Usefulness of Glucose Monitoring in Neonates of Mothers With an Elevated Glucose Challenge Test and a Normal Oral Glucose Tolerance Test
Margaret A Uchefuna, Giddel Alvarado, Imoh L Ebong, Saman Aryal, Sheng-Hsin Chen, Alexander Rodriguez

TL;DR
This study examines whether glucose monitoring is useful for neonates whose mothers had an elevated glucose challenge test but normal oral glucose tolerance test, finding that hypoglycemia is rare in these infants.
Contribution
The study provides new evidence on neonatal hypoglycemia risk in infants of mothers with elevated GCT but normal OGTT, suggesting limited need for glucose monitoring in this group.
Findings
Only 8 out of 63 neonates had asymptomatic hypoglycemia.
Hypoglycemia resolved with oral feed or glucose gel and did not require NICU admission.
No significant correlation was found between maternal GCT and neonatal glucose levels.
Abstract
Background Neonatal hypoglycemia is a common metabolic disturbance in neonates. Glucose monitoring is recommended for certain groups of neonates, including those whose mothers have pre-gestational or gestational diabetes. Little is known about the relevance of glucose monitoring in neonates whose mothers have an elevated screening glucose challenge test (GCT) but a normal oral glucose tolerance test (OGTT). Objectives The objectives of this study were to determine if neonates of mothers with an elevated GCT but a normal OGTT had hypoglycemia and to establish if there was an association between the maternal GCT and neonatal blood glucose level. Methods A single-site retrospective analysis was conducted on 307 neonates born in a community hospital in the Brooklyn area of New York between November 1, 2021, and November 1, 2023, who were identified as being at risk for hypoglycemia due…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
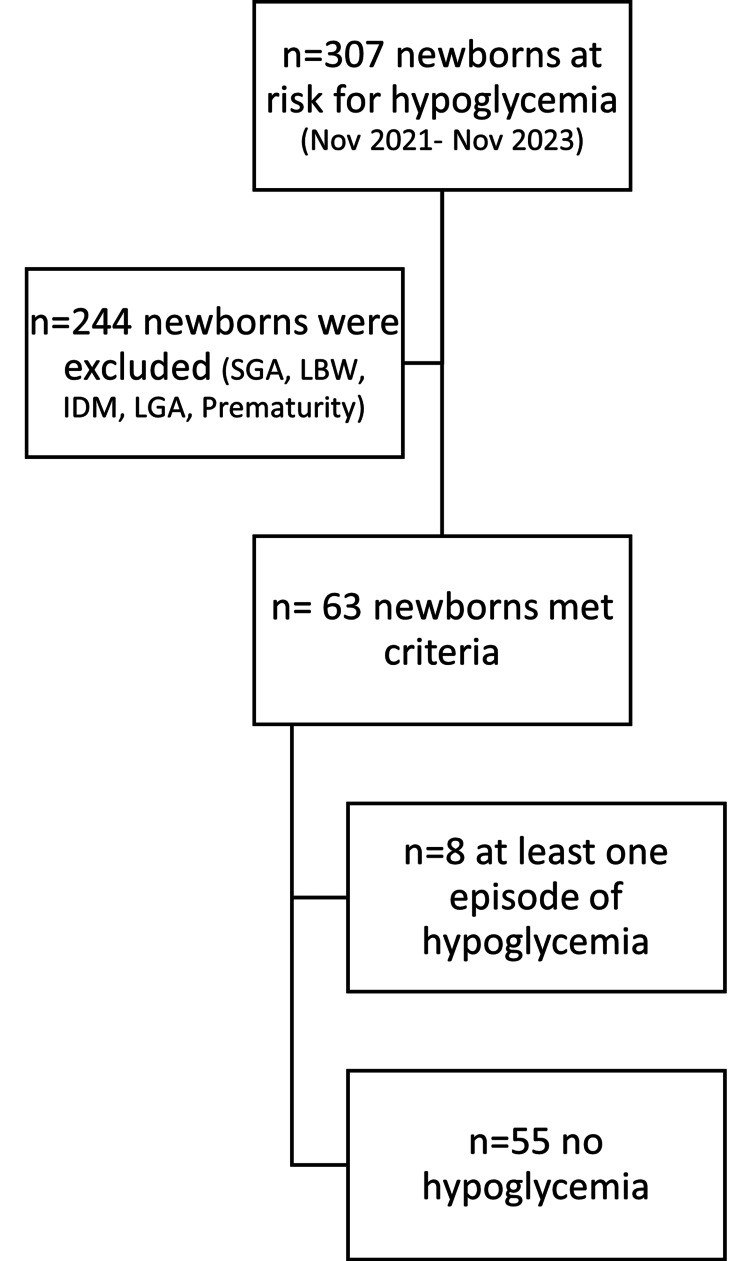 Figure 1
Figure 1| Variable | Frequency | Percentage | |
| Gender | |||
| Female | 32 | 50.8% | |
| Male | 31 | 49.2% | |
| Total | 63 | 100.0% | |
| Race/Ethnicity | |||
| Black/African American | 7 | 11.1% | |
| Hispanic/Latinx | 41 | 65.1% | |
| Jewish | 1 | 1.6% | |
| Not Hispanic | 3 | 4.8% | |
| Asian | 1 | 1.6% | |
| Russian | 4 | 6.3% | |
| White | 1 | 1.6% | |
| Unspecified/Unknown/Missing | 5 | 7.9% | |
| Total | 63 | 100.0% | |
| Hypoglycemia | |||
| Negative | 55 | 87.3% | |
