Clinical profile, management strategy, and outcomes of patients with prosthetic valve thrombosis
Waqar Khan, Arsalan Younus, Muhammad Imran Ansari, Jehangir Ali Shah, Mariam Naz, Raheela Khawaja, Aamir Khowaja, Taimur Asif Ali, Munawar Khursheed, Tahir Saghir

TL;DR
This study examines the treatment and outcomes of patients with prosthetic valve thrombosis, finding that most achieve success with therapies like streptokinase, but some face serious complications.
Contribution
The study provides a detailed analysis of treatment strategies and outcomes for prosthetic valve thrombosis in a clinical setting.
Findings
Streptokinase was the most common treatment, with 84% of patients achieving clinical success.
Severe complications like irreversible neurologic damage and bleeding occurred in 4.1% of cases.
The 30-day mortality rate was 12%, with recurring PVT and complications each affecting 1.5% of patients.
Abstract
Background: Prosthetic valve thrombosis (PVT) is a severe complication following prosthetic heart valve replacement, particularly in inadequately anticoagulated patients. Primary treatment options include intensive anticoagulation therapy, thrombolytic treatment (TT), and emergency surgery. This study aims to evaluate the clinical profile, management strategies, and short-term outcomes of patients with PVT. Methodology: Consecutive patients with PVT presenting to the emergency department of a tertiary care cardiac center were included in this study. Responses to treatment, hospital outcomes, and 30-day outcomes post-treatment were observed. Results: A total of 75 patients were analyzed, with a male predominance (50.7%) and a mean age of 39.5 ± 12.3 years. Bi-leaflet prosthetic valves were most common (96.0%), 54 (72.0%) had prosthetic mitral valve and 10 (13.3%) had prosthetic both…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
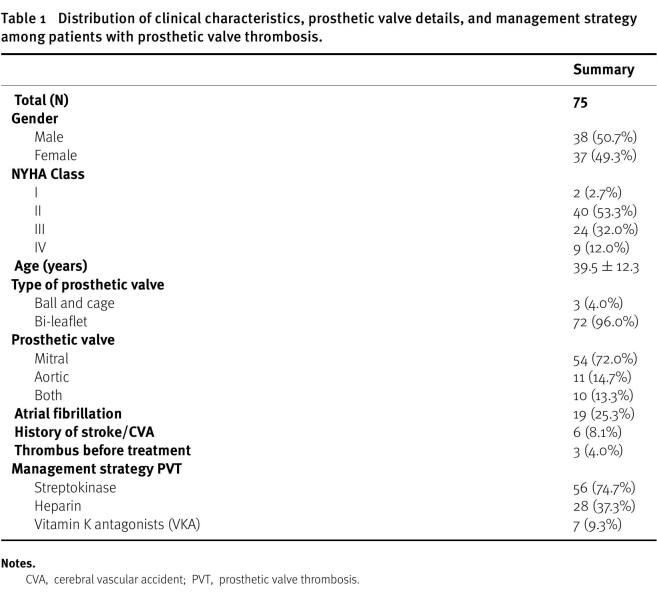 Figure 1
Figure 1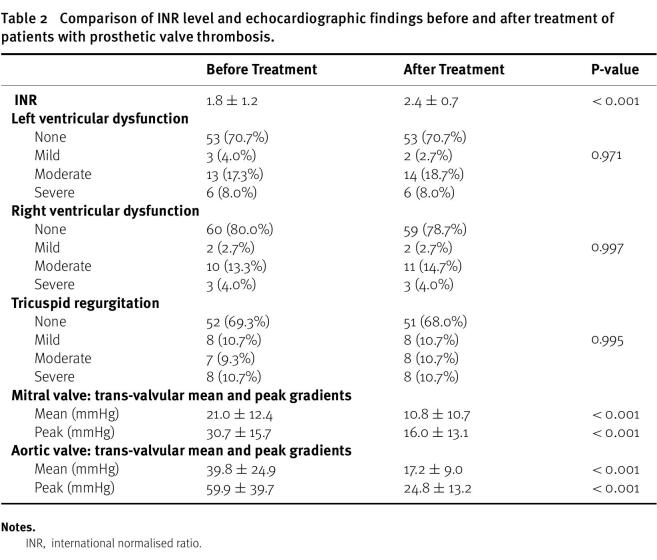 Figure 2
Figure 2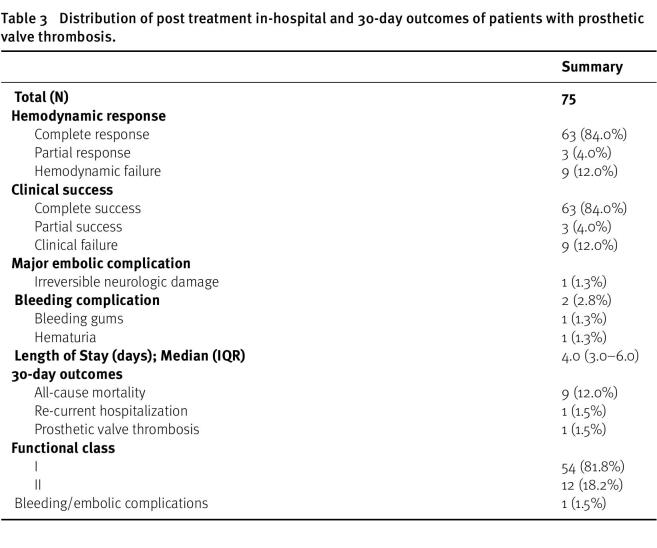 Figure 3
