Mediation Effect of CSF Substance P on the Association Between Smoking and Sleep
Xie Zhang, Lingling Chen, Yuyu Wu, Yu‐Hsin Chen, Xingguang Luo, Zeping Xu, Weiming Hu, Yimin Kang, Li Chen, Yanlong Liu, Fan Wang, Danhui Liu

TL;DR
This study finds that smoking affects sleep quality through increased levels of Substance P in cerebrospinal fluid.
Contribution
It identifies Substance P as a mediator linking smoking to sleep disorders.
Findings
Active smokers had higher sleep disturbance scores and Substance P levels than nonsmokers.
Substance P levels negatively correlated with sleep quality in nonsmokers but not in smokers.
Substance P mediates the relationship between smoking and sleep regulation.
Abstract
Cigarette smoking has been linked to severe and persistent sleep disturbances alongside notable fluctuations in neuropeptide levels. Substance P (SubP), influenced by smoking, also impacts sleep‐wake cycles. However, its specific role in smoking‐induced sleep disorders remains unclear. This study aimed to explore the connection between cigarette smoking and sleep quality by examining SubP levels in cerebrospinal fluid (CSF) and identifying potential treatment avenues for sleep disorders. A total of 146 Chinese men (93 nonsmokers, 53 active smokers) undergoing lumbar puncture before anterior cruciate ligament reconstruction were enrolled. Clinical data and Pittsburgh Sleep Quality Index (PSQI) scores were assessed, followed by CSF sample collection and CSF SubP level measurement. Active smokers exhibited significantly higher PSQI scores (4.02 ± 2.27 vs. 2.60 ± 2.46, p < 0.001) and CSF…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
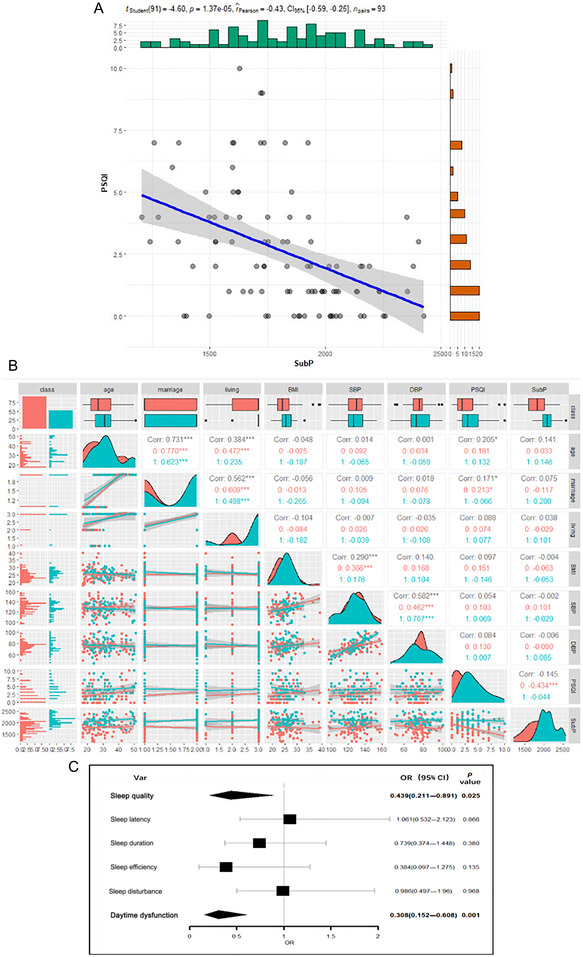 FIGURE 1
FIGURE 1 FIGURE 2
FIGURE 2| Variable | Nonsmokers | Active smokers |
|
|---|---|---|---|
| ( | ( | ||
| Age | 29 (9) | 32 (9) | 0.013 |
| BMI | 24.8 (4.1) | 25.6 (2.8) | 0.035 |
| SBP | 130 (13) | 126 (13) | 0.3 |
| DBP | 75 (9) | 76 (12) | 0.9 |
| SubP | 1821 (289) | 2111 (212) | <0.001 |
| PSQI Global Score | 2.60(2.46) | 4.02 (2.27) | <0.001 |
| PSQI component | No symptom/with symptom | No symptom/with symptom | |
| 1.Sleep quality | 53/40 | 19/34 | 0.014 |
| 2.Sleep latency | 69/24 | 19/34 | <0.001 |
| 3.Sleep duration | 45/48 | 27/26 | 0.8 |
| 4.Sleep efficiency | 86/7 | 47/6 | 0.5 |
| 5.Sleep disturbance | 59/34 | 10/43 | <0.001 |
| 6.Sleep medication | 89/4 | 52/1 | 0.7 |
| 7.Daytime dysfunction | 52/41 | 24/29 | 0.2 |
| Marriage | 0.011 | ||
| Married | 50 (54%) | 17 (32%) | |
| Unmarried | 43 (46%) | 36 (68%) | |
| Living | 0.002 | ||
| Alone or with family | 68 (73%) | 50 (94%) | |
| With others | 25 (27%) | 3 (5.7%) |
| Model1 (PSQI) | Model2 (SubP) | Model3 (PSQI) | ||||
