Physicians' Perspectives on Barriers to Multiple Sclerosis Care in the United Arab Emirates: A Survey Study
Ruqqia Mir, Lev Brylev, Sabah Zahoorudin, Rene A Rivero Jimenez, Rosario Servano, Yandy M Castillo-Aleman, Maysoon M Al Karam, Yendry Ventura-Carmenate, Fatema Al-Kaabi

TL;DR
This study explores challenges in Multiple Sclerosis care in the UAE from neurologists' perspectives, highlighting issues like cost, insurance, and system gaps.
Contribution
The study provides new insights into barriers to MS care in Abu Dhabi, focusing on physician perspectives and gender differences.
Findings
High medication costs and insurance issues are major barriers to MS care.
Private institutions show gaps in monitoring and support practices.
Gender differences in perceived barriers are statistically significant.
Abstract
Introduction: Multiple Sclerosis care in the United Arab Emirates faces several barriers impacting patient outcomes and healthcare delivery. This study aims to identify and analyze these barriers from the perspective of neurologists. Methods: In February 2024, a survey was conducted targeting neurologists involved in Multiple Sclerosis management in Abu Dhabi. The survey included questions on demographics, regularly measured clinical variables, perceived barriers, and contributing factors. A total of 21 neurologists responded, and data were analyzed to identify prevalent issues and correlations. Results: Among the 21 respondents, 15 (71.4%) were male, and 15 (71.4%) were from private institutions. Most neurologists regularly advised on vitamin D level monitoring (16, 76.2%) and psychological support (15, 71.4%). Screening for disease-modifying treatment side effects, Expanded…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
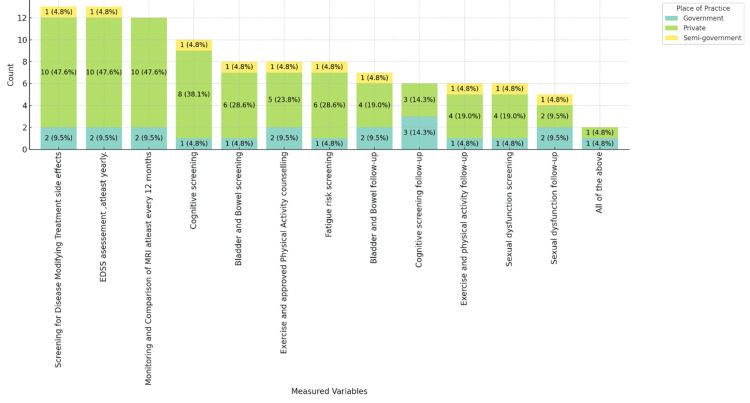 Figure 1
Figure 1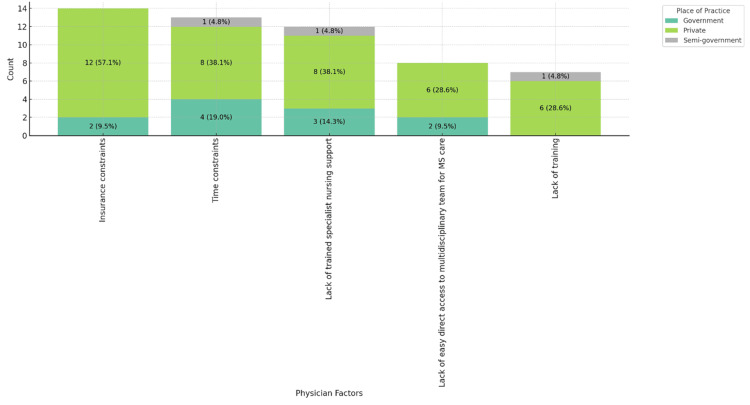 Figure 2
Figure 2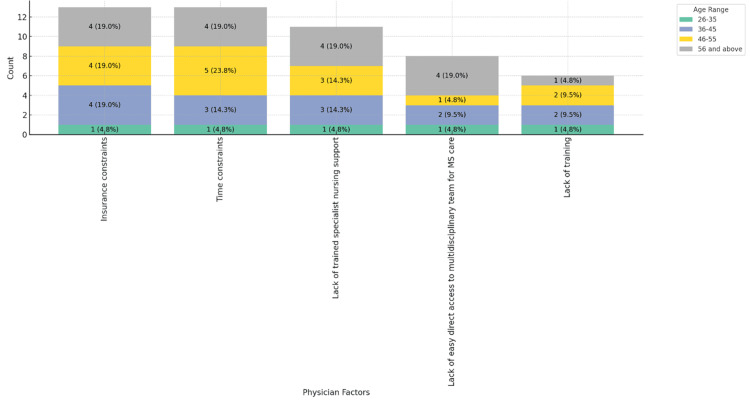 Figure 3
Figure 3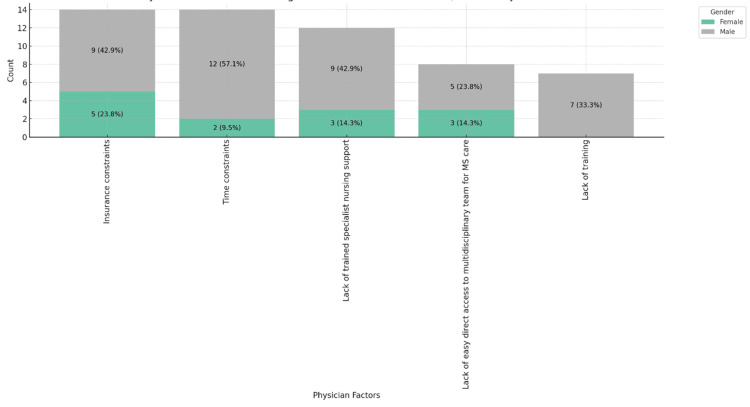 Figure 4
Figure 4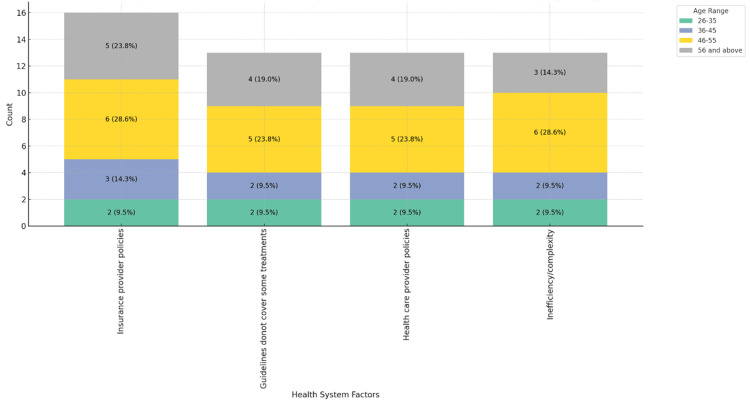 Figure 5
Figure 5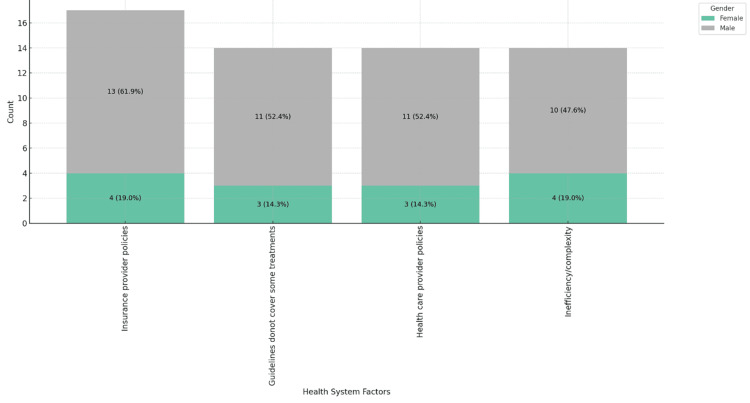 Figure 6
