Giant inguinal hernia with mal-rotation in a resource-limited area: Case report
Abdirahman Burale, Mahir Yusuf Kahir, Musse Ahmed, Ahmednour Sh Abdirahman Elmi, Abdirahman Ibrahim Said, Hassan Sh. Abdirahman Elmi

TL;DR
A rare giant inguinal hernia case in a resource-limited area was successfully treated with a tailored surgical approach.
Contribution
Highlights the need for standardized protocols for managing giant inguinal hernias in low-resource settings.
Findings
Giant inguinal hernias are rare and pose significant surgical challenges in low- and middle-income countries.
A tailored surgical strategy, including Ladd's procedure and appendectomy, led to a successful outcome in this case.
Anatomical anomalies like malrotation complicate management and require individualized approaches.
Abstract
Giant inguinoscrotal hernias (GIH), defined as hernias extending below the inner thigh midpoint in a standing position, are rare and often seen in resource-limited settings due to delayed medical care. These hernias pose surgical challenges, particularly in low- and middle-income countries (LMICs), where standardized management protocols are lacking, and risks such as cardiorespiratory compromise are significant. A 55-year-old male presented with a large, irreducible right inguinoscrotal hernia of 1.5 years duration. Elective surgery involved sac separation and laparotomy, revealing herniation of bowel segments, including the terminal ileum and sigmoid colon, with concurrent intestinal malrotation. Ladd's procedure, appendectomy, and hernia repair were performed without complications. Postoperative recovery was uneventful, with the patient remaining asymptomatic during follow-up. GIH…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
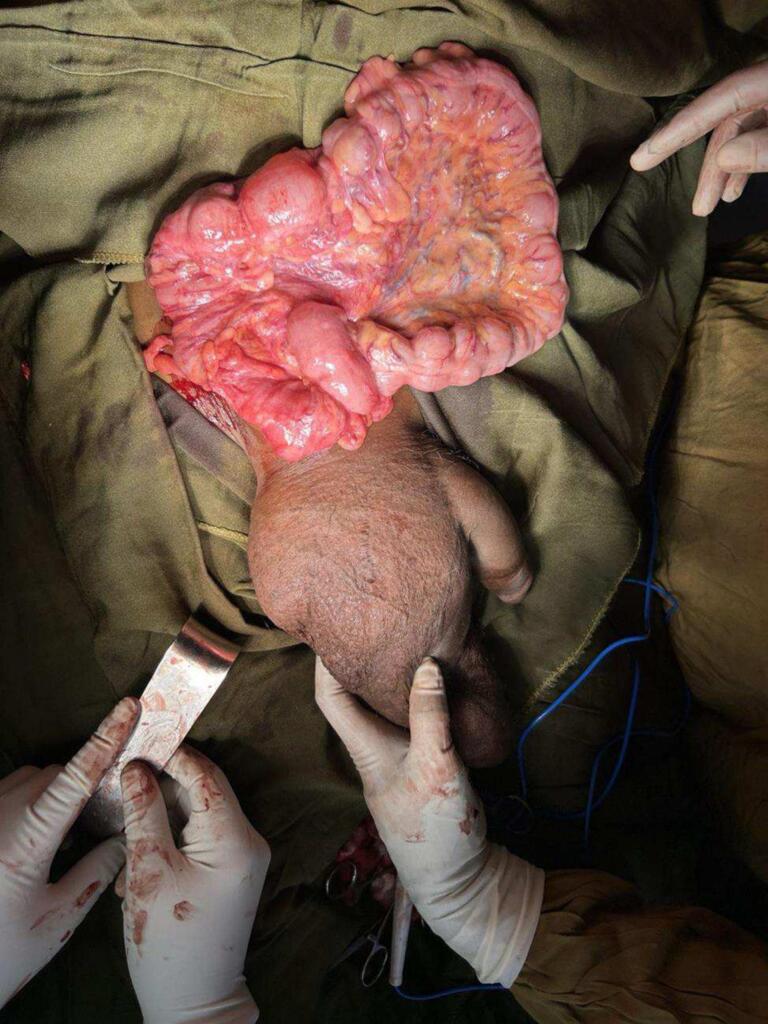 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHernia repair and management · Intestinal and Peritoneal Adhesions · Congenital Diaphragmatic Hernia Studies
Introduction
1
Giant inguinoscrotal hernias are defined as hernias extending below the midpoint of the inner thigh in the standing position [1]. These hernias, though rare, often result from prolonged neglect or fear of surgical intervention and are more prevalent in rural populations and resource-limited regions, particularly in Sub-Saharan Africa [2]. In these low-resource settings, patients may avoid seeking medical care due to limited access, financial constraints, or lack of awareness, leading to the progression of hernias to this advanced stage.
These massive hernias present significant surgical challenges. One primary concern during the surgical repair is the potential for cardiorespiratory compromise, which can result from the sudden increase in intra-abdominal pressure following the replacement of herniated viscera into the abdominal cavity [3]. This issue underscores the need for careful preoperative assessment and planning in cases of giant hernias, especially in low- and middle-income countries (LMICs).
