Carbapenem Usage in the Initial Antibiotic Therapy of Sepsis in Japanese Intensive Care Units
Eri Kobayashi, Atsushi Shiraishi, Toshiyuki Karumai, Yoshiro Hayashi, Toshikazu Abe, Hiroshi Ogura, Kushimoto Shigeki, Satoshi Gando, Kohji Okamoto, Yutaka Umemura, Junichi Sasaki, Yasukazu Shiino, Toshihiko Mayumi

TL;DR
This study found that over half of sepsis patients in Japanese ICUs received carbapenems as initial treatment, but no link was found between carbapenem use and in-hospital mortality.
Contribution
The study provides new insights into carbapenem usage patterns and their clinical outcomes in sepsis treatment within Japanese ICUs.
Findings
55% of sepsis patients in Japanese ICUs received carbapenems as initial antibiotic therapy.
In-hospital mortality was not significantly associated with carbapenem use after adjusting for patient and hospital factors.
Carbapenem use varied widely across ICUs, with a median utilization rate of 55.2%.
Abstract
Background Achieving a balance between the utilization and limitation of carbapenems for initial sepsis therapy is imperative, yet documentation on the use of carbapenems in sepsis treatment is limited. This study aimed to ascertain the prevalence of carbapenem use in Japanese intensive care units (ICUs) and evaluate the association between its use in the initial antibiotic therapy for sepsis and patient prognosis. Methods This study is a post hoc descriptive analysis of the Focused Outcome Research on Emergency Care for Acute Respiratory Distress Syndrome, Sepsis, and Trauma (FORECAST), a multicenter, prospective cohort study conducted in 59 ICUs in Japan from January 2016 to March 2017. This study described the rate of carbapenem use overall and in each ICU and assessed the association between carbapenem use and in-hospital mortality by generalized linear mixed effect model…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
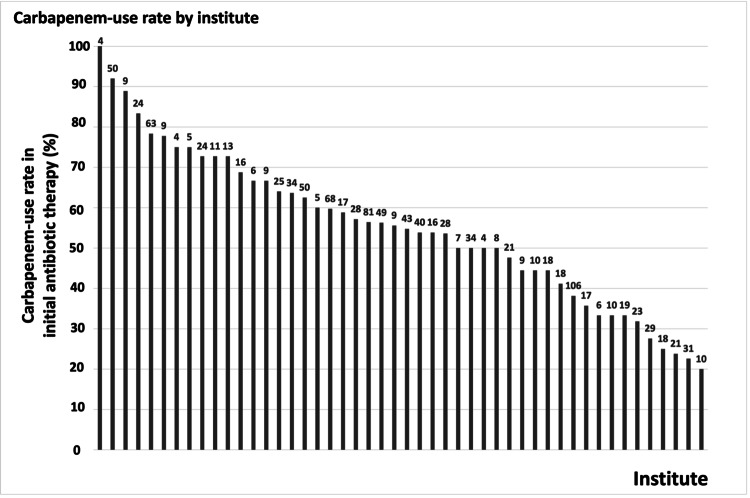 Figure 1
Figure 1| Baseline characteristics | Overall, n=1140 | Carbapenem group, n=627 (55.0%) | Non-carbapenem group, n=513 (45.0%) |
| Age | 73 (63,81) | 72 (64,81) | 73 (63,81) |
| Sex (male) | 696 (61.1%) | 380 (60.6%) | 316 (61.6%) |
| Charlson Index | 1 (0,2) | 1 (0,2) | 1 (0,2) |
| Infection site | |||
| Abdominal | 297 (26.1%) | 182 (29.0%) | 115 (22.4%) |
| Respiratory | 353 (31.0%) | 159 (25.4%) | 194 (37.8%) |
| Urinary tract | 213 (18.7%) | 127 (20.3%) | 86 (16.8%) |
| Skin/soft tissue | 112 (9.8%) | 75 (12.0%) | 37 (7.2%) |
| Catheter | 22 (1.9%) | 11 (1.8%) | 11 (2.1%) |
| Central nervous system | 22 (1.9%) | 10 (1.6%) | 12 (2.3%) |
| Osteoarticular | 21 (1.8%) | 8 (1.3%) | 13 (2.5%) |
| Endocardium | 16 (1.4%) | 8 (1.3%) | 8 (1.6%) |
| Implant device | 8 (0.7%) | 3 (1.0%) | 5 (0.1%) |
| Wound | 12 (1.1%) | 4 (0.6%) | 8 (1.6%) |
| Other | 64 (5.6%) | 40 (6.4%) | 24 (4.7%) |
| SOFA | 9 (6,11) | 9 (7,12) | 8 (5,11) |
| APACHE II | 22 (17,29) | 23 (17,30) | 22 (16,29) |
| Septic shock | 717 (62.9%) | 456 (72.7%) | 261 (50.9%) |
| Time to antibiotics use (min) | 101 (55,191) | 99 (51,190) | 107 (59,191) |
| De-escalation | 644 (56.5%) | 410(65.4%) | 234(45.6%) |
| Facilities form | |||
| University hospital | 690 (60.5%) | 376 (60.0%) | 314 (61.2%) |
| Teaching hospital | 432 (37.9%) | 246 (39.2%) | 186 (36.3%) |
| Other | 18 (1.6%) | 5 (0.8%) | 13 (2.5%) |