Figure 6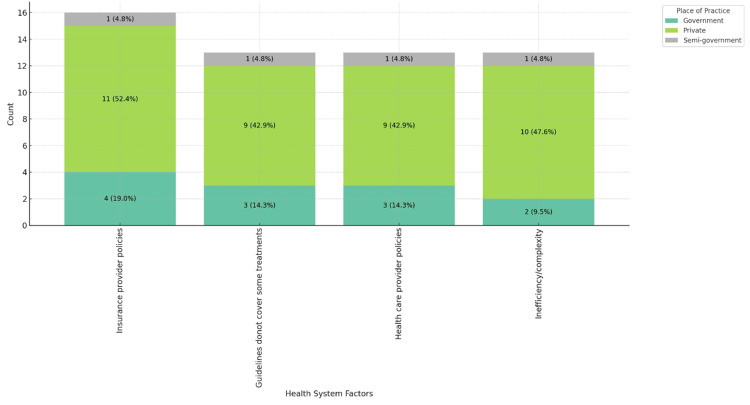 Figure 7
Figure 7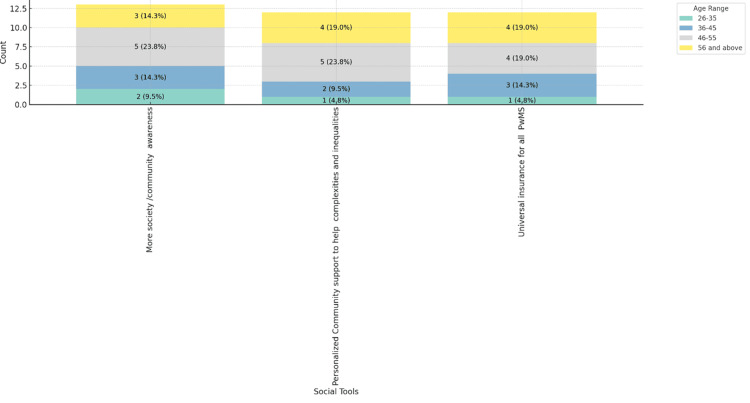 Figure 8
Figure 8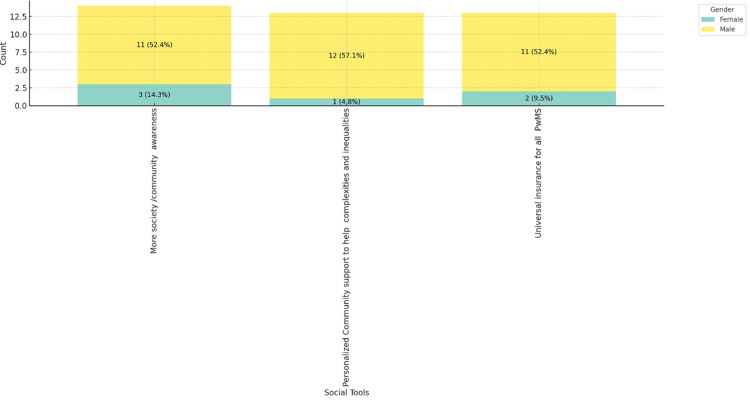 Figure 9
Figure 9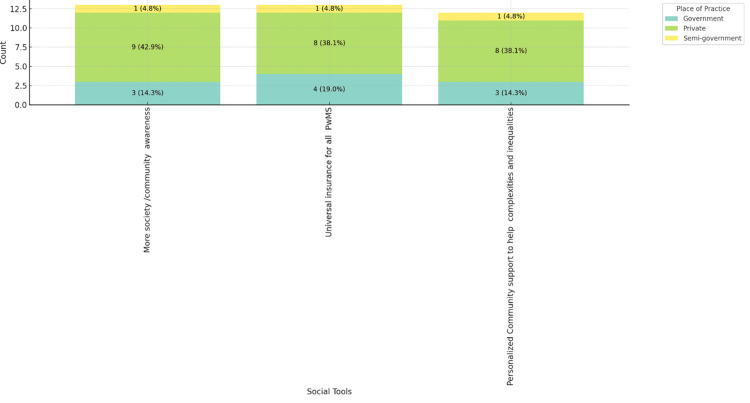 Figure 10
Figure 10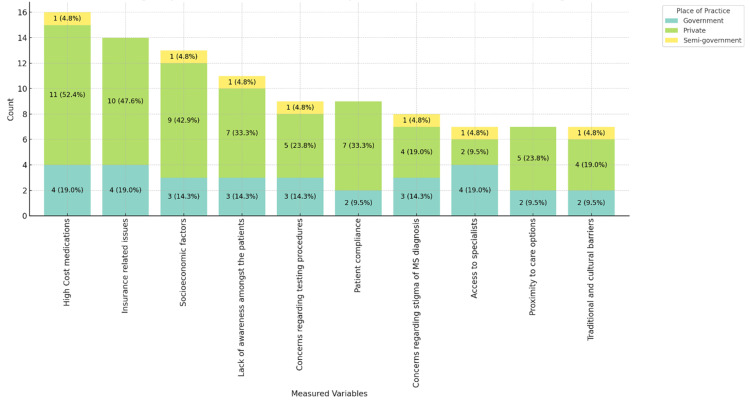 Figure 11
Figure 11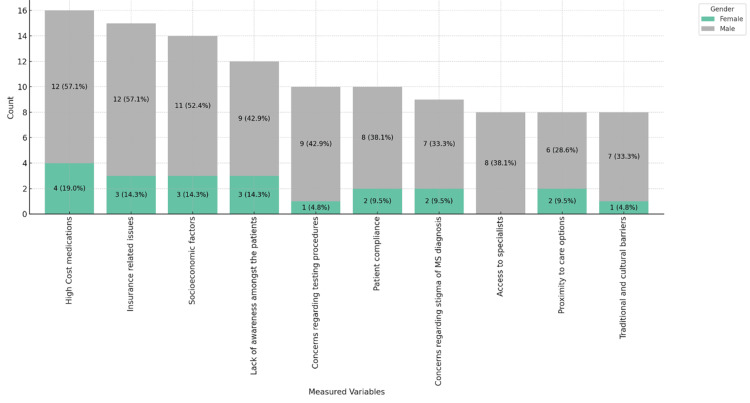 Figure 12
Figure 12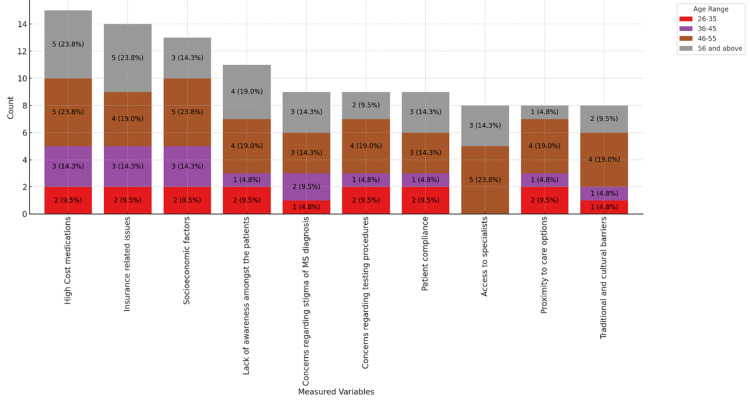 Figure 13
Figure 13| Category | Sub-category (age range) | Count (%) |
| Age | 26-35 | 2 (9.52) |
| 36-45 | 4 (19.05) | |
| 46-55 | 7 (33.33) | |
| 56 and above | 5 (23.81) | |
| Unspecified | 3 (14.29) | |
| Gender | Male | 15 (71.43) |
| Female | 6 (28.57) | |
| Place of practice | Private | 15 (71.43) |
| Semi-government | 1 (4.76) | |
| Government | 4 (19.05) | |
| Unspecified | 1 (4.76) | |
| Knowledge of quality improvement tools | Yes | 18 (85.71) |
| No | 3 (14.29) | |
| Quality measurement tool | American Association of Neurologists | 2 (9.52) |
| MENACTRIMS | 9 (42.86) | |
| NICE guidelines | 2 (9.52) |
| Variable | Count (%) |
| Weight management | 10 (47.62) |
| Blood pressure management | 11 (52.38) |
| Glycemic monitoring | 9 (42.86) |
| Smoking cessation | 14 (66.67) |
| Vitamin D level monitoring | 16 (76.19) |
| Psychological support | 15 (71.43) |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMultiple Sclerosis Research Studies
Introduction
Multiple sclerosis (MS) is a chronic neurological condition that significantly impacts patients' quality of life due to its unpredictable course and progressive nature. Effective management of MS is crucial to alleviate symptoms and improve patient outcomes, adhering to global standards and guidelines [1-3]. In the United Arab Emirates (UAE), the healthcare system has made strides in providing care for MS patients, yet unique regional challenges exist. Recent initiatives aim to enhance MS care, but comprehensive data on current practices and infrastructure remain limited [2,3]. Understanding these practices is essential to identifying areas for improvement.