Unlike high-income countries (HICs), which are less likely to encounter such extensive hernias, LMICs face unique challenges in addressing these conditions. Given the frequency and complexity of these cases, preparedness for managing giant inguinoscrotal hernias is essential in LMICs [4]. Furthermore, there is currently no established standard treatment protocol for managing giant inguinoscrotal hernias, adding to the complexity and variability in their management across different settings [5]. This case report highlights the challenges of managing a giant inguinal hernia with malrotation in a resource-limited setting.
Case presentation
2
A 55-year-old male patient who underwent hernia repair surgery for an indirect inguinal hernia 2 years back currently presented with a vast scrotal mass of 1 and a half years duration associated with intermittent lower abdominal pain. On examination, there was a surgical scar over the right inguinal region and significant irreducible, non-tender right inguinoscrotal swelling reaching up to the mid-point of the inner thigh. This work has been reported in line with the SCARE criteria [6].
The patient was scheduled for elective surgery under spinal anesthesia. An oblique inguinal incision was made, and subsequently, the sac was separated from the cord and opened; reduction of content from the scrotum was challenging, and terminal ilium, appendix, cecum, ascending colon, transverse colon, descending colon, and proximal part sigmoid colon was found to be herniated into the scrotum with no evidence of ischemia. By this time, laparotomy was done for adequate evaluation of the mal-rotation and proper replacement of the bowel. It was found that the ascending colon and descending colon did not have a retroperitoneal attachment. The third and fourth part of the duodenum descended vertically on the right side in the absence of ligament of Treitz. Ladd's procedure was done with appendectomy. The wound was closed primarily without undue tension; the patient had a smooth postoperative course and discharged on the 5th post-op day. Up on fellow up on his 14th post-op, he had no complaint, and the wound was healing.
See Fig. 1: - for how intra-operative reduction of content from the scrotum through an oblique right inguinal incision (terminal ileum, cecum, ascending colon, transverse colon, descending colon, and proximal sigmoid colon) but i\still some distal sigmoid colon is inside the scrotum as shown on the image, thought the scrotum is partially decompressed it reaches up to mid-thigh.Fig. 1- shows intra-operative reduction of content from the scrotum through an oblique right inguinal incision (terminal ileum, cecum, ascending colon, transverse colon, descending colon, and proximal sigmoid colon) but i\still some distal sigmoid colon is inside the scrotum as shown on the image, thought the scrotum is partially decompressed it reaches up to mid-thigh.Fig. 1
Discussion
3
Giant inguinoscrotal hernias (GIH) are classified into three types based on their extent, influencing management approaches. Type I hernias, which extend to the suprapatellar margin, generally require only hernioplasty with intra-abdominal and intrathoracic pressure monitoring without additional interventions to prevent abdominal compartment syndrome (ACS). Types II and III, characterized by loss of domain, may necessitate further measures to prevent ACS, such as resection of hernia contents and techniques to increase abdominal volume, including Preoperative Progressive Pneumoperitoneum (PPP), Botulinum toxin A injection and component separation. Studies report successful outcomes with these approaches, even in complex bilateral cases, highlighting the need for tailored management strategies based on hernia classification [7].
The development of giant inguinal hernias, despite advancements in medical procedures and the availability of effective treatments, remains a significant issue. Several factors contribute to this phenomenon. For instance, a case report from Kashmir, India, describes a 62-year-old male whose hernia developed primarily due to a lack of awareness regarding the surgical procedure. When the patient was informed about the possibility of local anesthesia, he had accepted the procedure. This highlights the critical role of patient education and awareness in the timely management of such conditions [8].
In another case from Nepal, a 65-year-old male presented with progressive swelling and multiple non-discharging ulcers over the scrotal skin. The patient delayed seeking medical attention due to financial constraints and a lack of confidence in the surgical system [4]. These factors, particularly financial limitations, play a significant role in the neglect of such conditions. A study investigating the reasons for delays in treatment found that financial barriers and neglect of the condition were the primary causes. Additionally, the patients often sought medical care only when their condition interfered with daily activities, such as the inability to engage in sexual intercourse, which led to psychological distress [9].
Giant inguinoscrotal hernias (GIH) pose significant challenges for patients and surgeons, particularly in resource-limited settings. These massive hernias can severely impact mobility, leading to difficulties in walking, sitting, or even lying down. Patients may also experience scrotal skin ulceration, urinary retention due to pressure on the penis, and potentially life-threatening tissue expansion of vascular pedicles [1] [10]. Our patient's case highlights the challenges of managing a GIH in a resource-limited setting, as he initially declined surgery due to the perceived complexity and potential complications.