Figure 3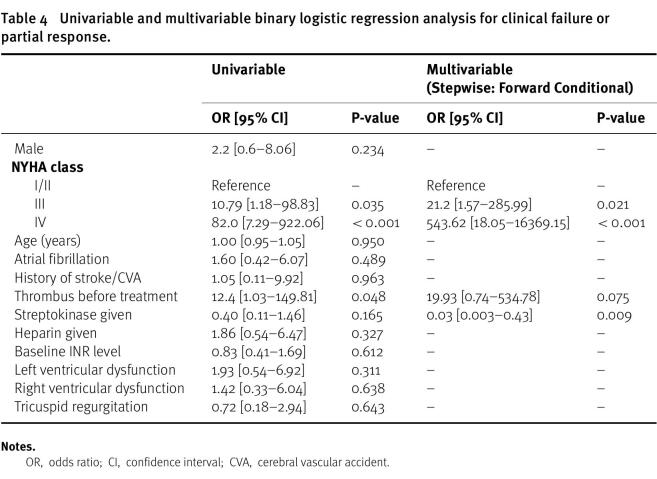 Figure 4
Figure 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCardiac Valve Diseases and Treatments · Infective Endocarditis Diagnosis and Management · Atrial Fibrillation Management and Outcomes
Introduction
The prevalence of valvular heart disease (VHD) varies globally, with rheumatic heart disease (RHD) affecting approximately 41 million individuals worldwide^1,2^. Calcific aortic valve disease (CAVD) has also become increasingly common, leading to rising incidence, prevalence, and mortality rates over the past three decades^3,4^. While non-rheumatic VHD has been steadily increasing, the occurrence of RHD has been on the decline^1,5^. Contributing factors include high systolic blood pressure, aging populations, and lifestyle choices such as smoking and alcohol consumption^3,6^.
For patients with severe native valvular heart disease, surgical replacement with mechanical or biological valves, as well as percutaneous valve implantation, are established gold standard therapies^7,8^. However, prosthetic heart valve replacement is not without its complications, both during and after the procedure. Despite the long-term durability of mechanical valves, valve malfunction remains a concern, with mechanical prosthetic valve thrombosis (PVT) being a particularly serious complication that can lead to rapid deterioration and compromise patient outcomes^9^.
PVT is an uncommon yet potentially life-threatening condition that can occur in any part of the heart valve prosthesis^10^. Although the exact incidence of valve thrombosis is uncertain, estimates suggest it ranges from 0.5% to 6% per patient per year in the aortic and mitral positions, and up to 20% in the tricuspid position^11^. Factors influencing PVT development include inadequate anticoagulant treatment, valve thrombogenicity, and hemodynamics of transprosthetic blood flow^12^. Despite advancements in surgical techniques, mechanical valves’ hemodynamic and physical properties still pose a risk for thrombus formation^13^.