|---|---|---|---|---|---|---|
|
|
|
|
|
|
| |
| Age | 0.161 | 1.372 | 0.159 | 1.467 | 0.219 | 1.966 |
| BMI | 0.082 | 1.018 | −0.052 | −0.694 | 0.063 | 0.828 |
| Marriage | −0.005 | −0.03 | −0.166 | −1.363 | −0.066 | −0.524 |
| Living | 0.023 | 0.24 | 0.038 | 0.421 | 0.037 | 0.406 |
| Smoke | 0.238 | 2.88 | 0.480 | 6.297 | 0.414 | 4.698 |
| SubP | — | — | — | — | −0.367 | −4.259 |
|
| 0.076 | 0.210 | 0.177 | |||
|
| 3.386 (5140) | 8.722 (5140) | 6.19 (6139) | |||
| Effect decomposition | Estimated | 95% CI |
| |
|---|---|---|---|---|
| Lower | Upper | |||
| Indirect effect | −0.176 | −0.267 | −0.091 | <0.001 |
| Direct effect | 0.414 | 0.242 | 0.583 | <0.001 |
| Total effect | 0.238 | 0.060 | 0.406 | 0.006 |
- —Beijing Natural Science Foundation 10.13039/501100004826
- —Technology Support Project of Xinjiang
- —Natural Science Foundation of Xinjiang Uygur Autonomous Region 10.13039/100009110
- —Outstanding Youth Science and Technology Talents of Xinjiang
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsSleep and Wakefulness Research · Neuropeptides and Animal Physiology · Neuroscience of respiration and sleep
Introduction
1
Cigarette smoking poses a significant global health threat, causing harm to nearly every organ in the body. It stands as the primary culprit behind over 30% of all cancer‐related deaths, 80% of chronic obstructive pulmonary disease fatalities, and a substantial portion of premature cardiovascular mortality (G. B. D. T. Collaborators 2017). Beyond its direct impact, smoking indirectly contributes to various health issues, including physical and mental distress, by disrupting sleep patterns among smokers (Liao et al. 2019; Liu et al. 2020). Extensive evidence from population‐based, laboratory, and clinical studies underscores the negative correlation between cigarette smoking and sleep quality in both adults and adolescents (Catoire et al. 2021; Hwang and Park 2022; Liu et al. 2020). These studies consistently reveal that smokers experience compromised sleep efficiency, reduced total sleep duration, disruptions in slow‐wave sleep, increased sleep onset latency, and other indicators of diminished sleep quality compared to nonsmokers (Catoire et al. 2021; Liao et al. 2019; McNamara et al. 2014). Additionally, smoking is associated with an elevated risk of developing various sleep disorders, such as restless legs syndrome, sleep apnea, and alterations in sleep architecture, further exacerbating health risks (Hwang and Park 2022; Liao et al. 2019). These sleep disturbances can have profound repercussions on individuals' well‐being, highlighting the urgent need to understand the relationship between smoking and sleep disorders and explore effective treatment options.