| Positive | 8 | 12.7% | |
| Total | 63 | 100.0% | |
| Maternal GTT | |||
| Normal | 63 | 100% | |
| Missing | 0 | 0% | |
| Total | 63 | 100% | |
| Maternal HbA1c | |||
| Normal | 49 | 77.8% | |
| Elevated | 8 | 12.7% | |
| Missing | 6 | 9.5% | |
| Total | 63 | 100.0% | |
| Variable | Mean | Standard Deviation |
| Birthweight (in grams) | 3,212.40 | 375.65 |
| Gestational age (in weeks) | 39.20 | 1.17 |
| Maternal age (in years) | 30.65 | 6.34 |
| Maternal GCT | 156.78 | 22.08 |
| Test variable | Hypoglycemic Reaction | Mean | SD | T | P |
| Birthweight | Negative | 3,250.80 | 388.79 | ||
| Positive | 3,184.63 | 281.73 | 0.463 | NS | |
| Maternal GCT | Negative | 156.11 | 21.23 | ||
| Positive | 161.38 | 28.51 | -0.627 | NS | |
| Gestational age | Negative | 39.13 | 1.16 | ||
| Positive | 39.70 | 1.21 | -1.278 | NS |
| Pearson Correlation | P | |
| Correlation between maternal GCT and Initial glucose reading | -0.173 | NS |
| Correlation between maternal GCT and lowest glucose reading | -0.182 | NS |
| Correlation between initial and lowest glucose readings | 0.719 | <0.001 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGestational Diabetes Research and Management · Hyperglycemia and glycemic control in critically ill and hospitalized patients · Diabetes Management and Research
Introduction
Hypoglycemia is one of the most frequent metabolic imbalances that occur in neonates [1] and is a common reason for neonatal hospitalizations worldwide [2]. It affects approximately 5-15% of otherwise healthy neonates [3].
In utero, the fetus does not generate glucose within its body but relies entirely on maternal glucose obtained through the placental connection. The process of building glycogen stores through glycogenesis occurs slowly in the fetus in the early weeks of pregnancy but gradually increases towards term. At birth, the clamping of the cord disrupts glucose supply to the neonate, and hormone levels rise in an attempt to mobilize glucose through glycogenolysis and gluconeogenesis. This process may take a while which explains why healthy neonates usually experience a period of transitional hypoglycemia during the first 2-3 hours after birth [4]. The inability to normalize blood glucose levels over time poses risks for neurological complications like mental retardation, epilepsy, cardiac issues, and muscle weakness [5].