While emergency surgery has been the traditional treatment for PVT, intravenous thrombolytic therapy has emerged as a viable alternative, showing excellent success rates and acceptable risks^14^. Current guidelines recommend either slow-infusion low-dose thrombolytic therapy (TT) or emergency surgery for PVT treatment^15^. In settings like Pakistan, where regular INR monitoring may be challenging due to geographic and financial constraints, thrombolytic therapy remains the primary treatment due to financial considerations. Therefore, this study aims to evaluate the clinical characteristics, management strategies, and short-term outcomes of patients presenting with prosthetic valve thrombosis at a tertiary care cardiac center’s emergency department.
Methodology
Study design: We conducted this prospective observational study at the emergency department of the largest tertiary care cardiac center in Karachi, Pakistan, the National Institute of Cardiovascular Diseases (NICVD). Our aim was to assess the clinical profile, opted management strategy, and in-hospital and 30-day outcomes of patients presenting with PVT. Data collection was carried out between November 22, 2021 and November 21, 2022.
Ethics: The study was conducted in accordance with the guidelines provided by the Declaration of Helsinki. Verbal consent for participation in the study was obtained from all participants prior to their inclusion. The study proposal was approved by the institution review board of the NICVD (ERC-119/2021).
Study population: The study population consisted of a consecutive sample of adult patients (≥ 18 years) of either gender who presented with PVT. Patients who declined consent for participation or those who left against medical advice (LAMA) were excluded from the analysis.
Data collection: Data for the study were collected using a predefined structured proforma. Collected data included demographic information such as age, gender, NYHA (New York Heart Association) class, and disease-related factors such as time since valve replacement, type of prosthetic valve, position of PVT, prosthesis size, atrial fibrillation, echocardiography parameters such as thrombus size, LV (left ventricular) dysfunction, RV (right ventricular) dysfunction, TR, trans-valvular gradient (mean/peak), and anticoagulation status. Additionally, data regarding the opted management strategy such as streptokinase, heparin, VKA, emergency surgery, and in-hospital outcomes of the patients such as hemodynamic response, clinical success, and incidence of any major embolic complication during hospital stay and post-discharge 30-day follow-up were also recorded.
Patients without contraindications for streptokinase received: loading dose of 250,000 International Units (IU) over 1 h and maintenance dose of 100,000 IU/hour via continuous infusion. For patients with contraindications to thrombolytic therapy, anticoagulation was initiated with heprin infusion with Targeted Partial Thromboplastin Time (PTT) of 1.5-2 times the upper normal range. PTT was repeated every 6 h.
At 24 h, a detailed echocardiogram, Hemodyanamic and clinical response was noted. Before discharge patient were bridged to warfarin and targeted INR achieved. Weekly INR monitoring was scheduled.
Variables and definitions: The hemodynamic response was categorized as follows: complete response - normalization of the trans-valvular mean and peak gradients (>75% reduction) on Doppler echocardiography and restoration of normal leaflet(s) motion on cine-fluoroscopy; partial response – 50–75% reduction in trans-valvular gradients with restricted movement of prosthetic valve leaflet(s) on cine-fluoroscopy, even if gradients decreased by more than 75%; hemodynamic failure – less than 50% reduction in trans-valvular gradients. Clinical success was categorized as follows: complete clinical success - complete hemodynamic response in the absence of any major complication; partial success - either complete or partial hemodynamic response and occurrence of any major hemorrhagic/embolic complication; clinical failure - either hemodynamic failure or occurrence of a complication resulting in death irrespective of the hemodynamic response. A major embolic complication was defined as one resulting in irreversible neurologic damage or myocardial infarction or one needing limb-salvage surgery.
Sample size: A total of 75 patients presenting to the emergency department with PVT during a 12-month study period were included in this study. The collected sample was deemed sufficient due to the exploratory nature of the analysis; however, no formal calculation of sample size was carried out.