| Number of hospital beds | |||
| ≤500 | 177 (15.5%) | 99 (15.8%) | 78 (15.2%) |
| 501-1000 | 723 (63.4%) | 385 (61.4%) | 338 (65.9%) |
| ≥1001 | 240 (21.1%) | 143 (22.8%) | 97 (18.9%) |
| Number of ICU beds per year | |||
| ≤10 | 355 (31.1%) | 183 (29.2%) | 172 (33.5%) |
| 11-20 | 558 (48.9%) | 313 (49.9%) | 245 (47.8%) |
| ≥21 | 221 (19.4%) | 128 (20.4%) | 93 (18.1%) |
| Annual ICU admissions (data of 2013) | |||
| none | 5 (0.4%) | 3 (0.5%) | 2 (0.4%) |
| ≤500 | 210 (18.4%) | 100 (15.9%) | 110 (21.4%) |
| 501-1000 | 610 (53.5%) | 351 (56.0%) | 259 (44.6%) |
| ≥1001 | 309 (27.1%) | 170 (27.1%) | 139 (27.1%) |
| Tertiary emergency facility | 981 (86.1%) | 538 (85.8%) | 443 (86.4%) |
| Department of infectious diseases | 490 (43.0%) | 282 (45.0%) | 208 (40.5%) |
| Antibiotics | Carbapenem group, n=627 (55.0%) | Non-carbapenem group, n=513 (45.0%) |
| Penicillin | 31 (4.9%) | 315 (61.4%) |
| Cephalosporin | 15 (2.4%) | 148 (28.9%) |
| Monobactam | 0 (0%) | 0 (0%) |
| Aminoglycoside | 3 (0.5%) | 5 (1.0%) |
| Quinolone | 12 (1.9%) | 7 (1.4%) |
| Macrolide | 0 (0%) | 0 (0%) |
| Tetracycline | 2 (0.3%) | 5 (1.0%) |
| Anti-MRSA drug | 189 (30.1%) | 81 (15.8%) |
| Antifungal drug | 34 (5.4%) | 17 (3.3%) |
| Antiviral drug | 0 (0%) | 3 (0.6%) |
| Other | 40 (6.4%) | 20 (3.9%) |
| Other treatment | Carbapenem group, n=627 (55.0%) | Non-carbapenem group, n=513 (45.0%) |
| Norepinephrine | 473 (75.4%) | 258 (50.3%) |
| IRRT | 22 (3.5%) | 13 (2.5%) |
| CRRT | 199 (31.7%) | 95 (18.5%) |
| PMX | 76 (12.1%) | 21 (4.1%) |
| Protease inhibitor | 54 (8.6%) | 28 (5.5%) |
| Sivelestat | 21 (3.3%) | 17 (3.3%) |
| IVIg | 165 (26.3%) | 50 (9.7%) |
| Corticosteroid | 223 (35.6%) | 110 (21.4%) |
| AT | 149 (23.8%) | 73 (14.2%) |
| rhTM | 168 (26.8%) | 67 (13.1%) |
| Variables | Carbapenem group, n=627 (55.0%) | Non-carbapenem group, n=513 (45.0%) | Unadjusted difference (95%CI) | Adjusted difference (95%CI) |
| In-hospital mortality, n (%) | 158/616 (25.6%) | 101/493 (20.5%) | 5.2 (0.2,10.2) | 1.2 (-4.3,6.6) |
| 28-day mortality, n (%) | 127/612 (20.8%) | 79/487 (16.2%) | 4.5 (-0.1,9.2) | 1.0 (-4.0,5.9) |
| Length of hospital stay, days | 38 (42) | 33 (35) | 6 (1,10) | 4 (-1,10) |
| 28-day ventilator-free days | 15 (11) | 18 (12) | -2 (-3,-1) | -1 (-3,0) |
| 28-day ICU-free days | 15 (9) | 18 (9) | -2 (-3,-1) | -1 (-2,0) |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsSepsis Diagnosis and Treatment · Nosocomial Infections in ICU · Antibiotics Pharmacokinetics and Efficacy
Introduction
Carbapenems have been widely used to treat bacterial infections in recent years. Studies from Latin American countries (2008 to 2009), Poland (2014 to 2015), and Japan (2011) indicate that the usage rate of carbapenems was approximately 20% [1-3]. A study from the United States indicated that carbapenems were prescribed 11.2% between 2004-2014 [4]. Furthermore, this usage trend has consistently grown over time. Longitudinal data shows an increase in Europe from 76 defined daily doses (DDD) in 2001 to 216 DDD in 2011. Similarly, in Germany, there was a rise from 76 DDD in 2001 to 250 DDD in 2015, while intensive care units (ICU) in Switzerland recorded an uptick from 114 DDD in 2009 to 156 DDD in 2018 [5-7].
