Secondary Iron Overload Due to Amino Acid Chelated Iron Supplementation: A Case Report Involving a Mother and Daughter
Naomi Sugimori, Yoh Jinnouchi, Toru Mizoguchi

TL;DR
A mother and daughter developed iron overload from long-term use of amino acid chelated iron supplements, highlighting the need for caution and monitoring.
Contribution
This is the first reported case of secondary iron overload due to amino acid chelated iron supplementation.
Findings
Elevated ferritin levels and increased transferrin saturation were observed in both the mother and daughter.
MRI confirmed iron accumulation in the liver, spleen, and bone marrow in the daughter.
Discontinuation of the supplement and phlebotomy led to improvement in hematologic profiles.
Abstract
Amino acid chelated iron (bisglycinate chelate iron, Ferrochel) has been developed and used as a food fortifier to prevent and treat iron deficiency anemia. However, its long-term use has not been described and reports of iron overload are unavailable. We report a case of a mother and daughter who were diagnosed with iron overload based on blood sampling. Serum analysis revealed elevated ferritin levels and increased transferrin saturation (TSAT). MRI of the daughter showed iron accumulation in the liver, spleen, and bone marrow with normal inflammatory response and no findings suggestive of collagen disease or tumor, and she was diagnosed with secondary iron overload due to oral administration of an amino acid chelated iron preparation. After discontinuing over-the-counter medications and approximately two years of phlebotomy, the women showed a trend toward improvement in their…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
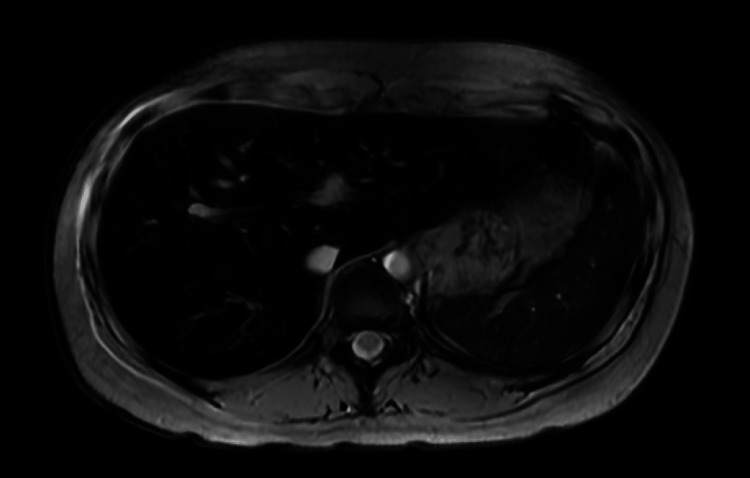 Figure 1
Figure 1| Variable | Normal value | Examination findings at the initial visit |
| April 202X | ||
| Hb (g/dL) | 11.5-16.0 | 14.9 |
| HCT (%) | 34.0-47.0 | 41.2 |
| MCV (fL) | 84-100 | 90.2 |
| MCH (pg) | 26-36 | 32.6 |
| MCHC (g/dL) | 32-36 | 36.2 |
| Fe (μg/dL) | 43-172 | 157 |
| TIBC (μg/dL) | 251-398 | 296 |
| Ferritin (ng/mL) | 5.0-177.6 | 2194.1 |
| TSAT (%) | 20-50 | 53 |
| AST (IU/L) | 12-31 | 28 |
| ALT (IU/L) | 8-40 | 37 |
| γGTP (IU/L) | 9-49 | 26 |
| Variable | Normal value | Examination findings at the initial visit |
| August 202X | ||
| Hb (g/dL) | 11.5-16.0 | 13.9 |
| HCT (%) | 34.0-47.0 | 40.7 |
| MCV (fL) | 84-100 | 90 |
| MCH (pg) | 26-36 | 30.8 |
| MCHC (g/dL) | 32-36 | 34.2 |
| Fe (μg/dL) | 43-172 | 104 |
| TIBC (μg/dL) | 251-398 | 299 |
| Ferritin (ng/mL) | 5.0-177.6 | 1691.1 |
| TSAT (%) | 20-50 | 35 |
| AST (IU/L) | 12-31 | 20 |
| ALT (IU/L) | 8-40 | 34 |
| γGTP (IU/L) | 9-49 | 53 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsIron Metabolism and Disorders · Hemoglobinopathies and Related Disorders · Trace Elements in Health
Introduction
Artificial iron pills have been developed to solve the global iron shortage and are widely available. However, their long-term use is still a matter of controversy. Amino acid chelated iron (bisglycinate chelate iron, Ferrochel) has been developed and used as a food fortifier to prevent and treat iron deficiency anemia, and it has been associated with minimal gastrointestinal symptoms and other side effects [1]. To date, most reports on the use of amino acid chelated iron have involved short-term clinical trials, with no reports on long-term use of more than a year.
The absorption of amino acid chelated iron is regulated by the amount of stored iron [2], and it has been speculated that iron overload does not occur in these instances; however, iron amino acid chelate preparations, which are thought to be absorbed via an amino acid transporter different from the absorption pathway of nonheme iron and heme iron, may cause iron overload [3]. We report the case of a 45-year-old mother and her 15-year-old daughter who developed iron overload after the intake of amino acid chelated iron preparations for more than a year.
Case presentation
Case 1
The patient was a 15-year-old female, diagnosed with a developmental disorder at seven years of age, and had a history of taking antipsychotics. She had started taking amino acid chelated iron at 12 years of age on the recommendation of her mother who had read in a book that “iron administration is effective for developmental disorders.” At 13 years of age, she had experienced an onset of nausea, leading her to take the supplement only occasionally, and she had eventually stopped taking it at 15 years of age due to stomatitis and swollen gums. Because her symptoms persisted, her mother took her to the Sugimori Clinic in April 202X and had a blood test, the results of which are presented in Table 1.
