Heartfelt struggles: When ablation brings the squeeze
Hussam Al Hennawi, Alexander Shpilman

TL;DR
A 65-year-old patient developed chronic pericarditis after a heart procedure, highlighting the need for early detection of this rare but treatable complication.
Contribution
The paper emphasizes the importance of timely diagnosis of constrictive pericarditis following pulmonary vein isolation.
Findings
Chronic pericarditis can occur after pulmonary vein isolation for atrial fibrillation.
Prompt diagnosis of constrictive pericarditis is crucial for effective treatment.
The case illustrates the challenges in diagnosing this condition due to nonspecific symptoms.
Abstract
Pericarditis frequently occurs as a complication following pulmonary vein isolation (PVI) for atrial fibrillation (AF), yet it seldom progresses to constrictive pericarditis (CP). The diagnosis of constrictive pericarditis is often challenging owing to nonspecific signs and symptoms. Nevertheless, a high level of suspicion and prompt diagnosis offer an ultimate cure. We present a case of a 65-year-old patient who developed chronic pericarditis following PVI. This instance underscores the importance of promptly identifying this complication within this particular group of patients.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
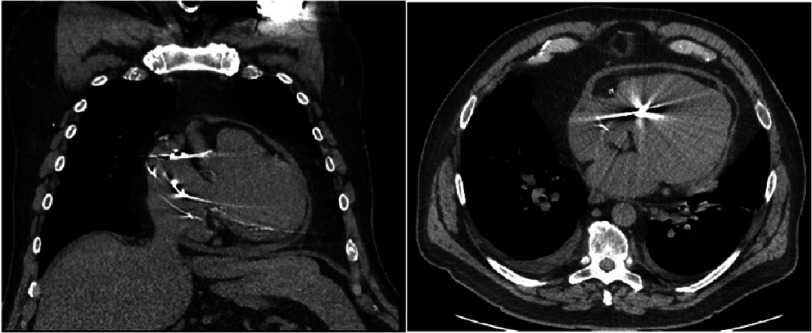 Figure 1
Figure 1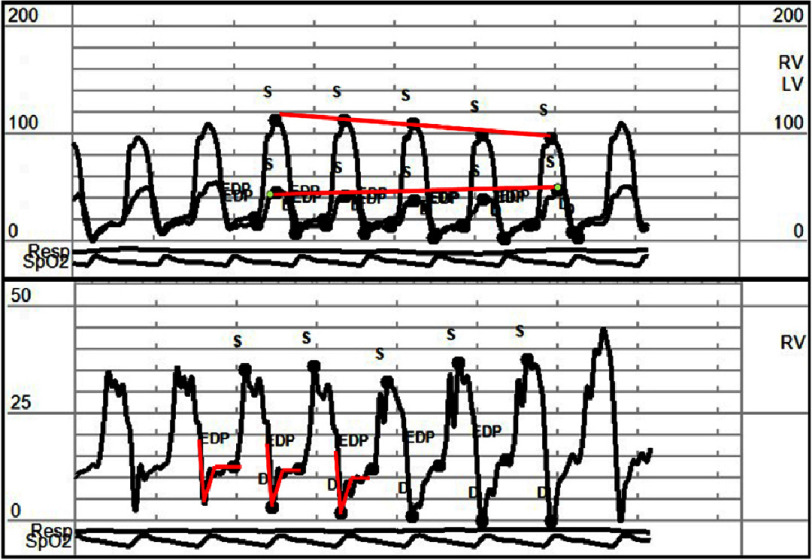 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPericarditis and Cardiac Tamponade · Cardiac tumors and thrombi · Cardiac Structural Anomalies and Repair
Case presentation
A 65-year-old male was evaluated for dyspnea on exertion and fatigue for four months. He had a history of chronic diastolic heart failure, long-standing persistent atrial fibrillation status post six catheter ablations, most recently 4 months before presentation, followed by cardiac resynchronization therapy and coronary artery disease status post percutaneous intervention, obstructive sleep apnea, hypertension, hyperlipidemia, and diabetes mellitus. Examination revealed jugular venous distention and trace bilateral lower extremity edema.
He was taking amlodipine 10 mg, atorvastatin 40 mg, bumetanide 1 mg twice daily, clopidogrel 75 mg, dapagliflozin 10 mg, metoprolol succinate 100 mg twice daily, and warfarin. Transthoracic echocardiogram showed markedly dilated LV with normal wall thickness and mild-moderately decreased systolic function (compared to echocardiogram prior to PVI) with regional variation and dyssynchrony of contractility, excessive respiratory phasic septal motion, and inferior vena cava appeared dilated with reduced inspiratory decrease. Computerized tomography showed a small pericardial effusion with a noncalcified thickened pericardium (Figure 1).