The American Academy of Pediatrics (AAP) defines neonatal hypoglycemia as blood glucose levels below specific thresholds, 40 mg/dL within the first four hours of life and 45 mg/dL between 4 and 24 hours of life and recommends screening glucose checks for certain groups of neonates who, based on different mechanisms, are at risk for hypoglycemia [6]. This includes neonates who are born late preterm, small or large for gestational age, or whose mothers have pre-gestational or gestational diabetic mothers.
Gestational diabetes mellitus (GDM) is the onset of diabetes during pregnancy, in women who did not have diabetes pre-pregnancy. In a recent meta-analysis, the global prevalence was found to be 4.4%, higher in the US and Canada compared to Europe [7]. According to the American Diabetes Association, the evaluation of gestational diabetes involves a two-step approach. Initially, a non-fasting glucose challenge test (GCT) is performed between 24 and 28 weeks of pregnancy. An elevated test result defined by a one-hour random glucose equal to or greater than 135 mg/dl after ingesting a 50-g glucose load is followed by a confirmatory fasting oral glucose tolerance test (OGTT) which entails drinking a 100-g glucose load. Gestational diabetes is diagnosed when two or more values from the OGTT are elevated above certain cut-offs based on widely accepted criteria [8]. For our study, we used the Carpenter-Coustan criteria, in keeping with our hospital's guidelines, to identify an abnormal OGTT, with values defined as elevated if they were equal to or greater than 95 mg/dL for fasting glucose, 180 mg/dL for one-hour glucose, 155 mg/dL for two-hour glucose and 140 mg/dL for three-hour glucose [9].
In some mothers, the elevated screening GCT is followed by a normal OGTT, creating a gray area in some centers as to whether glucose monitoring is required in the neonate, or not. Our study aimed to assess the usefulness of glucose monitoring in asymptomatic neonates born to mothers with elevated GCTs but normal OGTT results.
Materials and methods
A single-site retrospective analysis was conducted on 307 neonates born in a community hospital (Woodhull Medical Center) in the Brooklyn area of New York between November 1, 2021, and November 1, 2023, who were identified as being at risk for hypoglycemia due to known risk factors like maternal diabetes, prematurity, low birth weight, small or large size for gestational age, as well as possible risk factors like an elevated maternal GCT but a normal OGTT. Glucose monitoring had been done for these neonates at birth per AAP recommendations. The Office of Science and Research Institutional Review Board reviewed the study which was determined to meet the criteria for exemption. The individual authorization requirements were waived and adequate steps were taken to ensure data privacy.
Neonates of diabetic mothers or mothers with elevated OGTT and neonates who were born preterm, low birth weight, small or large for gestational age were excluded from the study while neonates whose mothers had an elevated GCT but a normal OGTT were included. This brought to 63 the number of neonates who met the inclusion criteria (Figure 1).
Chart review methodologySGA: small for gestational age, LBW: low birth weight, IDM: infants of diabetic mothers, LGA: large for gestational age
An elevated non-fasting 50-g, one-hour GCT was plasma glucose ≥ 135 mg/dl (defined by the American College of Obstetricians and Gynecologists criteria for areas with a high prevalence of GDM). The charts of neonates who met the inclusion criteria were reviewed to see if they had hypoglycemia at the time of glucose monitoring during hospital stay. Neonatal hypoglycemia was defined as capillary blood glucose level <40 mg/dl between 0 and 4 hours of life and < 45 mg/dl between 4 and 24 hours of life [6].
For statistical processing, the chi-square test was used for categorical variables and the two-sample t-test was used for continuous variables. Multiple logistic regression analysis was performed to estimate the odds ratio (ORs) of adverse outcomes with adjustment for confounders. Statistical analysis was performed using Statistical Analysis System (SAS) version 9.2 (SAS Institute, Inc., Cary, NC).