However, carbapenems are typically considered last-resort antibiotics. The escalating use of these drugs has raised concerns about the rise in carbapenem-resistant bacteria [8-10]. Consequently, antimicrobial stewardship, which includes a carbapenem-sparing strategy, has been emphasized as crucial in combating antimicrobial resistance and reducing healthcare costs [11-13]. Further, implementing a carbapenem-sparing strategy in sepsis therapy could reduce costs without negatively impacting patient outcomes [14,15].
Finding a balance between the utilization and restriction of carbapenems in initial sepsis therapy is crucial. However, there is limited documentation on carbapenem use in the initial antibiotic treatment for sepsis. This study aimed to illustrate the prevalence of carbapenem use in the initial antibiotic treatment of septic patients, the prognosis of those who received carbapenems, and the variation in carbapenem use across various institutions in Japanese ICUs.
Materials and methods
Design and data source
This study was a post hoc descriptive analysis of the sepsis sub-study from the Focused Outcome Research on Emergency Care for Acute Respiratory Distress Syndrome, Sepsis, and Trauma (FORECAST) study. FORECAST was a multi-center, prospectively collected cohort study conducted in 59 ICUs across Japan from January 2016 to March 2017 [16]. The FORECAST sepsis study included adult patients (age ≥16 years) with severe sepsis or septic shock, as defined by the sepsis-2 criteria, who were admitted to the ICUs of the participating hospitals [17]. Patients with limitations on sustained life care or those in a post-cardiopulmonary arrest resuscitation status at sepsis diagnosis were excluded. These details are described in a previous article (UMIN-CTR ID: UMIN000019742) [16]. According to the sepsis-2 criteria proposed in 2001, sepsis was defined in the FORECAST study as the probable or documented presence of infection along with the systemic response to that infection [17]. Additionally, severe sepsis was defined as sepsis accompanied by sepsis-induced organ dysfunction or tissue hypoperfusion. Septic shock was characterized as sepsis-induced hypotension persisting despite adequate fluid resuscitation [17,18].
Participants
Patients were selected from the FORECAST study if they had available data on the use of initial antibiotic therapy for sepsis. No exclusion criteria were applied.
Variables
The baseline characteristics of the study population included demographics, site of infection, and laboratory tests at the time of sepsis diagnosis in the emergency department or intensive care unit. The study's exposure variable was whether or not a carbapenem was used as the initial antibiotic treatment. Intermediate variables encompassed dialysis, polymyxin B hemoperfusion, sivelestat sodium hydrate, intravenous immunoglobulin, antithrombin, and recombinant human soluble thrombomodulin. We also evaluated characteristics of the study hospitals, such as the type and volume of the hospital and the presence or absence of an infectious disease department. The proportion of carbapenem use in each ICU was documented for study hospitals that enrolled more than three patients in the FORECAST registry. Outcome variables for the study were in-hospital mortality, 28-day mortality, 28-day length of hospital stay, 28-day ventilator-free days, and 28-day ICU-free days.