Data Analysis: The collected data were summarized in accordance with the study objective. Appropriate summary measures such as mean ± standard deviation (SD) or median [interquartile range (IQR)] were computed for age, INR level, length of stay, and echocardiographic parameters. The distribution of various clinical and demographic variables along with outcome variables was expressed as percentages (%). Pre- and post-echocardiographic parameters were compared with paired sample t-test or Chi-square test, with the significance level set at p ≤ 0.05. The univariable and stepwise forward conditional multivariable binary logistic regression analysis was performed for clinical failure or partial response and odds ratio (OR) along with 95% confidence interval (CI) were computed.
Results
A total of 75 patients were included in this analysis; 38 (50.7%) were male, and the mean age was 39.5 ± 12.3 years. The type of prosthetic valve was bi-leaflet in 72 (96.0%) patients, with 54 (72.0%) having a prosthetic mitral valve and 10 (13.3%) having prosthetic valves in both the mitral and aortic positions. Atrial fibrillation was prevalent in 25.3% (19 patients), and 6 (8.1%) patients had a history of CVA/stroke. Among the patients, 56 (74.7%) were treated with streptokinase, 28 (37.3%) received heparin, and VKA was administered in 7 (9.3%) patients (Table 1).
Table 1: Distribution of clinical characteristics, prosthetic valve details, and management strategy among patients with prosthetic valve thrombosis.
The mean INR level increased from 1.8 ± 1.2 to 2.4 ± 0.7 ( p < 0.001) after treatment. Both the mean and peak trans-valvular gradients across the mitral valve decreased significantly from 21.0 ± 12.4 to 10.8 ± 10.7 (p < 0.001) and 30.7 ± 15.7 to 16.0 ± 13.1 (p < 0.001), respectively. Similarly, both the mean and peak trans-valvular gradients across the aortic valve decreased significantly from 39.8 ± 24.9 to 17.2 ± 9.0 (p < 0.001) and 59.9 ±39.7 to 24.8 ± 13.2 (p < 0.001) (Table 2).
Table 2: Comparison of INR level and echocardiographic findings before and after treatment of patients with prosthetic valve thrombosis.
Complete hemodynamic response was noted in 63 (84.0%) patients, while 9 (12.0%) patients experienced hemodynamic failure. Similarly, 63 (84.0%) patients achieved complete clinical success, whereas 9 (12.0%) patients encountered clinical failure, among whom one patient (1.3%) suffered irreversible neurologic damage, and 2 (2.8%) patients experienced bleeding complications. The 30-day mortality rate was 12.0% (9/75), with one patient experiencing PVT recurrence, one patient encountering PVT (1.5%), and one patient experiencing bleeding/embolic complications (1.5%) (Table 3).
Table 3: Distribution of post treatment in-hospital and 30-day outcomes of patients with prosthetic valve thrombosis.
The multivariable analysis revealed NYHA class III and IV were independently associated with higher risk of clinical failure or partial response with adjusted ORs of 21.2 [1.57–285.99] and 543.62 [18.05–16369.15], respectively. While, administration of Streptokinase was indendently associated with a lower risk of clinical failure or partial response with adjusted OR of 0.03 [0.003–0.43] (Table 4).
Table 4: Univariable and multivariable binary logistic regression analysis for clinical failure or partial response.
Discussion
The study examined the clinical characteristics, management approaches, and short-term outcomes of patients presenting with PVT following prosthetic heart valve replacement. Among the 75 patients analyzed, predominantly male with a mean age of 39.5 years, bi-leaflet prosthetic valves were most common, with the mitral valve being predominantly affected. A significant proportion of patients exhibited atrial fibrillation. Treatment predominantly comprised streptokinase, with notable success rates. A substantial proportion of patients (84.0%) achieved complete clinical success, underscoring the effectiveness of thrombolytic therapy. However, the study also revealed concerning outcomes, including clinical failure in 12.0% of patients, with one case resulting in irreversible neurologic damage. Additionally, bleeding complications were observed in a small percentage of patients. The success rate of 84% in our study aligns with the success rate reported by various studies. The reported success rate of thrombolytic therapy ranges from 65% to 92.4%^16–23^.