Smoking‐induced sleep disturbances are primarily attributed to the pharmacological effects of nicotine on brain neurotransmission (Branstetter, Krebs, and Muscat 2022; Leonel et al. 2020). Nicotine's activation of cholinergic receptors leads to the release of neurotransmitters, including dopamine, norepinephrine, serotonin, acetylcholine, and substance P (SubP) (Smith, Dwoskin, and Pauly 2010), all crucial for regulating sleep and wakefulness. SubP, an 11‐amino‐acid neuropeptide, exerts influence over sleep physiology (Hecht et al. 1980). It colocalizes with neurotransmitters in cells and brain regions implicated in sleep regulation, such as serotonin within the raphe nucleus, dopamine in the midbrain and striatum, and adrenocorticotropin‐releasing hormone within the hypothalamus (Otsuka and Yoshioka 1993; Sergeyev, Hokfelt, and Hurd 1999). Functioning through binding to neurokinin (NK) receptors, primarily NK‐1R, which are abundant in the human brain (Caberlotto et al. 2003), SubP is widely distributed in regions crucial for sleep regulation within the central nervous system (CNS), including the hypothalamus, brainstem, and cortex (Brown et al. 2012; Dam, Escher, and Quirion 1988). Laboratory experiments demonstrate that SubP administration enhances slow‐wave activity in mice and increases nonrapid eye movement sleep in rats (G. Zhang et al. 2004; Zielinski et al. 2015). Furthermore, low CSF SubP levels have been associated with anxiety and depression, closely linked to sleep problems (Carpenter et al. 2008). Despite these findings, the precise role and underlying mechanism of SubP in the sleep‐wakefulness cycle remain incompletely understood.
Our previous research indicated an association between smoking and elevated SubP levels in the cerebrospinal fluid (CSF) of active smokers (Wang et al. 2021). However, to date, no study has explored the relationship between smoking, CSF SubP levels, and sleep quality. In this study, we utilized the Chinese version of the Pittsburgh Sleep Quality Index (PSQI) to assess sleep quality, aiming to delineate the interplay among smoking, CSF SubP levels, and sleep, with the ultimate goal of identifying potent therapeutic strategies for addressing sleep disturbances.
Materials and Methods
2
Participants
2.1
A total of 146 Chinese adult males participated in this study, comprising 53 active smokers and 93 nonsmokers. Demographic information, including age, years of education, and body mass index (BMI), was recorded. Clinical data, such as history of substance abuse and dependence, were obtained via self‐report and corroborated by next of kin and family members. Exclusion criteria encompassed: (1) a familial history of neurological or psychiatric disorders; (2) diagnoses of systemic or CNS diseases according to the Mini International Neuropsychiatric Interview. The nonsmoking cohort consisted solely of individuals who had never smoked and had no history of substance abuse or dependence. Active smokers were defined as those consuming at least half a pack of cigarettes daily (equivalent to 10 cigarettes) for over a year, following the Diagnostic and Statistical Manual of Mental Disorders, 4th Edition. Smokers consuming fewer than 10 cigarettes per day were excluded. Participants with a history of alcoholism or psychiatric disorders were not included. Approval for the study was obtained from the Institutional Review Board of Inner Mongolian Medical University (YKD2014031) on March 11, 2014, adhering to the Declaration of Helsinki, with written informed consent obtained from all participants.
Assessments, Biological Sample Collection, and Laboratory Tests
2.2
Sleep quality was assessed using the Chinese version of the PSQI (Tsai et al. 2005), a widely utilized scale comprising 19 items. Each item is rated on a 4‐point Likert scale (ranging from 0 to 3), contributing to seven sub‐scales: subjective sleep quality, sleep latency, sleep duration, habitual sleep efficiency, sleep disturbances, use of sleep medication, and daytime dysfunction. Total scores range from 0 to 21, with higher scores indicating poorer sleep quality.