MS care globally faces numerous challenges, including limited access to specialized treatments and variability in care standards. In the UAE, these issues are compounded by region-specific factors such as healthcare infrastructure and patient demographics [3,4]. Previous studies have highlighted these obstacles, emphasizing the need for targeted interventions. Despite the challenges identified, there is a notable gap in the literature concerning the specific barriers to MS care in the UAE from the perspective of healthcare providers. Current research primarily focuses on patient outcomes and clinical data, leaving a void in understanding physicians' viewpoints [4-7]. Addressing this gap is crucial for comprehensive care improvement.
This study aims to fill the gap by directly surveying physicians involved in MS care to understand the barriers they face. By gathering insights from healthcare providers, the study seeks to identify factors contributing to these barriers and propose solutions to enhance MS care practices. The survey focuses on key topics such as resource availability, treatment accessibility, and administrative support. It aims to provide a detailed understanding of the challenges physicians encounter and how these impact their ability to deliver optimal care to MS patients.
The findings of this study will be valuable for policymakers, healthcare providers, and patients. They will inform future research and healthcare strategies, contributing to the overall improvement of MS care in the UAE and potentially serving as a model for other regions.
Materials and methods
This cross-sectional survey study was conducted in February 2024 to gather insights from neurologists on the barriers to MS care in Abu Dhabi and across the UAE. Participation was voluntary, and electronic informed consent was obtained from all respondents before completing the survey. All data were collected and analyzed anonymously, with no personally identifiable information recorded, ensuring participant confidentiality.
Sample size and participants
A purposive sampling technique was employed. Invitations were sent via email to 120 neurologists practicing in Abu Dhabi and affiliated regions of the UAE. The neurologists were identified through professional networks and local neurology societies. The sample size (n=120) was chosen based on the estimated number of practicing neurologists involved in MS management in the region and practical considerations regarding survey distribution and response rates. Of the 120 invited neurologists, 21 completed and returned the survey, resulting in a response rate of 17.5%.
Inclusion and exclusion criteria
Inclusion criteria were (1) licensed neurologists currently practicing in the UAE; (2) direct involvement in the diagnosis, management, or follow-up of patients with MS; and (3) willingness to provide informed consent and participate in the survey. Exclusion criteria were (1) healthcare professionals not specializing in neurology, (2) neurologists not involved in MS patient care, and (3) those who declined to provide consent or did not complete the survey in full.
Survey instrument and data collection
The questionnaire used in this study was adapted from a previously published instrument examining global barriers to MS care [8]. The original questionnaire was described in detail by Solomon et al. [8] and was modified slightly to reflect regional healthcare structures and resources available in the UAE (Appendix). The adapted survey covered demographics, clinical management practices, perceived barriers, physician-related factors, and healthcare system-related challenges.
A multidisciplinary team of neurologists and quality improvement specialists reviewed and refined the adapted instrument to ensure its relevance and clarity. It comprised multiple sections. The first section focused on demographics and practice characteristics, collecting information such as the respondents’ age range, gender, place of practice (private, government, or semi-government), and knowledge of quality improvement tools. The second section addressed clinical management and monitoring, with questions about variables routinely measured every 6-12 months, including vitamin D levels, screening for disease-modifying treatment side effects, and the use of the Expanded Disability Status Scale (EDSS) or magnetic resonance imaging (MRI) comparisons. Another section explored patient advice, focusing on recommendations provided to MS patients, such as smoking cessation, weight management, psychological support, and monitoring blood pressure and glycemic control.
The survey also investigated perceived barriers and contributing factors, using open-ended and multiple-choice items to identify challenges related to patients, physicians, and the healthcare system. Respondents ranked these barriers and highlighted factors contributing to difficulties in MS care delivery. Additionally, the survey assessed the role of social tools and interventions, aiming to identify community or societal resources that could best improve MS care. The survey was distributed electronically via a secure online platform, with two reminder emails sent at one-week intervals to enhance response rates. Responses were automatically recorded in Microsoft Excel to ensure accuracy and minimize transcription errors.
Statistical analysis
Statistical analysis was performed using Python 3.12.0 with the matplotlib library for data visualization. After data extraction into a CSV format, Python scripts were used to compute frequencies, percentages, and cross-tabulations. Descriptive statistics were generated to summarize participant demographics, practice characteristics, and perceived barriers. Visualizations, including bar charts and stacked plots, were created using matplotlib to illustrate trends, distributions, and comparisons across different physician subgroups, thus enhancing interpretability and facilitating the identification of key patterns in the survey responses.