At the initial visit, the serum ferritin level was 2194 ng/mL, with a moderate increase and a transfer saturation (TSAT) of 53%. Liver MRI (Figure 1) showed iron accumulation in the liver, spleen, and bone marrow (radiology imaging at Kouseiren Takaoka Hospital); the inflammatory response [C reactive protein (CRP)] was normal; no findings suggestive of collagen disease or tumor were observed, and secondary iron overload due to oral administration of amino acid chelated iron preparations was diagnosed. Phlebotomy treatment of 100 mL was performed once a month, and the ferritin concentration dropped to 733.5 ng/mL in January 202X+2. Phlebotomy entails the removal of a certain amount of blood from a patient for therapeutic purposes. The nurse at the clinic manually performed the phlebotomy with a syringe, and considering the burden on the patient and the nurse, 100 ml of phlebotomy was given each time.
Liver MRIT2-weighted image: the liver and spleen are relatively more sensitive to magnetic substances such as iron in the tissues than the muscle and bone marrow. The diagnosis reached was iron overload secondary to the oral administration of amino acid chelated iron (bisglycinate chelate iron, Ferrochel)MRI: magnetic resonance imaging*
Case 2
This case involves the mother of Case 1: a 45-year-old woman. She had been diagnosed with hyperlipidemia and uterine fibroids at 25 and 35 years old, respectively. She had started taking 27 mg of the amino acid chelated iron twice daily at the same time as her daughter. The mother had excessive menstruation due to uterine fibroids, and hence she voluntarily took the iron supplement that her daughter was taking. She had not done a gynecologist test for anemia. She had become concerned while visiting the outpatient clinic with her daughter, leading her to visit the Sugimori Clinic in August 202X and undergo a blood test, although she was asymptomatic. Table 2 shows the initial laboratory findings.
Ferritin level was moderately elevated at 1691 ng/mL and TSAT was 35% in blood sampling at the initial visit. She was diagnosed with secondary iron overload due to intake of amino acid chelated iron preparations. Normally, treatment is carried out with drugs that bind to iron and excrete it from the body; however, due to side effects, the patient had to undergo phlebotomy. We also administered phlebotomy treatment once a month, and in July 202X+1, the ferritin level dropped to 518.1 ng/mL; phlebotomy was discontinued, and the patient was kept under observation.
Discussion
Iron overdose has been reported to occur even with the consumption of oral iron tablets [4]. Cases of suicides related to nonheme iron overdose [5], ferritin overdose, and chronic diarrhea have been reported [6]. While amino acid-chelated iron overdose has not been reported so far, overdose could occur with long-term use, such as in the cases presented here. Further experimental evaluation is needed to more comprehensively elucidate the mechanism of AA-/peptide-mediated iron absorption by iron glycine chelates [7]. One possible mechanism is that iron glycine chelates are not absorbed through the native physiological iron absorption pathways, such as DMT1 and HCP1. Although orally administered iron is originally shed from the tip of the small intestinal villi and excreted via the stool, iron amino acid chelates accumulate in the crypts of the small intestinal epithelium [3].
Conclusions
We reported two cases of iron overload in a mother and her daughter who were diagnosed using blood tests and MRI. Based on their medical history, the cause was thought to be the ingestion of an amino acid chelated iron supplement (bisglycinate chelate iron, Ferrochel). Chelated iron supplements carry a risk of iron overload, and ferritin levels should be checked in cases of long-term use. Iron overload can occur even in asymptomatic patients and can be dangerous if left untreated. Chelated iron glycinate should be administered as medicine, not as an iron supplement, and immediate action is needed in these cases.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1New insights into iron deficiency anemia in children: a practical review Metabolites Moscheo C Licciardello M Samperi P La Spina M Di Cataldo A Russo G 4612202210.3390/metabo 12040289 PMC 902907935448476 · doi ↗ · pubmed ↗
- 2Repleting hemoglobin in iron deficiency anemia in young children through liquid milk fortification with bioavailable iron amino acid chelate J Am Coll Nutr Iost C Name JJ Jeppsen RB Ashmead HD 187194171998955046310.1080/07315724.1998.10718745 · doi ↗ · pubmed ↗
- 3Intestinal Absorption of Metal Ions and Chelates Ashmead HD Graff DJ Ashmead HH Springfield, IL Charles C Thomas Publisher 1998 https://catalogue.nla.gov.au/catalog/1195433
- 4Iron overload due to excessive supplementation Handbook of Iron Overload Disorders Barton JC Edwards CQ Phatak PD Britton RS Bacon BR 313318 Cambridge, UK Cambridge University Press 42010 https://www.cambridge.org/core/books/abs/handbook-of-iron-overload-disorders/iron-overload-due-to-excessive-supplementation/9A 9988 B 2E 99E 082B 59473 DAAAC 5206 E 0
- 5Liver transplantation for acute hepatic failure following intentional iron overdose Cureus Eça R Ferreira S Gandara J Pessegueiro H Daniel J 015202310.7759/cureus.48392 PMC 1069986338060750 · doi ↗ · pubmed ↗
- 6Iron-storage disorder presenting as chronic diarrhea Cureus Vobugari N Kim J Gandhi KD Lee ZE Smith HP 013202110.7759/cureus.18864 PMC 859808334804717 · doi ↗ · pubmed ↗
- 7Oral iron therapy: current concepts and future prospects for improving efficacy and outcomes Br J Haematol Ebea-Ugwuanyi PO Vidyasagar S Connor JR Frazer DM Knutson MD Collins JF 75977320420243825396110.1111/bjh.19268 PMC 10939879 · doi ↗ · pubmed ↗