Moreover, the 30-day mortality rate of 12.0% underscores the gravity of PVT as a life-threatening complication, emphasizing the need for prompt and effective management strategies to improve patient outcomes. Furthermore, the recurrence of PVT and bleeding/embolic complications within the short follow-up period emphasize the necessity of long-term monitoring and comprehensive management strategies to mitigate the risk of recurrent events. These findings highlight the importance of balancing the benefits of thrombolytic and anticoagulant therapies with the potential risks of adverse events, particularly in patients with PVT. The recurrence of PVT after thrombolytic therapy remains an issue, with incidence varying from 16.2% to 31%^20,24,25^. In our study, we observed recurrence of PVT in 1 patient during the 30-day follow-up.
Similar to our study, Manandhar R et al.^26^ conducted a retrospective study of 45 cases presented to a cardiac center in Nepal over a period of 2 years. Atrial fibrillation was noted in 46.7%, and PVT was mostly at the mitral position (87%). A majority, 86.9%, were managed with thrombolysis, with streptokinase being the main treatment modality (86.9%), and in-hospital mortality was reported to be 13.3%, with no major bleeding or new stroke events. Hirachan A et al.^16^ reported suboptimal anticoagulation (INR < 1.5) in 69.6% of the case series of 23 patients with PVT. Thrombolysis, primarily with streptokinase, was administered to 86.9% of patients. Mitral valve thrombosis was most common (73.9%). In-hospital mortality occurred in 21.7% of cases, with no major bleeding events or new strokes noted.
Sharma V et al.^17^ concluded that thrombolysis is a reasonable option for PVT management, especially in cases of warfarin poor compliance and subtherapeutic INR. The study reported the efficacy of both tPA or SK with a success rate of 86.66% with tPA, while partial success and failure were observed in 17.77% and 6.66% respectively. For patients treated with streptokinase (n = 27), complete success was reported in 85.19%, with partial success and failure in 11.11% and 3.7% respectively. In another study from India by Kiran GR et al.^18^, the efficacy of streptokinase and tenecteplase for patients with PVT was compared. The complete hemodynamic response and complete clinical success were observed in 81% and 84.5% of the cases with 8.3% bleeding events and 4.7% embolic manifestations. However, tenecteplase was found to be associated with a lower complication rate. Continuing on the same premise, Kathirvel D et al.^21^ evaluated the efficacy and safety of tenecteplase and streptokinase for the treatment of PVT. Slow infusion of tenecteplase is equally efficacious but more effective than streptokinase in managing PVT with a complete success rate of 77.5% vs. 75%, respectively. However, minor bleeding (16.7% vs. 0%) was more common in tenecteplase compared to streptokinase, respectively. Hence, thrombolytic therapy should be considered as the first-line therapy when immediate surgical options are not feasible.
A study by Mahindru S et al.^19^ evaluated the midterm follow-up of patients with PVT (stuck valve), focusing on outcomes after thrombolysis. Thrombolysis was successful in 92.4% with a mortality rate of 7.57%. However, the 5-year mortality rate was found to be 22.95%. Milne O et al.^20^ conducted a retrospective case series of 21 patients with 32 episodes during a 17-year period at a cardiac center in the Northern Territory of Australia. The majority of patients presented with severe symptoms (NYHA class III and IV) and subtherapeutic anticoagulation (88%). Most valves were mechanical, with an average time from implantation to initial PVT of 5.1 years. Thrombolytic therapy was the main treatment approach (82% of episodes), achieving complete success in 65% and partial success in 19%. However, four patients did not respond to thrombolytic therapy, resulting in mortality or urgent transfer to a facility with cardiothoracic surgery capabilities. Overall mortality for the cohort was 24%, with thrombolytic therapy associated with major bleeding episodes in 16% of cases.
The low-dose and slow infusion thrombolytic therapy is a safe and effective management strategy in elderly patients with PVT. In a study by Gündüz S et al.^22^, this strategy has a cumulative success rate of 85.2%, with adverse events in 22.2% of patients. Higher thrombus burden and New York Heart Association class were predictive of adverse events, with the thrombus area being the only independent predictor. A study by Raman K et al.^27^ argued the effect of reoperation vs. thrombolysis on the long-term outcomes of patients with PVT. The reoperation was found to be advantageous over thrombolysis, with a significantly lower rate of embolism, bleeding events, re-intervention, as well as mortality at the end of 10-years follow-up.