Results
A total of 120 neurologists were invited to complete the survey, and 21 responded (17.5%). Of these 21 respondents, 15 (71.4%) were male and 6 (28.6%) were female. The age distribution showed that two (9.5%) were aged 26-35, four (19.0%) were 36-45, seven (33.3%) were 46-55, and five (23.8%) were 56 and above, with three (14.3%) unspecified. Regarding the place of practice, 15 (71.4%) were from private institutions, four (19.0%) from government institutions, and one (4.8%) from semi-government institutions, with one (4.8%) unspecified. A majority, 18 (85.7%), were knowledgeable about quality improvement tools, while three (14.3%) were not. The quality measurement tools used included guidelines from the American Association of Neurologists (2, 9.5%), the Middle East North Africa Committee for Treatment and Research in Multiple Sclerosis (MENACTRIMS) (9, 42.9%), and the National Institute for Health and Care Excellence (NICE) (2, 9.5%) (Table 1) [9-11].
The survey included responses to the question: "Do you advise your patients on any of the following regularly?" The results are summarized in Table 2.
The majority of neurologists (16, 76.2%) regularly advise their patients on vitamin D level monitoring, followed closely by psychological support (15, 71.43%) and smoking cessation (14, 66.67%). Blood pressure management (11, 52.38%) and weight management (10, 47.62%) are also common recommendations. While still significant, glycemic monitoring is advised by nine (42.9%) of the respondents. These findings strongly emphasize holistic care approaches that address both physical and psychological aspects of MS management.
The patient's insurance level significantly influences the quality and frequency of checking certain variables, such as vitamin D levels and smoking cessation. Patients with higher insurance coverage are more likely to receive comprehensive monitoring and advice, including regular vitamin D level checks and smoking cessation support. Conversely, those with limited insurance coverage may not have consistent access to these preventive measures, highlighting an inequity in healthcare provision that needs addressing. This disparity underscores the importance of improving insurance policies to ensure equitable healthcare access and quality for all patients.
Figure 1 illustrates the variables regularly measured in MS care, categorized by place of practice (government, private, and semi-government). Screening for disease-modifying treatment side effects, Expanded Disability Status Scale (EDSS) assessment, and magnetic resonance imaging (MRI) comparisons are predominantly carried out by neurologists in private practices, each reported by 10 (47.6%) of respondents from private settings. Cognitive screening (8, 38.1%) and bladder and bowel screening (6, 28.6%) followed and were primarily conducted in private practices. Semi-government practices show minimal engagement across these variables. Other activities, including physical activity counseling, fatigue risk screening, and various follow-ups, show a varied distribution, with private practices leading in most categories. This chart emphasizes the more extensive engagement in private practices, with government and semi-government practices participating to a lesser extent.
Variables regularly measured in MS care, stacked by place of practice.MS: multiple sclerosis.
Figure 2 shows that insurance constraints (12, 57.1%) and time constraints (8, 38.1%) are the primary barriers to MS patient care, as reported predominantly by private practice physicians.
Physician factors contributing to barriers in MS patient care, stacked by place of practice.MS: multiple sclerosis.
Figure 3 indicates that insurance and time constraints uniformly affect MS patient care across all physician age groups, showing no significant age relation (P = 0.147).
Physician factors contributing to barriers in MS patient care, stacked by age range.MS: multiple sclerosis.
Figure 4 reveals gender differences: male physicians report more insurance and time constraints, while female physicians cite insufficient specialist nursing support and access to multidisciplinary teams more often, with a significant gender relation (P = 0.016), suggesting the need for gender-specific strategies.
Physician factors contributing to barriers in MS patient care, stacked by place of gender.MS: multiple sclerosis.
Figures 5-7 highlight the impact of healthcare system factors on MS patient care. Figure 5 shows insurance provider policies as the main barrier across age groups, especially notable in the 46-55 range, 6 (28.6%). Figure 6 reveals a gender disparity, with 13 (61.9%) male physicians citing these policies as a barrier, compared to 4 (19.0%) female physicians. Figure 7 shows that private practice physicians (11, 52.4%) report these issues more frequently than those in government settings (4, 19.0%).
Healthcare system-related factors contributing to barriers in MS patient care, stacked by age range.MS: multiple sclerosis.