Lumbar puncture is routinely performed as part of the standard clinical procedure for patients undergoing anterior cruciate ligament reconstructive surgery in China, facilitating CSF sample collection with minimal disease entity interference. Smoking cessation prior to this procedure was not mandated. A licensed anesthetist conducted lumbar punctures in the morning before surgery using 3 mL of 0.5% ropivacaine for local anesthesia, and 5 mL CSF samples were obtained via intrathecal collection. Samples were promptly frozen at −80°C. The anterior cruciate ligament reconstruction procedure typically lasted less than 1 hour, with participants hospitalized for a maximum of 2 days before surgery. SubP levels in CSF were quantified using commercial radioimmunoassay kits from Phoenix (Phoenix Pharmaceuticals, Inc., Burlingame, CA, USA), following the manufacturer's instructions, with laboratory technicians blinded to clinical data.
Statistical Analysis
2.3
The normality of all variables was assessed using the Shapiro–Wilk test. Age, BMI, and SubP demonstrated nonnormal distributions (p < 0.05). Consequently, the Mann–Whitney rank‐sum test and independent t‐test were employed to compare differences in general demographic data, clinical data, and raw biomarkers between groups. Spearman correlation analysis was conducted to evaluate the relationship between SubP and PSQI scores. Linear regression analyses were then conducted to explore the mediating effect of SubP on PSQI scores, with gender, age, BMI, marital status, and living arrangements included as control variables. A mediation analysis was performed to elucidate whether SubP mediated the relationship between smoking and PSQI scores. Logistic regression was utilized to elucidate the relationship between the seven subdomains of PSQI and SubP in all participants. All statistical analyses were conducted using R Programming Language 4.2.0 and the R package (Bruce R). All tests were two‐sided, with the significance threshold set at p < 0.05.
Results
3
Sociodemographic and Clinical Characteristics
3.1
Table 1 presents the results. Age (29 ± 9 vs. 33 ± 9, p = 0.013), BMI (24.8 ± 4.1 vs. 25.6 ± 2.8, p = 0.035), SubP (1821 ± 298 vs. 2111 ± 212, p < 0.001), PSQI global score (2.60 ± 2.46 vs. 4.02 ± 2.27, p < 0.001), sleep quality (0.51 ± 0.64 vs. 0.72 ± 0.60, p = 0.028), sleep latency (0.32 ± 0.61 vs. 0.72 ± 0.63, p < 0.001), and sleep disturbance (0.40 ± 0.57 vs. 0.87 ± 0.48, p < 0.001) were significantly higher in the smoker group compared to the nonsmoker group. No significant differences were observed in other variables. Active smokers exhibited a significantly lower marriage rate (p = 0.011) and a higher rate of living alone or with family (p = 0.002) compared to nonsmokers.
Correlation Between SubP Levels and PSQI Scores
3.2
A negative correlation was observed between SubP and PSQI scores in all participants (r = −0.145, p < 0.001, see Figure 1A). Spearman's correlations revealed a consistent relationship between CSF SubP level and PSQI scores in nonsmokers (r = −0.434***, p < 0.001). Additionally, logistic regression analysis demonstrated significant associations between PSQI subgroups (sleep quality and daytime dysfunction) and CSF SubP level, with adjustments for age, education, and BMI (all p < 0.05, see Figure 1C).
*Correlation analysis between Substance P and PSQI scores. (A) Linear regression model was used to analyze the relationship between CSF SubP levels and PSQI scores in all participants. (B) Bivariate correlation matrix for the study variables in nonsmokers and active smokers using Spearman's rank correlation coefficients analysis. (C) SubP levels (divided into two groups by the median level) and six components of PSQI (yes/no) were included into the logistics regression model as dichotomous variables to assess the associations between the two. The linear regression and logistic regression models were adjusted for age, body mass index, marital status and living arrangement. Statistical significance (p < 0.05) was denoted in bold. p < 0.05. CI, confidence interval; OR, odds ratio; PSQI, Pittsburgh Sleep Quality Index; SubP, Substance P.