The main factors influencing the development of PVT are inappropriate treatment by anticoagulants, thrombogenicity of the valve, and hemodynamics of the transprosthetic blood flow. A study by Bezanjani FN et al.^28^ reported several factors significantly associated with thrombosis included inadequate anticoagulation (INR < 2.5), a history of infection, prothrombin time check interval, atrial fibrillation rhythm, and plasma fibrinogen level.
It is important to acknowledge certain limitations of the study. It was conducted at a single tertiary care cardiac center and included a relatively small sample size of 75 patients. The study primarily focused on short-term outcomes up to 30 days post-treatment, which may not capture long-term complications or outcomes, limiting the comprehensive evaluation of treatment efficacy and safety over time. Finally, the study lacks a control or comparison group, making it challenging to assess the relative effectiveness of different treatment modalities or to compare outcomes with alternative management strategies. Hence we recommend prospective studies with larger sample size, longer follow-up period, and multi-center design to overcome the shortcoming of this study.
Conclusion
In conclusion, this study provides valuable insights into the clinical characteristics, management approaches, and short-term outcomes of patients presenting with PVT. While the majority of patients achieved successful outcomes with appropriate interventions, the study also highlights the challenges and potential complications associated with PVT management. Further research is warranted to elucidate optimal treatment strategies and long-term outcomes in this patient population.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Yu J Wang Z Bao Q Lei S You Y Yin Z Xie X 2022 Global burden of calcific aortic valve disease and attributable risk factors from 1990 to 2019 Front Cardiovasc Med 9doi: 10.3389/fcvm.2022.1003233100323336505369 PMC 9727398 · doi ↗ · pubmed ↗
- 2Aluru JS Barsouk A Saginala K Rawla P Barsouk A 2022 Valvular Heart Disease Epidemiology Med Sci (Basel)10232 doi: 10.3390/medsci 1002003235736352 PMC 9228968 · doi ↗ · pubmed ↗
- 3Zheng X Guan Q Lin X 2023 Changing trends of the disease burden of non-rheumatic valvular heart disease in China from 1990 to 2019 and its predictions: Findings from global burden of disease study Front Cardiovasc Med 9912661 doi: 10.3389/fcvm.2022.91266136741848 PMC 9897059 · doi ↗ · pubmed ↗
- 4Yi B Zeng W Lv L Hua P 2021 Changing epidemiology of calcific aortic valve disease: 30-year trends of incidence, prevalence, and deaths across 204 countries and territories Aging (Albany NY)1391271012732 doi: 10.18632/aging.20294233973531 PMC 8148466 · doi ↗ · pubmed ↗
- 5Santangelo G Bursi F Faggiano A Moscardelli S Simeoli PS Guazzi M Lorusso R Carugo S Faggiano P 2023 The Global Burden of Valvular Heart Disease: From Clinical Epidemiology to Management J Clin Med 1262178 doi: 10.3390/jcm 1206217836983180 PMC 10054046 · doi ↗ · pubmed ↗
- 6Chen J Li W Xiang M 2020 Burden of valvular heart disease, 1990-2017: Results from the Global Burden of Disease Study 2017 J Glob Health 102doi: 10.7189/jogh.10.02040402040433110570 PMC 7568921 · doi ↗ · pubmed ↗
- 7Writing Committee Members Otto CM Nishimura RA Bonow RO Carabello BA Erwin 3rd JP Gentile F Jneid H Krieger EV Mack M Mc Leod C O’Gara PT Rigolin VH Sundt 3rd TM Thompson A Toly C 20212020 ACC/AHA Guideline for the Management of Patients with Valvular Heart Disease: Executive Summary: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines J Am Coll Cardiol 774450500 doi: 10.1016/j.jacc.2020.11.03533342587 · doi ↗ · pubmed ↗
- 8Falk V Baumgartner H Bax JJ De Bonis M Hamm C Holm PJ Iung B Lancellotti P Lansac E Muñoz DR Rosenhek R Sjögren J Tornos Mas P Vahanian A Walther T Wendler O Windecker S Zamorano JL ESC Scientific Document Group 20172017 ESC/EACTS Guidelines for the management of valvular heart disease Eur J Cardiothorac Surg 524616664 doi: 10.1093/ejcts/ezx 32429156023 · doi ↗ · pubmed ↗