Healthcare system-related factors contributing to barriers in MS patient care, stacked by gender.MS: multiple sclerosis.
Healthcare system-related factors contributing to barriers in MS patient care, stacked by place of practice.MS: multiple sclerosis.
Figures 8-10 depict the social tools considered best for improving MS care, categorized by age range, gender, and place of practice. Figure 8 shows that personalized community support and universal insurance for all people with MS are highly valued across all age groups, with more society/community awareness being slightly more favored by respondents aged 46-55, 5 (23.8%). Figure 9 reveals that both male (11, 52.4%) and female (12, 57.1%) respondents prioritize personalized community support and universal insurance equally. Figure 10 indicates that these social tools are consistently favored across different practice settings, with private practice respondents slightly more inclined towards personalized community support (8, 38.1%). These figures highlight the universal recognition of the importance of community support and comprehensive insurance in improving MS care across various demographics and practice environments.
Social tools best for improving MS care in practice, stacked by age range.MS: multiple sclerosis; PwMS: people with multiple sclerosis.
Social tools best for improving MS care in practice, stacked by gender.MS: multiple sclerosis; PwMS: people with multiple sclerosis.
Social tools best for improving MS care in practice, stacked by place of practice.MS: multiple sclerosis; PwMS: people with multiple sclerosis.
Figures 11-13 provide insights into the barriers neurologists believe affect the care of MS patients in their practice, ranked in order of importance. Figure 11 shows that the high cost of medications (11, 52.4%) and insurance-related issues (10, 47.6%) are the most significant barriers, particularly in private practices. Socioeconomic factors (9, 42.9%) and patient compliance (7, 33.3%) are notable barriers. Figure 12 highlights that 12 (57.1%) male physicians report high medication costs and insurance issues as significant barriers, while for female physicians, these barriers are reported at 4 (19.0%) and 3 (14.3%), respectively. Figure 13 categorizes barriers by age range, showing a consistent concern across all age groups, particularly among those aged 46-55 and 56 and above. These figures underscore the multifaceted challenges in MS care, emphasizing financial and systemic barriers as the most critical issues across different demographics and practice settings.
Barriers physicians believe affect the care of MS patients in their practice, stacked by place of practice.MS: multiple sclerosis.
: Barriers physicians believe affect the care of MS patients in their practice, stacked by gender.MS: multiple sclerosis.
Barriers physicians believe affect the care of MS patients in their practice, stacked by age range.MS: multiple sclerosis.
Discussion
The findings from this study highlight significant barriers to MS care in the UAE. The survey revealed that despite perceived high awareness of quality improvement tools, practical barriers persist, impacting the delivery of optimal MS care. This discussion will explore these barriers in detail, contextualize them with existing literature, and provide recommendations for future improvements.
The high awareness and use of quality improvement tools among respondents (18, 85.71%) is promising but may require further training and development of regional quality improvement tools. However, integrating these tools into everyday practice remains challenging. Previous studies have shown that while healthcare providers may be aware of quality improvement strategies, systemic and operational barriers often hinder their effective implementation [12].
MENACTRIMS was included in the quality improvement tool question to understand the neurologists' perspectives on using quality improvement tools in their practice. However, no specific published MENACTRIMS quality improvement tool has been mentioned in the literature. This indicates a potential gap in the availability of standardized quality improvement tools specific to the region, highlighting the need for developing and disseminating such tools tailored to local practice environments.
Regular measurement of clinical variables, such as screening for disease-modifying treatment side effects and MRI comparisons, is critical for effective MS management. Our study found that these practices are widely followed, with no significant variation across different practice settings. This aligns with the global standards for MS care, where regular monitoring is emphasized to manage disease progression [13].
However, it is noteworthy that some doctors do not usually perform the full EDSS assessment, which includes functional scores. This partial assessment may lead to an incomplete understanding of the patient's condition and potentially impact the effectiveness of the management plan. Ensuring that all components of the EDSS assessment are consistently utilized is crucial for a comprehensive evaluation of MS patients and for tailoring treatment plans more accurately.
Patient-related barriers, particularly insurance issues and the cost of medications, were frequently reported. These financial barriers significantly impact patient adherence to treatment plans. Similar findings were reported in other regions, underscoring the universal challenge of healthcare affordability in chronic disease management [14]. The high cost of MS treatments necessitates policy interventions to improve insurance coverage and reduce out-of-pocket expenses for patients.