Various surgical techniques have been described for GIH repair, with approaches focusing on either increasing abdominal capacity or reducing hernia contents. Preoperative progressive pneumoperitoneum therapy, involving inflating the abdominal cavity with air to create space for hernia contents, has shown promise in some cases but can lead to discomfort, shoulder pain, and potential complications [11] [12]. Another approach involves debulking the hernia contents by resecting bowel segments, which carries the risk of anastomotic insufficiency and prosthetic infection [13] [14]. The best surgical strategy must be tailored to the individual patient, their health, and available resources. A combined approach involving a transabdominal midline incision, omental resection, and mesh placement in a preperitoneal position successfully reduced the hernia without requiring bowel resection.
Minimally invasive surgery for giant inguinoscrotal hernias is challenging due to their size and potential for “loss of domain,” often requiring open approaches like the one described by Staubitz et al. Their case highlights the need for open surgery to address complex issues that may include component separation, tailored mesh placement, and orchiectomy after a failed laparoscopic attempt. While future possibilities may lie in improving abdominal space or robot-assisted techniques, open surgery, and combined open approaches, remains a necessary option, allowing for the best results as seen in the successful repair by the authors of the case study [15].
The presence of malrotation in our patient is unusual, as this congenital anomaly is typically diagnosed in infancy [16] [17]. This case highlights the importance of considering potential anatomical variations, even in adult patients with GIH. Complications of GIH repair are common and can include respiratory compromise, wound dehiscence, hematocele/seroma formation, and recurrent hernias. These complications can be more challenging to manage in resource-limited settings [18,19]. Careful postoperative follow-up is essential to monitor for complications and ensure long-term success. In our patient's case, the successful repair with the chosen surgical approach and meticulous postoperative care led to a favorable outcome. This case report can contribute to a better understanding of GIH management in resource-limited settings, promoting further research and encouraging the development of standardized protocols.
Conclusion
4
Giant inguinoscrotal hernias (GIH) represent a significant surgical challenge, particularly in resource-constrained environments. Their classification into types based on the extent of hernia provides a structured approach to management, with Type I hernias requiring simpler interventions and Types II and III often demanding advanced techniques to mitigate risks like abdominal compartment syndrome (ACS). Strategies such as Preoperative Progressive Pneumoperitoneum (PPP), botulinum toxin injections, and component separation demonstrate the importance of individualized, resource-aware surgical planning.
This case highlights the intricate decision-making required in managing GIH, especially in the presence of uncommon anatomical anomalies like malrotation. Successful outcomes can be achieved even in complex cases by combining careful preoperative planning, innovative surgical approaches, and meticulous postoperative care. Addressing these challenges in resource-limited settings emphasizes the need for ongoing research and the development of standardized management protocols to improve care for patients with GIH worldwide.
Author contribution
All the authors in this work participated in the patient caring and treatment, conceptualization of the case report, drafted the manuscript, and reviewed the final version of the case report.
Ethical approval
Ethical approval for this study was obtained.
Guarantor
Dr. Hassan Sh. Abdirahman Elmi.
Consent for publication
After thoroughly explaining the study's purpose and implications, the patient provided informed consent.
Funding
No funding was received to conduct this study.
Declaration of competing interest
There are no conflicts of interest related to the publication of this article.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Hodgkinson D.J.Mc Ilrath D.C.Scrotal reconstruction for giant inguinal hernias Surg. Clin. North Am.642198430731310.1016/S 0039-6109(16)43287-16233734 · doi ↗ · pubmed ↗
- 2Gilbert A.I.Hernia 9Hernia 1999161166
- 3Coetzee E.Price C.Boutall A.Simple repair of a giant inguinoscrotal hernia Int. J. Surg. Case Rep.232011323510.1016/j.ijscr.2010.11.00522096682 PMC 3199728 · doi ↗ · pubmed ↗
- 4Khatiwada P.Living with a giant inguinoscrotal hernia for 35 years-a case report J. Surg. Case Reports 20211020211310.1093/jscr/rjab 458PMC 855742634729170 · doi ↗ · pubmed ↗
- 5Trakarnsagna A.Giant inguinal hernia: report of a case and reviews of surgical techniques Int. J. Surg. Case Rep.511201486887210.1016/j.ijscr.2014.10.04225462054 PMC 4245684 · doi ↗ · pubmed ↗
- 6Sohrabi C.Mathew G.Maria N.Kerwan A.Franchi T.Agha R.A.The SCARE 2023 guideline: updating consensus surgical C Ase R Eport (SCARE) guidelines Int. J. Surg.109520231136114010.1097/JS 9.000000000000037337013953 PMC 10389401 · doi ↗ · pubmed ↗
- 7Basukala S.Rijal S.Pathak B.D.Gupta R.K.Thapa N.Mishra R.Bilateral giant inguinoscrotal hernia: a case report Int. J. Surg. Case Rep.88, no. August 202110646710.1016/j.ijscr.2021.106467 PMC 852872834673470 · doi ↗ · pubmed ↗
- 8Wani I.Shah M.Malik A.Naqash S.Giant inguinal hernia: a case report Int. J. Case Reports Med.201320131510.5171/2013.692094 · doi ↗