Mediation Analysis
3.3
To elucidate whether the relationship between smoking and PSQI scores is mediated by SubP, three separate mediation models were conducted. The mediation effect of SubP was confirmed in the association between smoking and PSQI scores (see Table 2 or 3 and Figure 2). Linear regression results showed a positive effect of smoking on PSQI scores (β = 0.238, t = 2.88, p < 0.01) after adjusting for age, BMI, marital status, and living arrangement. Similarly, a positive effect of smoking on CSF SubP level was observed. The addition of mediator variables demonstrated the mediating effect of CSF SubP level (β = −0.367, t = −4.259, p < 0.001).
*Effect decomposition of mediation models in PSQI scores. (A) Total effect between smoke and PSQI scores. (B) Effect decomposition of the mediation model for the relationship between smoke and PSQI scores association with CSF SubP levels as mediator. *p < 0.05, **p < 0.01, **p < 0.001. PSQI, Pittsburgh Sleep Quality Index; SubP, Substance P.
Bootstrap sampling revealed that smoking had a direct effect on PSQI scores (estimated = 0.414 (95% CI = 0.242–0.583), p < 0.001), as well as an indirect effect (estimated = −0.176 (95% CI = −0.267 to −0.091), p < 0.001), and total effect (estimated = 0.238 (95% CI = 0.060–0.406), p < 0.01). The mediating effect of CSF SubP level was found to be incomplete.
Discussion
4
In this study, we utilized human CSF SubP levels to examine the association between cigarette smoking and sleep quality. Our key finding reveals that smoking is indeed associated with impaired sleep quality, as evidenced by higher PSQI scores and elevated CSF SubP levels in active smokers compared to nonsmokers (see Table 1). These findings align with previous research demonstrating interactions between SubP and sleep disorders (Lieb et al. 2002; Ursavas et al. 2007; Zielinski et al. 2015), corroborating our observation of a negative correlation between CSF SubP levels and PSQI scores across all subjects. Furthermore, logistic regression analysis identified two PSQI subgroups (sleep quality and daytime dysfunction) significantly correlated with CSF SubP levels. Moreover, mediation analysis indicated that CSF SubP levels mediated the relationship between smoking and sleep quality, as measured by PSQI scores.
It is widely recognized that smoking significantly impacts sleep quality across various cohorts. Numerous studies have reported that smokers exhibit primary symptoms of insomnia, including decreased overall sleep duration, reduced sleep efficiency, prolonged sleep latency, diminished slow‐wave sleep, and increased daytime sleepiness (Cohrs et al. 2014; Jaehne et al. 2009; L. Zhang et al. 2006). Our findings align with these observations, demonstrating a correlation between smoking and higher PSQI scores indicative of poorer sleep quality. Nicotine in cigarettes can modulate sleep‐wake cycles by activating nicotinic receptors in crucial cholinergic circuits (Htoo et al. 2004) and dopaminergic neurons within the ventral tegmental area (Picciotto et al. 1998). Additionally, our study revealed significantly elevated CSF SubP levels in active smokers compared to nonsmokers (2111 ± 212 vs. 1821 ± 289, p < 0.001, see Table 1), consistent with our previous research (Wang et al. 2021). Previous studies have reported that chronic exposure to cigarette smoke upregulates SubP expression in CNS neurons (Canning and Spina 2009; De Swert et al. 2009). This phenomenon may be attributed to the inactivation of neutral endopeptidase by cigarette smoking, leading to reduced SubP degradation and subsequent elevation of SubP levels (Wong et al. 2004).
Additionally, our secondary finding suggests a potential negative correlation between CSF SubP levels and sleep quality assessed by PSQI scores in all participants (see Figure 1A), with sleep quality and daytime dysfunction emerging as two subgroups revealing significant differences (see Figure 1C). SubP is a well‐studied neuropeptide belonging to the tachykinins family and is widely distributed throughout the nervous system (Hidese et al. 2023). In the CNS, SubP is prominently found in regions such as the midbrain periaqueductal gray, nucleus raphe magnus, nucleus reticularis gigantocellularis pars α, posterior hypothalamus, basal forebrain, basal ganglia, nucleus accumbens, and cerebral cortex (Bright, Vink, and Byard 2018; Kaczyńska et al. 2018; Zieglgänsberger 2019). Consequently, SubP is intricately involved in regulating various physiological and pathophysiological processes, including sleep‐wake states (Bright, Vink, and Byard 2018; Kaczyńska et al. 2018; Zieglgänsberger 2019). Notably, the NK‐1 receptor (NK‐1R), to which SubP binds, is distributed widely across the brain, including areas crucially involved in sleep regulation, such as the hypothalamus, brainstem, and cortex (Brown et al. 2012; Dam, Escher, and Quirion 1988).