Clinical practice barriers, such as insurance constraints, costs, and patient compliance issues, were prevalent. These barriers reflect broader systemic problems within the healthcare system. Studies have shown that reducing these barriers requires comprehensive strategies, including policy changes and enhanced patient support systems [15]. Addressing these issues can lead to better health outcomes and more efficient use of healthcare resources.
Physician-related barriers, including time constraints and lack of specialist support, were significant. Gender-related differences were noted, with female physicians reporting different challenges than their male counterparts. This finding suggests the need for tailored interventions that address the specific needs of diverse physician groups to enhance their capacity to provide high-quality MS care [16].
Healthcare system-related barriers, such as insurance provider policies and guideline coverage gaps, were prominent. These systemic issues hinder the delivery of consistent and effective MS care. Policy reforms to standardize insurance coverage and update clinical guidelines to cover all essential treatments are crucial to overcoming these barriers for MS patients [17].
Social tools identified as effective for improving MS care included increased community awareness and personalized support systems. These tools can enhance patient engagement and support and address social and psychological barriers. Implementing these tools requires collaborative efforts between healthcare providers, policymakers, and community organizations [18].
Comparative analysis with similar studies from other regions indicates that many barriers identified in the UAE are consistent with global challenges in MS care. However, some unique regional factors, such as cultural and educational barriers, require tailored strategies. Understanding these unique factors is essential for developing effective, context-specific interventions [19].
This study's limitations include the relatively small sample size and potential biases due to the survey method. These limitations suggest that the findings should be interpreted cautiously and that further research with larger, more diverse samples is needed to validate these results [20].
Based on the findings, several recommendations can be made. Enhancing insurance coverage, reducing treatment costs, and implementing targeted support for physicians are critical. Future research should focus on longitudinal studies to track the impact of these interventions and explore additional strategies to overcome identified barriers [21].
Conclusions
Identifying and addressing the barriers to MS care in the UAE requires a multifaceted approach involving policy changes, systemic improvements, and enhanced support for both patients and healthcare providers. With the progressive improvement in the management of MS care, all stakeholders should be flexible in tackling these challenges to further enhance the quality of MS care and patient outcomes in the region. A task force should be set up to develop standardized quality improvement tools specific to the region and disseminate such tools tailored to local practice environments.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Multiple sclerosis Lancet Compston A & Coles A 1502151737220081897097710.1016/S 0140-6736(08)61620-7 · doi ↗ · pubmed ↗
- 2Prevalence, demographics and clinical characteristics of multiple sclerosis in Qatar Mult Scler Deleu D Mir D Al Tabouki A 8168191920132296854510.1177/1352458512459291 · doi ↗ · pubmed ↗
- 3The challenge of multiple sclerosis: how do we cure a chronic heterogeneous disease?Ann Neurol Weiner HL 2392486520091933406910.1002/ana.21640 · doi ↗ · pubmed ↗
- 4Multiple sclerosis Lancet Thompson AJ Baranzini SE Geurts J 1622163639120182957650410.1016/S 0140-6736(18)30481-1 · doi ↗ · pubmed ↗
- 5Sick leave and occupational burnout among nurses caring for patients with multiple sclerosis Mult Scler Relat Disord Saposnik G Bueno-Gil G SempereÁP 1039166320223566156610.1016/j.msard.2022.103916 · doi ↗ · pubmed ↗
- 6Quantifying the relationship between increased disability and health care resource utilization, quality of life, work productivity, health care costs in patients with multiple sclerosis in the USBMC Health Serv Res Jones E Pike J Marshall T Ye X 2941620162744327810.1186/s 12913-016-1532-1PMC 4957342 · doi ↗ · pubmed ↗
- 7Multiple sclerosis: clinical aspects Curr Opin Neurol Oh J Vidal-Jordana A Montalban X 7527593120183030023910.1097/WCO.0000000000000622 · doi ↗ · pubmed ↗
- 8Global barriers to the diagnosis of multiple sclerosis: data from the Multiple Sclerosis International Federation Atlas of MS, third edition Neurology Solomon AJ Marrie RA Viswanathan S 035101202310.1212/WNL.0000000000207481 PMC 1042483237321866 · doi ↗ · pubmed ↗