Results
A sample of 63 women and their neonates were included in the final analysis. The women were of diverse ethnicity although 41 (65.1%) identified primarily as Hispanic or Latinx. The average age of the women was 30.65 years (SD = 6.34 years). All the GCT results were elevated with an average of 156.78 mg/dl (SD = 22.08), while the OGTT results were in the normal range, per study protocol. More than three-quarters of the mothers’ hemoglobin A1c readings were in the normal range while 8 mothers (12.7%) had elevated readings. The male-to-female ratio was approximately 1:1, the average birthweight was 3,212.40 grams (SD = 375.65 grams) and the average gestational age was 39.20 weeks (SD = 1.17 weeks). Fifty-five (87.3%) of the 63 neonates had no hypoglycemia, while 8 (12.7%) had hypoglycemia (see Tables 1, 2).
Of the eight babies with hypoglycemia, two babies (25%) had one hypoglycemic value each, four babies (50%) had two hypoglycemic values each, and two babies (25%) had three hypoglycemic values each. Thus, 16 hypoglycemic readings were distributed among the eight babies, with two (12.5%) occurring before four hours of life and 14 (87.5%) between 4 and 24 hours of life. The average initial glucose reading was 64.83 mg/dl (SD=18.74), and the average lowest glucose reading of the babies was 53.50 mg/dl (SD=10.57). All the neonates with hypoglycemia were identified within the first three glucose measurements, per the AAP hypoglycemia screening protocol.
In the next set of analyses, we tested to determine if there were differences in birthweight, maternal GCT, and gestational age as a function of hypoglycemia in the neonate. Independent t-test analyses demonstrated no relationship between neonatal hypoglycemia and birthweight, maternal GCT, or gestational age (see Table 3).
Our study also found no correlation between elevated maternal GCT (in the setting of normal OGTT) and neonatal hypoglycemia (see Table 4).
Discussion
Most babies with hypoglycemia are asymptomatic which is where the real concern lies as subtle neurological damage may occur before symptoms become evident [10]. The symptoms of hypoglycemia are non-specific and include apnea, jitteriness, irritability, poor feeding, poor tone, hypothermia, and seizures. Treatment interventions for hypoglycemia are recommended parenterally for all symptomatic neonates and when oral supplementation fails for asymptomatic neonates whose blood glucose levels fall below the defined cut-offs per hour of life, as stated by current guidelines [6].
A 2024 publication by Andrews et al. concluded that neonates whose mothers had an abnormal glucose screen test (even if the confirmatory OGTT was unremarkable) were more likely to have hypoglycemia when compared to those whose mothers had a normal glucose screen [11]. This was similar to other studies [12,13] in similar settings which showed a more frequent occurrence of hypoglycemia. Our study found an average hypoglycemic value of 37.5 mg/dl within four hours of life and 40 mg/dl between 4 and 24 hours of life, and none of the neonates was symptomatic.
Women with elevated glucose screening tests were also found more likely to have newborns who were larger in size for gestational age and required cesarean section or assisted delivery and this occurred despite subsequent normalization of maternal glucose values [14-17]. The babies in our study had no significant difference in birth weight as a function of hypoglycemia.
Early pregnancy causes a hormonal surge which leads to insulin resistance; some studies have shown the insulin-resistant states of gestational hyperglycemia to be associated with worse neonatal outcomes and greater need for neonatal ICU admissions when compared to insulin-deficient states [16]. None of the hypoglycemic neonates in our study required IV fluids or neonatal ICU admission as there was resolution of hypoglycemia with oral feed, oral glucose gel, or a combination of both.
Other negative perinatal outcomes like hyperbilirubinemia, birth trauma, and stillbirth have also been found to occur in neonates of women with impaired glucose tolerance of any form [12,13]. This finding is relatable to several other studies that have shown an increased risk for untoward outcomes in neonates of women with impaired glucose tolerance of any form [18-20]. In contrast, a remarkably decreased incidence of low blood glucose was seen in a study by Wang et al. [21] of neonates whose mothers had impaired glucose tolerance when compared to those whose mothers had gestational diabetes mellitus.