Several studies have reported the sleep‐promoting effects of SubP. For instance, research has shown a significant positive correlation between serum levels of SubP and slow‐wave sleep (Ursavas et al. 2007). Furthermore, studies utilizing NK‐1R antagonists have demonstrated an association between reduced SubP levels and augmented sleep (Kramer et al. 1998). Microinjection of SubP into the bilateral ventrolateral preoptic area in rats has been shown to enhance slow‐wave sleep (G. Zhang et al. 2004), while injection of SubP into the cortex of mice has potentiated slow‐wave activity (Zielinski et al. 2015). Additionally, SubP conjugated with cholera toxin A subunit has been found to increase nonrapid eye movement sleep slow‐wave activity (Zielinski and Gerashchenko 2017).
It is evident from our findings that smoking is associated with higher PSQI scores and CSF SubP levels, while higher CSF SubP levels are linked to lower PSQI scores. This raises the question: What is the actual relationship and interaction among smoking, CSF SubP levels, and sleep quality assessed by PSQI scores? Our results suggest that SubP might serve as a mediator in the process of smoking affecting PSQI scores (see Table 2 or 3 and Figure 2). One potential mechanism underlying SubP's mediation between smoking and sleep involves the influence of smoking on NK‐1R expression in the human brain. In the cerebral cortex, NK‐1R is exclusively expressed in type I nitric oxide synthase (nNOS) cells (Williams et al. 2019). Notably, type I nNOS cells play a pivotal role in linking homeostatic sleep drive with slow‐wave sleep (Dittrich et al. 2012) and have been identified as sleep‐active in mice (Pasumarthi, Gerashchenko, and Kilduff 2010). Moreover, research indicates that repeated and long‐term nicotine intake may elicit an augmentation in the synthesis or a diminution in the release of SubP via counteradaptations in opponent‐process dynamics (Pittenger et al. 2016). Likewise, smoking can up‐regulate NK‐1R expression in monocytes of healthy individuals (Amoruso et al. 2015). Thus, smoking may increase CSF SubP levels and NK‐1R expression, thereby activating type I nNOS cells, which in turn induce sleep.
In summary, our study suggests that cigarette smoking might potentially enhance SubP receptors, particularly NK‐1R, to influence sleep. However, the precise mechanisms underlying how smoking affects sleep, despite the mediation effect of CSF SubP levels, remain incompletely elucidated. Therefore, further investigation is necessary to better understand the mechanisms by which SubP modulates sleep‐wake behaviors in the context of smoking.
Several limitations in our study should be noted. Firstly, our reliance on subjective measures of sleep rather than objective assessments imposes certain constraints on the findings. Secondly, while CSF tissue analysis provides insights into biochemical changes, it does not directly assess neuronal functions in the brain. Thirdly, our study included patients with anterior cruciate ligament injuries rather than healthy individuals, potentially introducing confounding factors such as surgical stress that could affect biomarkers and sleep quality. Furthermore, the use of a cross‐sectional research design presents a fundamental methodological challenge, hindering the ability to derive causal inferences. Lastly, SubP seems to have a bidirectional function when it comes to regulating sleep (Shen et al. 2022), so there is a clear need for delving deeper into the mechanism of SubP mediating sleep in smokers and a larger sample size to effectively validate our results.
Conclusions
5
In conclusion, our study highlights the association between cigarette smoking, sleep disorders, and elevated SubP levels in the CSF of smokers compared to nonsmokers. Furthermore, SubP appears to play a mediating role in the relationship between smoking and sleep regulation, as evidenced by a negative correlation between CSF SubP levels and PSQI scores.
