some limitations to this scoping review that should be considered. We only considered studies published in English or French, which may have led to the exclusion of relevant research in other languages. Additionally, this scoping review focused solely on full-time day care centers, excluding family-based day care and after-school programs. The primary reason for excluding family-based day cares was the lack of formalized data, and after-school programs were not included as they typically do not cater to children aged 0-5 years. Another limitation encountered during the search for gray literature was the presence of paywalls and restricted access to certain tools, which hindered our ability to fully explore available resources.
Conclusions
This scoping review explored the breadth of evidence on eHealth tools aimed at improving nutrition and physical activity environments in ECEC settings. Future research should conduct a systematic review to assess the effectiveness of these tools and identify the specific elements that contribute to a greater impact and sustained behavior change.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Jayedi A Soltani S Abdolshahi A Shab-Bidar S Healthy and unhealthy dietary patterns and the risk of chronic disease: an umbrella review of meta-analyses of prospective cohort studies Br J Nutr 20201214124111133114410.1017/S 000711452000233032600500 S 000711452000233032600500 · doi ↗ · pubmed ↗
- 2Brawner CA Churilla JR Keteyian SJ Prevalence of physical activity is lower among individuals with chronic disease Med Sci Sports Exerc 2016064861062710.1249/MSS.00000000000008612674111726741117 · doi ↗ · pubmed ↗
- 3Kesäniemi Antero Riddoch CJ Reeder B Blair SNSørensen Thorkild Ia Advancing the future of physical activity guidelines in Canada: an independent expert panel interpretation of the evidence Int J Behav Nutr Phys Act 20100511741 10.1186/1479-5868-7-41204597851479-5868-7-4120459785 PMC 2876061 · doi ↗ · pubmed ↗
- 4Swinburn B A Caterson I Seidell J C James W P T Diet, nutrition and the prevention of excess weight gain and obesity Public Health Nutr 20040271 A 12346 10.1079/phn 20035851497205714972057 · doi ↗ · pubmed ↗
- 5Lee A Cardel M Donahoo WT Feingold KR Anawalt B Blackman MR Social and environmental factors influencing obesity Endotext 2000 South Dartmouth, MAMD Text.com, Inc
- 6Hajat C Stein E The global burden of multiple chronic conditions: a narrative review Prev Med Rep 20181212284293 10.1016/j.pmedr.2018.10.00830406006 S 2211-3355(18)30246-830406006 PMC 6214883 · doi ↗ · pubmed ↗
- 7Hadian M Mozafari MR Mazaheri E Jabbari A Challenges of the health system in preventing non-communicable diseases; systematized review Int J Prev Med 20211271 10.4103/ijpvm.IJPVM_487_2034447513 IJPVM-12-7134447513 PMC 8356955 · doi ↗ · pubmed ↗
- 8Olsen AMøller P Hausner H Early origins of overeating: early habit formation and implications for obesity in later life Curr Obes Rep 20131132215716410.1007/s 13679-012-0046-3 · doi ↗