Our study showed a 1:1 ratio in gender distribution among the neonates with hypoglycemia and no significant relationship was found between gender and hypoglycemic reaction (X2 = 0.002). Although no correlation was seen between elevated maternal GCT (in the setting of normal OGTT) and neonatal hypoglycemia, the mean difference between the initial and lowest glucose values was found to be statistically significant (t=6.812, p<0.001). This great variability in readings following the initial test shows that although the first glucose check may be normal, subsequent checks can still be low which signals the need for serial glucose checks in those neonates who require glucose monitoring until they are able to fully establish their own glucose homeostasis. There is yet no consensus on whether elevated maternal GCT with subsequent normal maternal OGTT is a risk factor for neonatal hypoglycemia, or whether glucose monitoring is beneficial in neonates of such mothers. Our study helped provide additional research data that supports the idea that there may be a need to monitor glucose levels in this group.
In addition, we found that eight (12.7%) out of the 63 mothers had an elevated hemoglobin A1c (hbA1c). Interestingly, all the mothers of the babies with hypoglycemia had normal hbA1c, and we saw no relationship between the hypoglycemic reaction (X2 = 0.927) and hemoglobin A1c in the mothers who had elevated GCT but normal OGTT. Our study demonstrated no significant relationship between elevated maternal GCT (if OGTT is normal) and neonatal hypoglycemia and a relationship of great significance between the mean initial and lowest glucose values. However, our study was limited by its small sample size and the lack of a comparison group.
Conclusions
Hypoglycemia is a common metabolic problem in neonates and can manifest very subtly. With changes in diet and an increase in the prevalence of mothers with elevated GCTs with or without gestational diabetes, more neonates may be at risk.
Our study demonstrated that the likelihood of hypoglycemia in neonates of mothers with an abnormal GCT but a normal glucose tolerance test was slim. Further studies are needed, and a larger group size would be of benefit.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Admissions of Term Newborn Infants for Hypoglycaemia: Their Characteristics and Preventability Deshpande S Upton M Hawdon J Edinburgh, UK The Neonatal Society 2016 https://www.neonatalsociety.ac.uk/2016/06/24/admissions-of-term-newborn-infants-for-hypoglycaemia-their-characteristics-and-preventability/
- 2Controversies regarding definition of neonatal hypoglycemia: suggested operational thresholds Pediatrics Cornblath M Hawdon JM Williams AF Aynsley-Green A Ward-Platt MP Schwartz R Kalhan SC 1141114510520001079047610.1542/peds.105.5.1141 · doi ↗ · pubmed ↗
- 3Re-evaluating "transitional neonatal hypoglycemia": mechanism and implications for management J Pediatr Stanley CA Rozance PJ Thornton PS 1520152516620152581917310.1016/j.jpeds.2015.02.045PMC 4659381 · doi ↗ · pubmed ↗
- 4Postnatal glucose homeostasis in late-preterm and term infants Pediatrics Adamkin DH 57557912720112135734610.1542/peds.2010-3851 · doi ↗ · pubmed ↗
- 5Brain injury in neonatal hypoglycemia: a hospital-based cohort study Clin Med Insights Pediatr Gu MH Amanda F Yuan TM 13201910.1177/1179556519867953 PMC 668813631447599 · doi ↗ · pubmed ↗
- 6Hierarchy of glycemic thresholds for counterregulatory hormone secretion, symptoms, and cerebral dysfunction Am J Physiol Mitrakou A Ryan C Veneman T 074260199110.1152/ajpendo.1991.260.1.E 671987794 · doi ↗ · pubmed ↗
- 7Neonatal hypoglycemia Stat Pearls [Internet] Abramowski A Ward R Hamdan AH Treasure Island (FL)Stat Pearls Publishing 2023 https://pubmed.ncbi.nlm.nih.gov/30725790/30725790 · pubmed ↗
- 8Prevalence of gestational diabetes in the United States and Canada: a systematic review and meta-analysis BMC Pregnancy Childbirth Eades CE Burrows KA Andreeva R Stansfield DR Evans JM 2042420243849149710.1186/s 12884-024-06378-2PMC 10941381 · doi ↗ · pubmed ↗