Statistical analysis
Descriptive statistics comprised percentages for categorical variables and medians with interquartile ranges (IQR) for continuous variables, as not all variables followed normal distributions. The association between the initial use of carbapenems and in-hospital mortality was considered to vary across both the site of infection and the hospitals. The association was assessed using a generalized linear mixed-effects model, with adjustments for age and Sepsis-related Organ Failure Assessment (SOFA) score at presentation as fixed-effect confounders and the site of infection and the identification number of the treating hospital as random-effect confounders. The treatment effect was estimated as absolute risk differences with 95% confidence intervals. Statistical analyses were conducted using R 4.4.2 (R Foundation for Statistical Computing, Vienna, Austria), a language and environment for statistical computing.
Results
Of the 1184 patients registered in the FORECAST sepsis study, 1140 were included, and 44 patients were excluded due to missing antibiotic use data. Of the included patients, 627 (55.0%) initially received carbapenem treatment.
The age, sex, Acute Physiology and Chronic Health Evaluation II (APACHE II), and SOFA scores were comparable between groups (Table 1). Patients who received carbapenems had a higher incidence of septic shock than those who didn't. The most common sites of infection were the abdomen for the carbapenem group and the respiratory system for the non-carbapenem group. The carbapenem group showed a higher prevalence of anti-methicillin-resistant Staphylococcus aureus antibiotic usage, whereas the non-carbapenem group was more frequently treated with penicillin and cephalosporin antibiotics (Table 2). Moreover, carbapenem recipients exhibited higher rates of vasopressor agent use and dialysis (Table 3).
Out of the 59 participating ICUs, 48 enrolled more than three patients in the FORECAST registry. Among these ICUs, the prevalence of initial carbapenem use varied widely, showing a median of 55.2% (IQR: 43.6%-67.2%), ranging from 20.0% to 100.0% (Figure 1).
The proportion of carbapenem-use in each ICUsThe numbers above each bar represent the number of registered cases. The study hospitals enrolled more than three patients in the FORECAST registry.ICU - intensive care unit; FORECAST - Focused Outcome Research on Emergency Care for Acute Respiratory Distress Syndrome, Sepsis, and Trauma
In-hospital mortality was noted in 158 (25.6%) of the patients who received carbapenems, compared to 101 (20.5%) of those who did not (Table 4). In the unadjusted model, initial carbapenem use was significantly associated with increased in-hospital mortality (difference of 5.2%; 95% CI: 0.2%-10.2%, p=0.04). However, this association was insignificant in the adjusted model (difference of 1.2%; 95% CI: -4.3%-6.6%, p=0.66). Initial carbapenem use wasn't significantly linked to 28-day mortality in either model. Yet, it correlated with longer 28-day hospital stays, fewer 28-day ventilator-free days, and 28-day ICU-free days in the unadjusted model but not in the adjusted model.
Discussion
Our study revealed that over half of the patients with severe sepsis or septic shock in Japanese ICUs received carbapenems as their initial antibiotic therapy. Notably, there was considerable variation in this practice across institutions. After accounting for known confounding factors and clusters, carbapenem use did not correlate with improved in-hospital mortality rates.
In our examination of carbapenem usage among patients with severe sepsis or septic shock in Japanese ICUs, we found that 55% of patients were initially prescribed carbapenems. Previous guidelines, such as the 2016 Surviving Sepsis Campaign guidelines (SSCG) and the 2013 Japanese guidelines for managing sepsis, recommended the prompt initiation of empiric broad-spectrum therapy within one hour of diagnosis [19,20]. This recommendation might have contributed to the high rate of initial carbapenem use. Factors like limited awareness of antimicrobial resistance and inadequate promotion of antimicrobial stewardship practices in Japan may have influenced the preference for carbapenems in initial sepsis treatment [21-23].