Computerized chest tomography showed a small pericardial effusion with a noncalcified thickened pericardium.
Right and left heart catheterization showed stable coronary artery disease and a pronounced x and y descent on right atrial tracing, equalization of diastolic pressures with dip and plateau sign (square root sign), and LV/RV pressure respirophasic discordance suggestive of constrictive pericarditis (Figure 2).
Right and left heart catheterization filling pressure curves show equalization of right and left ventricles, diastolic filling pressures, and a “dip and plateau” sign in the right ventricle pressure tracing (red square root sign).Solid lines show left and right ventricular pressure respirophasic discordance.
C-reactive protein was 3.97 mg/L (reference range 0.00–3 mg/L). Antinuclear antibody and Quantifieron-TB were negative. A diagnosis of chronic constrictive pericarditis was made. He was started on colchicine, but his symptoms did not improve significantly. Owing to persistent symptoms, he underwent pericardial stripping with a resolution of his symptoms.
Discussion
CP is a rare contributor to heart failure, marked by the heart being surrounded by a thickened, inflexible, and fibrous pericardium. This unyielding enclosure hampers the filling of the ventricles during relaxation (diastole) and leads to interdependence between the ventricles, culminating in reduced cardiac output^1^. Diagnosing CP can be challenging due to vague symptoms, contradictory test outcomes, and its gradual onset^2^.
Although recent literature emphasizes noninvasive multimodality imaging as essential for diagnosing CP, our experience suggests that it often falls short in atypical cases^3^. Therefore, a comprehensive evaluation should include invasive hemodynamic profiling via thorough left and right heart catheterization, which remains the gold standard. In the case under review, pressure waveform analysis supported a diagnosis of constrictive pathology, evidenced by a clear square root sign, complete diastolic pressure equalization, and ventricular interdependence with the characteristic respiratory discordance between left ventricular and right ventricular pressure waves^4^.
Given our patient complex history of uncontrolled atrial fibrillation for which he underwent multiple PVI, similar other case reports reported no major difference in terms of CP complication following atrial fibrillation ablation modalities, including radiofrequency ablation versus cryoablation^5–8^.
Our case highlights and emphasizes the course of a patient with suspected CP following PVI and encourages early consideration of pericarditis following atrial fibrillation ablation techniques.
What have we learned?
•Constrictive pericarditis is a rare complication following atrial fibrillation ablation. •Maintaining a low threshold for diagnosis is essential to ensure timely testing and early intervention.
Competing Interests
The authors have no competing interests to declare.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Mookadam F Jiamsripong P Raslan SF 2011 Constrictive pericarditis and restrictive cardiomyopathy in the modern era Future Cardiol 74714832179774410.2217/fca.11.18 · doi ↗ · pubmed ↗
- 2Welch T 2018 Constrictive pericarditis: diagnosis, management and clinical outcomes Heart 1047257312917597810.1136/heartjnl-2017-311683 · doi ↗ · pubmed ↗
- 3Mahmoud A Bansal M Sengupta P 2017 New cardiac imaging algorithms to diagnose constrictive pericarditis versus restrictive cardiomyopathy Curr Cardiol Rep 19432840593710.1007/s 11886-017-0851-0 · doi ↗ · pubmed ↗
- 4Geske J Anavekar N Nishimura R 2016 Differentiation of constriction and restriction: complex cardiovascular hemodynamics J Am Coll Cardiol 68232923472788425210.1016/j.jacc.2016.08.050 · doi ↗ · pubmed ↗
- 5Ahsan S Moon J Hayward M 2008 Constrictive pericarditis after catheter ablation for atrial fibrillation Circulation 118e 834e 8351906468710.1161/CIRCULATIONAHA.108.786541 · doi ↗ · pubmed ↗
- 6Javaheri A Glassberg H Acker M 2012 Constrictive pericarditis presenting as a late complication of epicardial ventricular tachycardia ablation Circ Heart Fail 5e 22e 232243852410.1161/CIRCHEARTFAILURE.111.965236 · doi ↗ · pubmed ↗
- 7Oesterle A Singh A Balkhy H 2016 Late presentation of constrictive pericarditis after limited epicardial ablation for inappropriate sinus tachycardia Heart Rhythm Case Rep 24414452849172910.1016/j.hrcr.2016.07.003PMC 5419970 · doi ↗ · pubmed ↗
- 8De Roeck F 2019 Constrictive pericarditis as late complication of cryoballoon pulmonary vein isolation Heart Rhythm Case Reports 613439 doi: 10.1016/j.hrcr.2019.10.01231956500 PMC 6962741 · doi ↗ · pubmed ↗