Author Contributions
Xie Zhang: writing–original draft. Lingling Chen: writing–original draft. Yuyu Wu: writing–original draft, data curation, formal analysis. Yu‐Hsin Chen: writing–original draft, methodology, project administration. Xingguang Luo: writing–review and editing. Zeping Xu: investigation. Weiming Hu: project administration, supervision. Yimin Kang: methodology, project administration, supervision. Li Chen: writing–original draft, methodology, project administration. Yanlong Liu: writing–review and editing, supervision, conceptualization. Fan Wang: writing–review and editing, resources. Danhui Liu: writing–review and editing, supervision.
Ethics Statement
Our study received ethical approval from the Institutional Review Board of Inner Mongolian Medical University (YKD2014031) on March 11, 2014. All participants provided their written informed consent to participate in this study and the consents were obtained from minors in addition to parental/guardian consent.
Conflicts of Interest
The authors declare no conflicts of interest.
Peer Review
The peer review history for this article is available at https://publons.com/publon/10.1002/brb3.70296.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Amoruso, A. , C. Bardelli , C. I. Cattaneo , L. G. Fresu , E. Manzetti , and S. Brunelleschi . 2015. “Neurokinin (NK)‐1 Receptor Expression in Monocytes From Bipolar Disorder Patients: A Pilot Study.” Journal of Affective Disorders 178: 188–192. 10.1016/j.jad.2015.03.013.25841180 · doi ↗ · pubmed ↗
- 2Branstetter, S. A. , N. M. Krebs , and J. E. Muscat . 2022. “Nighttime Waking to Smoke, Stress, and Nicotine Addiction.” Behavioral Sleep Medicine 20, no. 6: 706–715. 10.1080/15402002.2021.1992408.34666564 PMC 9016098 · doi ↗ · pubmed ↗
- 3Bright, F. M. , R. Vink , and R. W. Byard . 2018. “The Potential Role of Substance P in Brainstem Homeostatic Control in the Pathogenesis of Sudden Infant Death Syndrome (SIDS).” Neuropeptides 70: 1–8. 10.1016/j.npep.2018.02.006.29908886 · doi ↗ · pubmed ↗
- 4Brown, R. E. , R. Basheer , J. T. Mc Kenna , R. E. Strecker , and R. W. Mc Carley . 2012. “Control of Sleep and Wakefulness.” Physiological Reviews 92, no. 3: 1087–1187. 10.1152/physrev.00032.2011.22811426 PMC 3621793 · doi ↗ · pubmed ↗
- 5Caberlotto, L. , Y. L. Hurd , P. Murdock , et al. 2003. “Neurokinin 1 Receptor and Relative Abundance of the Short and Long Isoforms in the Human Brain.” European Journal of Neuroscience 17, no. 9: 1736–1746. 10.1046/j.1460-9568.2003.02600.x.12752772 · doi ↗ · pubmed ↗
- 6Canning, B. J. , and D. Spina . 2009. “Sensory Nerves and Airway Irritability.” Handbook of Experimental Pharmacology 194, no. 194: 139–183. 10.1007/978-3-540-79090-7_5.19655107 PMC 7120605 · doi ↗ · pubmed ↗
- 7Carpenter, L. L. , L. Bayat , F. Moreno , et al. 2008. “Decreased Cerebrospinal Fluid Concentrations of Substance P in Treatment‐Resistant Depression and Lack of Alteration After Acute Adjunct Vagus Nerve Stimulation Therapy.” Psychiatry Research 157, no. 1‐3: 123–129. 10.1016/j.psychres.2007.04.016.17976740 · doi ↗ · pubmed ↗
- 8Catoire, S. , M. Nourredine , S. Lefebvre , et al. 2021. “Tobacco‐Induced Sleep Disturbances: A Systematic Review and Meta‐Analysis.” Sleep Medicine Reviews 60: 101544. 10.1016/j.smrv.2021.101544.34597890 · doi ↗ · pubmed ↗