Furthermore, the results of our investigation revealed no statistically significant disparity in mortality rates between the administration of carbapenem and alternative antibiotics. This aligns with the findings of other studies, which did not show significant differences in clinical efficacy, safety outcomes, and mortality rates when comparing carbapenems with alternative antibiotics [15,24,25]. Thus, evidence supporting carbapenems' superiority in clinical outcomes in sepsis treatment is scant. Interestingly, our study underscores the inter-institutional disparity in using carbapenems as an initial therapy. While the reasons for such differences remain unclear, prior studies have suggested that antibiotic use patterns can vary based on geographical location, country, and healthcare setting [26-28]. A multicenter survey conducted in North America indicated that several factors, such as facility size, number of ICU beds, use of non-carbapenem beta-lactams, and specific stewardship strategies, might influence the rate of carbapenem use [29]. In a survey of antibiotic prescribing practices in Japan, university hospitals and open ICUs exhibited significantly higher carbapenem use [3]. The elevated rate of carbapenem prescriptions in certain institutions might be influenced by factors like awareness of antimicrobial resistance, monitoring of antibiograms and antibacterial stewardship. However, these were not evaluated in our study.
Our study has several limitations. The dataset did not specify the types of carbapenems administered. There was no evaluation of causative bacteria susceptibility or the prevalence of antimicrobial-resistant strains, limiting the assessment of antibiotic appropriateness. The study also did not analyze the dosage and duration of antimicrobial use, carbapenem administration technique, and length of stay in the hospital and ICU at the time of antibiotic therapy. Being retrospective, it did not evaluate causal relationships, and patient characteristics were not examined in detail. Follow-ups post-hospital discharge were not conducted. Although there is wide variability in carbapenem usage among institutions, there was no evaluation of antimicrobial stewardship programs or level of care. Moreover, the selection of facilities from the FORECAST study may limit the generalizability of our findings to the broader Japanese population. As a single-nation study, the external validity of our results for other countries is constrained.
Conclusions
In Japanese ICUs, carbapenems were used as the initial antibiotic treatment for over half of the sepsis patients. However, the frequency of this practice varied across institutions. The use of carbapenems was not associated with improved in-hospital mortality rates after adjusting for known confounding factors.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Surveillance of antibiotic prescribing in intensive care units in Poland Can J Infect Dis Med Microbiol Trejnowska E Deptuła A Tarczyńska-Słomian M 5670238201820183022883310.1155/2018/5670238 PMC 6136475 · doi ↗ · pubmed ↗
- 2Antibiotic prescription in intensive care units in Latin America Rev Argent Microbiol Curcio DJ 203211432011 https://pubmed.ncbi.nlm.nih.gov/22430995/2243099510.1590/S 0325-75412011000300007 · doi ↗ · pubmed ↗
- 3A nationwide survey of intravenous antimicrobial use in intensive care units in Japan Int J Antimicrob Agents Ohnuma T Hayashi Y Yamashita K Marquess J Lefor AK Sanui M 6366415120182940873710.1016/j.ijantimicag.2018.01.022 · doi ↗ · pubmed ↗
- 4β-lactams and β-lactamase inhibitors: an overview Cold Spring Harb Perspect Med Bush K Bradford PA 06201610.1101/cshperspect.a 025247 PMC 496816427329032 · doi ↗ · pubmed ↗
- 5Surveillance of antibiotic use and resistance in intensive care units (SARI). A 15-year cohort study Dtsch Arztebl Int Remschmidt C Schneider S Meyer E Schroeren-Boersch B Gastmeier P Schwab F 85886511420172927134510.3238/arztebl.2017.0858 PMC 5763000 · doi ↗ · pubmed ↗
- 6Antibiotic consumption and resistance: data from Europe and Germany Int J Med Microbiol Meyer E Gastmeier P Deja M Schwab F 38839530320132372739610.1016/j.ijmm.2013.04.004 · doi ↗ · pubmed ↗
- 7Antimicrobial resistance and antibiotic consumption in intensive care units, Switzerland, 2009 to 2018 Euro Surveill Barnsteiner S Baty F Albrich WC 11126202110.2807/1560-7917.ES.2021.26.46.2001537 PMC 860340534794535 · doi ↗ · pubmed ↗
- 8Correlation between antimicrobial consumption and antimicrobial resistance of Pseudomonas aeruginosa in a hospital setting: a 10-year study J Clin Pharm Ther Mladenovic-Antic S Kocic B Velickovic-Radovanovic R Dinic M Petrovic J Randjelovic G Mitic R 5325374120162751180810.1111/jcpt.12432 · doi ↗ · pubmed ↗